Apocrine Sweat Retention in Man I
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
An Introduction to the Integumentary System
An Introduction to the Integumentary System • Learning Outcomes • 5-1 Describe the main structural features of the epidermis, and explain the functional significance of each. • 5-2 Explain what accounts for individual differences in skin color, and discuss the response of melanocytes to sunlight exposure. • 5-3 Describe the interaction between sunlight and vitamin D3 production. • 5-4 Describe the roles of epidermal growth factor. © 2012 Pearson Education, Inc. An Introduction to the Integumentary System • Learning Outcomes • 5-5 Describe the structure and functions of the dermis. • 5-6 Describe the structure and functions of the hypodermis. • 5-7 Describe the mechanisms that produce hair, and explain the structural basis for hair texture and color. © 2012 Pearson Education, Inc. An Introduction to the Integumentary System • Learning Outcomes • 5-8 Discuss the various kinds of glands in the skin, and list the secretions of those glands. • 5-9 Describe the anatomical structure of nails, and explain how they are formed. • 5-10 Explain how the skin responds to injury and repairs itself. • 5-11 Summarize the effects of aging on the skin. © 2012 Pearson Education, Inc. An Introduction to the Integumentary System • Two Components of the Cutaneous Membrane 1. Outer epidermis • Superficial epithelium (epithelial tissues) 1. Inner dermis • Connective tissues © 2012 Pearson Education, Inc. An Introduction to the Integumentary System • Accessory Structures • Originate in the dermis • Extend through the epidermis to skin surface • Hair • Nails • Multicellular exocrine glands © 2012 Pearson Education, Inc. An Introduction to the Integumentary System • Connections • Cardiovascular system • Blood vessels in the dermis • Nervous system • Sensory receptors for pain, touch, and temperature © 2012 Pearson Education, Inc. -
The Integumentary System the Integumentary System
Essentials of Anatomy & Physiology, 4th Edition Martini / Bartholomew The Integumentary System PowerPoint® Lecture Outlines prepared by Alan Magid, Duke University Slides 1 to 51 Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Integumentary Structure/Function Integumentary System Components • Cutaneous membrane • Epidermis • Dermis • Accessory structures • Subcutaneous layer (hypodermis) Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Integumentary Structure/Function Main Functions of the Integument • Protection • Temperature maintenance • Synthesis and storage of nutrients • Sensory reception • Excretion and secretion Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Integumentary Structure/Function Components of the Integumentary System Figure 5-1 Integumentary Structure/Function The Epidermis • Stratified squamous epithelium • Several distinct cell layers • Thick skin—five layers • On palms and soles • Thin skin—four layers • On rest of body Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Integumentary Structure/Function Cell Layers of The Epidermis • Stratum germinativum • Stratum spinosum • Stratum granulosum • Stratum lucidum (in thick skin) • Stratum corneum • Dying superficial layer • Keratin accumulation Copyright © 2007 Pearson Education, Inc., publishing as Benjamin Cummings Integumentary Structure/Function The Structure of the Epidermis Figure 5-2 Integumentary Structure/Function Cell Layers of The Epidermis • Stratum germinativum -

Anatomy of Skin Kyle EB
Anatomy of Skin Kyle EB 1.What is wrong with Kyle? 2.How does this condition affect Kyle’s health/life? 3.What is the new treatment? 4.What would you do if you were Kyle? (receive the treatment or not?) The Story of Kyle Hicks http://www.kansas. com/news/local/education/article21264273.html Skin ● The external surface of the body. ● Also referred to as the cutaneous membrane. ● About 16% of an adult’s total body weight. (So if you weigh 100 lbs that means your skin weighs 16 lbs) Structure of the Skin ● Two main parts: ○ Epidermis ■ superficial ■ thinner ■ epithelial tissue ○ Dermis ■ deeper ■ thicker ■ connective tissue *The two layers are attached by the basement membrane. ● Subcutaneous layer (subQ) ○ Also called the hypodermis. ○ Deep to the dermis, but not part of the skin. ○ consists of areolar and adipose ct ○ Attaches skin to underlying tissues and organs. Epidermis ● It is keratinized stratified squamous epithelium ● 4 key cells: 1. Keratinocytes ○ They make the protein keratin (a tough, protective protein). ○ The most numerous cell type: about 90% of the epidermal cells. 2. Melanocytes ○ About 8% of the epidermal cells. ○ Make the protein pigment melanin. ■ contributes to skin color ■ absorbs damaging ultraviolet light. 3. Langerhans cells ○ Immune cells located in the epidermis. 4. Merkel cells ○ associated with touch Layers of the Epidermis ● Most areas of the body have four strata or layers. This is referred to as thin skin. ● In areas of the body exposed to greater friction, like the fingertips, palms and soles of the feet the epidermis has five strata or layers. -

THE SKIN of the DOMESTIC PIG* WILLIAM MONTAGNA, Pn.D
THE SKIN OF THE DOMESTIC PIG* WILLIAM MONTAGNA, Pn.D. AND JEUNG S. YEN, M.S. Little is known about the anatomy or thehematoxylin and eosin, 0.05% toluidine blue physiology of porcine skin; the only pertinent(buffered at pH 4.5), the PAS technic, Verhoeff's stain, Giemsa stain, PTAH, HIll, Mallory's Azan modern studies are those of Schaffer (1) andtechnique and the DD reaction for —Sil and Kitamura (2), and Kurasumi and Kitamura (3)—S—S groups (l3arrnett and Seligman, 1952 (4)). on the glands of the so-called carpal organs. ThereAlkaline phosphatase, alpha naphthol esterase, is, furthermore, practically no data that sub-naphthol AS esterase (see Gomori (5)), tween esterase (Stowell and Lee, 1950 (6)) and eholines- stantiates the often repeated statement that theterases (Montagna and Ellis, 1957 (7)), were dem- skin of the pig is similar to that of man. Thisonstrated in frozen sections of tissues fixed in brief survey of the histology and histochemistry10% formalin. of the skin of the pig, therefore, should be a useful Succinic dehydrogenase (Farber and Louvierel, reference for those who plan to do further work1956 (5)), monoamino oxidase (Glenner, et at, 1957 (9)), and phosphorylase (Takeuchi and Kuri- on this animal. The pig, a highly specialized mam-aki, 1955 (10)) were studied in frozen sections of mal, with highly specialized habits, has manyunfixed tissues. local, topographic anatomical differentiations in its skin, which are beyond the scope of this study. GENERAL DESCRIPTION We have been more interested here in analyzing the general body skin, to allow us to draw some The skin of the pig has a remarkable number of focal specializations, some of these being asso- generalizations. -

Histology and Cytochemistry of Human Skin. Xiv. the Blood Supply of the Cutaneous Glands* Richard A
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector HISTOLOGY AND CYTOCHEMISTRY OF HUMAN SKIN. XIV. THE BLOOD SUPPLY OF THE CUTANEOUS GLANDS* RICHARD A. ELLIS, PH.D., WILLIAM MONTAGNA, Pn.D. AND HERBERT FANGER, M.D. Although the general blood supply to the skinout clearly against a nearly colorless background. has been mapped out in some detail (1), the exactIn thick frozen sections the entire capillary plexus vascular patterns of the human cutaneous ap-surrounding the cutaneous glands can frequently pendages need clarification. Other authors havebe seen as they emerge from their parent arteriole used injection methods, silver impregnation, and(Figs. 3, 6, 8). The endothelium of the arterioles benzidine to demonstrate the blood vessels of thehas practically no alkaline phosphatase activity, skin. None of these methods is completely satis-but enzyme activity becomes increasingly strong factory or practical in all cases. We have found,near the emergence of the capillaries and is in- however, that the capillaries supplying the skintense in the final capillary loops (9). Although it and the cutaneous appendages can be easilyis difficult to positively identify the arterioles and visualized in frozen sections with the azo-dyevenules in these preparations, recent observations technic for alkaline phosphatase (Fig. 1). Thisin our laboratory on the localization of phos- method is superior to the others used. It is simple,phorylase activity in human skin make the identi- quasi-specific, and demonstrates clearly even col-fication of arterioles easy, since the smooth mus- lapsed or blocked capillaries. Using this techniccle cells around them are rich in this enzyme (Fig. -

A Case of Canine Cutaneous Clear Cell Adnexal Carcinoma with Prominent Expression of Smooth Muscle Actin
J Toxicol Pathol 2010; 23: 265–269 Case Report A Case of Canine Cutaneous Clear Cell Adnexal Carcinoma with Prominent Expression of Smooth Muscle Actin Akiko Sakuma1, Shoko Nishiyama1, Kyohei Yasuno1, Tamio Ohmuro2, Junichi Kamiie3, and Kinji Shirota1,3 1 Research Institute of Biosciences and 3Laboratory of Veterinary Pathology, School of Veterinary Medicine, Azabu University, 1–17–71 Fuchinobe, Chuo-ku, Sagamihara, Kanagawa 252-5201, Japan 2Ohmuro Veterinary Clinic, 4262-2 Koyamacho, Machida, Tokyo 194-0212, Japan Abstract: Cutaneous clear cell adnexal carcinoma was found in the right lip of a 14-year-old male castrated Shih Tzu. Histologically, the tumor mostly consisted of neoplastic cells with clear or vacuolated cytoplasms and contained frequent tubular structures. Neoplastic cells showed coexpression of pan-cytokeratin (CK) and vimentin by double-labeled immunofluorescence staining. In addition, immunohistochemistry revealed that the tumor cells were positive for pan-CK (AE1/AE3, KL1, CAM 5.2), CK-7, CK-8, CK-14, CK-15, CK-18, vimentin and alpha-smooth muscle actin (SMA) with varied intensity and positivity. Among these marker proteins, SMA was positive in 75% of the tumor cells. On the other hand, CK-15, which is a specific marker of follicular stem cells, was expressed in less than 1% of the tumor cells. Based on these findings, the tumor showed diverse differentiation in apocrine sweat glands and the inner and outer root sheaths of hair follicles, indicating the follicular stem cell to be the origin of this tumor. (J Toxicol Pathol 2010; 23: 265–269) Key words: dermatopathology, dog, cytokeratin, skin, skin tumor, stem cell Introduction expression are useful for examining divergent adnexal differentiation of tumor3. -

Accessory Structures of the Skin and Their Functions
Copyright EMAP Publishing 2020 This article is not for distribution except for journal club use Clinical Practice Keywords Skin/Hair/Nails/Sweat glands/Sebaceous glands Systems of life This article has been Skin double-blind peer reviewed In this article... l The four main accessory structures of the skin l Structure and function of hair and nails l The role of sweat and sebaceous glands Skin 2: accessory structures of the skin and their functions Key points Author Sandra Lawton is Queen’s Nurse, nurse consultant and clinical lead Accessory structures dermatology, The Rotherham NHS Foundation Trust. of the skin include the hair, nails, Abstract Understanding the skin requires knowledge of its accessory structures. sweat and These originate embryologically from the epidermis and include hair, nails, sweat sebaceous glands glands and sebaceous glands. All are important in the skin’s key functions, including protection, thermoregulation and its sensory roles. This article, the second in a Hair’s primary two-part series, looks at the structure and function of the main accessory structures functions are of the skin. protection, warmth and sensory Citation Lawton S (2020) Skin 2: accessory structures of the skin and their functions. reception Nursing Times [online]; 116; 1, 44-46. Nails protect the tips of the fingers ccessory structures of the skin l Distribution of sweat-gland products; and toes include the hair, nails, sweat l Psychosocial – hair plays an glands and sebaceous glands. important role in determining self The two main types AThese structures embryologi- image and social perceptions of sweat gland – cally originate from the epidermis and are (Bit.ly/RUAccessoryStructures; eccrine and apocrine often termed “appendages”; they can extend Kolarsick et al, 2011; Graham-Brown and – are responsible down through the dermis into the hypo- Bourke, 2006) . -
Skin Integument Objectives to Gain a Greater Appreciation of the Diversity of Functions of Skin
Skin Integument Objectives To gain a greater appreciation of the diversity of functions of skin To recognize the different cell types and structures of the skin which make possible this functional diversity Functions of Skin: Functional Diversity of Skin • Protects against injury and desiccation • Maintenance of water balance • Excretes/secretes various substances • Thermoregulation • Receives stimuli − Temperature − Pain − Pressure • Basis of recognition and yields clues to one’s well being • Fat metabolism in the subcutaneous layer Fat Metabolism in the Subcutaneous Layer Fat Metabolism in the Subcutaneous Layer Obesity = Too much fat in the Subcutaneous Layer BINARY ORIGIN OF SKIN EPIDERMIS – ECTODERM DERMIS - MESODERM 31 Skin Overview and Introduction • http://www.youtube.com/watch?v=yKAzVC0WcmI Stratum Corneum Stratum Granulosum Stratum Spinosum Stratum Basale Layers of the Epidermis: palms and soles of feet Stratum Corneum – Keratinized flattened, denucleated, dead cells Stratum Granulosum – Keratohyalin granules Stratum Spinosum – Tonofibrils – desmosomes Stratum Basale – Continual renewal of epidermis Stratum Basale Stratum Spinosum Stratum Spinosum Stratum spinosum Slide 29: Thick Skin on finger cont. Keratohyalin granules The epidermis of Desmosomes thick skin is Hemidesmosomes subject to continuous1 friction and Epidermis pressure so the abundant desmosomes Stratum (and tonofibrils) spinosum withstand this and Dermis hold the cell layers together. Stratum basale Stratum Corneum Stratum Granulosum Stratum Corneum Stratum Corneum -
LAB-Skin-And-Adnexa-2018.Pdf
Skin Introduction It is easy enough to identify a basic tissue in isolation, but it takes further skill to incorporate the knowledge of these separate tissues and distinguish them as such in a compound tissue organ, such as the skin. These basic tissues will be found in some capacity in every tissue you encounter, and the function of this lab is to help you become more familiar in recognizing these specific tissues in organs. Skin is a great example of how the basic tissues combine to create a compound tissue and organ. It is a tissue composed of three distinct layers: epidermis, dermis and hypodermis. Each layer has specific functions, which are derived from their basic tissue components. Your job during this lab is to focus on identifying these basic tissues within these layers of skin and to think about the specific function they impart to the skin. Learning objectives and activities Using the Virtual Slidebox: A Examine the keratinized stratified squamous epithelium of the epidermis, and identify the modified epithelial exocrine glands. B Analyze the organization of collagen fibers and connective tissue cells in the dermis and hypodermis and interpret their function within the skin. C Locate muscle, peripheral nerve and modified nervous tissues in the skin. D Examine hair and hair follicles and determine that they are derived from the epidermis. E Investigate the anatomy of the growing fingernail and appreciate its relationship to skin. F Complete the self-quiz to test your understanding and master your learning. Epidermis: the epithelium of the skin The epidermis is a specialized epithelium: keratinized stratified squamous. -
The Integumentary System
5 The Integumentary System PowerPoint® Lecture Presentations prepared by Jason LaPres Lone Star College—North Harris © 2012 Pearson Education, Inc. An Introduction to the Integumentary System • The Integument • Is the largest system of the body • 16% of body weight • 1.5 to 2 m2 in area • The integument is made up of two parts 1. Cutaneous membrane (skin) 2. Accessory structures © 2012 Pearson Education, Inc. An Introduction to the Integumentary System • Two Components of the Cutaneous Membrane 1. Outer epidermis • Superficial epithelium (epithelial tissues) 2. Inner dermis • Connective tissues © 2012 Pearson Education, Inc. An Introduction to the Integumentary System • Accessory Structures • Originate in the dermis • Extend through the epidermis to skin surface • Hair • Nails • Multicellular exocrine glands © 2012 Pearson Education, Inc. An Introduction to the Integumentary System • Connections • Cardiovascular system • Blood vessels in the dermis • Nervous system • Sensory receptors for pain, touch, and temperature © 2012 Pearson Education, Inc. An Introduction to the Integumentary System • Hypodermis (Superficial Fascia or Subcutaneous Layer) • Loose connective tissue • Below the dermis • Location of hypodermic injections © 2012 Pearson Education, Inc. Figure 5-1 The Components of the Integumentary System Accessory Structures Cutaneous Membrane Hair shaft Epidermis Pore of sweat gland duct Papillary layer Dermis Tactile corpuscle Reticular layer Sebaceous gland Arrector pili muscle Sweat gland duct Hair follicle Lamellated corpuscle -
The Integumentary System Professor Edit
5 The Integumentary System_professor edit PowerPoint® Lecture Presentations prepared by Jason LaPres Lone Star College—North Harris © 2012 Pearson Education, Inc. An Introduction to the Integumentary System • Learning Outcomes • 5-1 Describe the main structural features of the epidermis, and explain the functional significance of each. • 5-2 Explain what accounts for individual differences in skin color, and discuss the response of melanocytes to sunlight exposure. • 5-3 Describe the interaction between sunlight and vitamin D3 production. • 5-4 Describe the roles of epidermal growth factor. © 2012 Pearson Education, Inc. An Introduction to the Integumentary System • Learning Outcomes • 5-5 Describe the structure and functions of the dermis. • 5-6 Describe the structure and functions of the hypodermis. • 5-7 Describe the mechanisms that produce hair, and explain the structural basis for hair texture and color. © 2012 Pearson Education, Inc. An Introduction to the Integumentary System • Learning Outcomes • 5-8 Discuss the various kinds of glands in the skin, and list the secretions of those glands. • 5-9 Describe the anatomical structure of nails, and explain how they are formed. • 5-10 Explain how the skin responds to injury and repairs itself. • 5-11 Summarize the effects of aging on the skin. © 2012 Pearson Education, Inc. An Introduction to the Integumentary System • The Integument • Is the largest system of the body • 16% of body weight • 1.5 to 2 m2 in area • The integument is made up of two parts 1. Cutaneous membrane (skin) 2. Accessory structures © 2012 Pearson Education, Inc. An Introduction to the Integumentary System • Two Components of the Cutaneous Membrane 1. -
Integumentary System
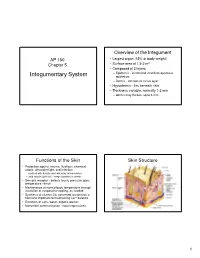
Overview of the Integument AP 150 • Largest organ (15% of body weight) Chapter 5 • Surface area of 1.5-2 m 2 • Composed of 2 layers – Epidermis - keratinized stratified squamous Integumentary System epithelium – Dermis - connective tissue layer • Hypodermis - lies beneath skin • Thickness variable, normally 1-2 mm – dermis may thicken, up to 6 mm Functions of the Skin Skin Structure • Protection against trauma, fluid loss, chemical attack, ultraviolet light, and infection – packed with keratin and linked by desmosomes – acid mantle (pH 4-6) - keeps bacteria in check • Sensory receptor - detects touch, pressure, pain, temperature stimuli • Maintenance of normal body temperature through insulation or evaporative cooling, as needed • Synthesis of vitamin D3; converted to calcitriol, a hormone important to maintaining Ca ++ balance • Excretion of salts, water, organic wastes • Nonverbal communication - facial expressions Figure 5.1 1 The Epidermis • A keratinized stratified squamous epithelium Layers of the Epidermis • Avascular; nourished by diffusion of nutrients from dermis • Cells found in the epidermis include • Stratum basale (stratum geminativum) – Stem cells • undifferentiated cells in deepest layers • Stratum spinosum – Keratinocytes – majority of the epidermal cells • Stratum granulosum – Melanocytes • Stratum lucidum (only in thick skin) • Synthesize pigment melanin that shields against UV – Tactile (Merkel) cells • Stratum corneum • receptor cells; detect light touch – Dendritic (Langerhans) cells • macrophages guard against pathogens