Betaine Monograph
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Beneficial Effects of Betaine: a Comprehensive Review
biology Review Beneficial Effects of Betaine: A Comprehensive Review Madan Kumar Arumugam 1,2 , Matthew C. Paal 1,2, Terrence M. Donohue Jr. 1,2,3, Murali Ganesan 1,2, Natalia A. Osna 1,2 and Kusum K. Kharbanda 1,2,3,* 1 Research Service, Veterans Affairs Nebraska-Western Iowa Health Care System, Omaha, NE 68105, USA; [email protected] (MK.A.); [email protected] (M.C.P.); [email protected] (T.M.D.J.); [email protected] (M.G.); [email protected] (N.A.O.) 2 Department of Internal Medicine, University of Nebraska Medical Center, Omaha, NE 68198, USA 3 Department of Biochemistry & Molecular Biology, University of Nebraska Medical Center, Omaha, NE 68198, USA * Correspondence: [email protected]; Tel.: +1-402-995-3752; Fax: +1-402-995-4600 Simple Summary: A large number of studies report that medicinal herbs and many food ingredients protect against the development of liver disease because they possess antioxidant, anti-inflammatory, or anti-necrotic activities. This review focuses on the biological and beneficial effects of dietary betaine (trimethylglycine), a naturally occurring and crucial methyl donor, that restores methionine homeostasis in cells. We describe recent studies on betaine’s mechanism(s) of action as a therapeutic agent for improving indices of alcohol-induced and metabolic- associated liver disease. Due to its low cost, high tolerability, and efficacy, we suggest betaine as a promising therapeutic for clinical use to treat these aforementioned diseases as well as other liver-/non-liver-related diseases and conditions. Abstract: Medicinal herbs and many food ingredients possess favorable biological properties that contribute to their therapeutic activities. -

Structure-Guided Function Discovery of an NRPS-Like Glycine Betaine Reductase for Choline Biosynthesis in Fungi
Structure-guided function discovery of an NRPS-like glycine betaine reductase for choline biosynthesis in fungi Yang Hai (海洋)a, Arthur M. Huangb, and Yi Tanga,b,1 aDepartment of Chemical and Biomolecular Engineering, University of California, Los Angeles, CA 90095; and bDepartment of Chemistry and Biochemistry, University of California, Los Angeles, CA 90095 Edited by Wilfred A. van der Donk, Howard Hughes Medical Institute and University of Illinois, Urbana–Champaign, Urbana, IL, and accepted by Editorial Board Member Stephen J. Benkovic April 10, 2019 (received for review February 27, 2019) Nonribosomal peptide synthetases (NRPSs) and NRPS-like enzymes focused on a fungal CAR-like protein with an unknown function. It have diverse functions in primary and secondary metabolisms. By is distinguished from all other CARs due to an extra C-terminal using a structure-guided approach, we uncovered the function of a YdfG-like short-chain dehydrogenase/reductase domain. We NRPS-like enzyme with unusual domain architecture, catalyzing named this protein ATRR and the corresponding gene atrr after its two sequential two-electron reductions of glycine betaine to choline. unusual domain architecture (A-T-R1-R2). The presence of two Structural analysis based on the homology model suggests cation-π fused R domains in ATRR implies that it could catalyze two con- interactions as the major substrate specificity determinant, which was secutive two-electron reductions of a carboxylic acid to yield an verified using substrate analogs and inhibitors. Bioinformatic analysis alcohol (Fig. 1B). Moreover, a genomic survey reveals that atrr indicates this NRPS-like glycine betaine reductase is highly conserved genes are widespread but exclusive to eukaryotes, mostly in fungi and widespread in kingdom fungi. -

Betaine Analogues and Related Compounds For
BETAINE ANALOGUES AND RELATED COMPOUNDS FOR BIOMEDICAL APPLICATIONS A thesis presented in fulfilment of the requirement for the degree of Doctor of Philosophy in Chemical and Process Engineering at the University of Canterbury Madhusudan Vasudevamurthy 2006 Department of Chemical and Process Engineering University of Canterbury Christchurch, New Zealand Acknowledgements I owe a debt of gratitude to my supervisor, Dr. Michael Lever for being the force behind this project. He has been my guiding star and a great mentor. His probing questions, enthusiasm to do things right and constantly finding new ways of functioning to resolve a problem was contagious. His humor and never ending discussions were a source of encouragement making him a great friend and confidant. The contribution of my supervisor Dr. Ken Morison is most appreciated. His continual support and guidance during the last couple of years has added immense value to my thesis. His invaluable suggestions, an eagerness to learn and implement has brought about the shape of this thesis. I am deeply indebted to Prof. Peter George and Prof. Steve Chambers for their valuable inputs and suggestions in this thesis. Their willingness to support and accommodate me in their hectic schedule is most appreciated. I am glad of this opportunity to extend my gratitude to Prof. Laurence Weatherley, my previous supervisor, whose encouragement and words of wisdom motivated me to pursue my PhD. His continual support helped me in the founding years of my thesis, opening doors to a wealth of knowledge and a thirst for learning more. His motivation has made me a scientist from an amateur. -

Betaine Supplementation for Various Clinical Disorders
Online - 2455-3891 Vol 10, Issue 10, 2017 Print - 0974-2441 Review Article BETAINE SUPPLEMENTATION FOR VARIOUS CLINICAL DISORDERS JAYALAKSHMI M, VANITHA V* Department of Biochemistry, School of Life Sciences, Vels University, Chennai - 600 117, Tamil Nadu, India. Email: [email protected] Received: 21 February 2017, Revised and Accepted: 24 March 2017 ABSTRACT Betaine is distributed widely in animals, plants, and microorganisms and rich dietary sources include seafood, especially marine invertebrates. Betaine is N-trimethylated amino acid called as glycine betaine. It is a by-product. Betaine aldehyde is produced when choline dehydrogenase acts on choline, then betaine aldehyde is oxidized to form betaine by aldehyde dehydrogenase. Metabolic derived betaines possess various functions in our body in which they act as methyl donor which helps in liver function, detoxication, and cellular functions. It plays an important role in fat metabolism. Recent research found that betaine can convert homocysteine to cysteine thus they prevent heart disease. Choline is oxidized to betaine in liver and kidney. Intracellular betaine serves as an osmolyte that regulates cell volume and tissue integrity. Betaine not only plays as an osmolyte but also play a major role in the protection of the liver and other tissues. Consequently, it has been proposed that betaine has significant nutrient for prevention of chronic disease. Betaine has been shown to protect internal organs, improve vascular risk factors, and enhance performance. Databases of betaine content in food are being developed for correlation with population health studies. This review focuses on the aspects of wide research field with emphasis on a recent data relevant to various human diseases. -

Effect of Choline Or Betaine Supplementation on Broilers Exposed to Different Temperature Treatments
University of Tennessee, Knoxville TRACE: Tennessee Research and Creative Exchange Masters Theses Graduate School 8-2013 Effect of choline or betaine supplementation on broilers exposed to different temperature treatments Joseph D. Summers University of Tennessee - Knoxville, [email protected] Follow this and additional works at: https://trace.tennessee.edu/utk_gradthes Part of the Poultry or Avian Science Commons Recommended Citation Summers, Joseph D., "Effect of choline or betaine supplementation on broilers exposed to different temperature treatments. " Master's Thesis, University of Tennessee, 2013. https://trace.tennessee.edu/utk_gradthes/2465 This Thesis is brought to you for free and open access by the Graduate School at TRACE: Tennessee Research and Creative Exchange. It has been accepted for inclusion in Masters Theses by an authorized administrator of TRACE: Tennessee Research and Creative Exchange. For more information, please contact [email protected]. To the Graduate Council: I am submitting herewith a thesis written by Joseph D. Summers entitled "Effect of choline or betaine supplementation on broilers exposed to different temperature treatments." I have examined the final electronic copy of this thesis for form and content and recommend that it be accepted in partial fulfillment of the equirr ements for the degree of Master of Science, with a major in Animal Science. Michael O. Smith, Major Professor We have read this thesis and recommend its acceptance: Brynn Voy, John Waller Accepted for the Council: Carolyn R. Hodges Vice Provost and Dean of the Graduate School (Original signatures are on file with official studentecor r ds.) Effect of choline or betaine supplementation on broilers exposed to different temperature treatments A Thesis Presented for the Master of Science Degree The University of Tennessee, Knoxville Joseph D. -
Mesoionic Compounds 3/25/17
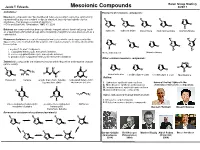
Baran Group Meeting Jacob T. Edwards Mesoionic Compounds 3/25/17 Definitions: Examples of mesoionic compounds: Mesoionic compounds are “five membered heterocycles which cannot be satisfactorily represented by any one covalent or dipolar structure, but only has hybrids of polar R R R R O+ structures…they possess a sextet of electrons.” N+ N+ N+ N+ O- – Ollis and Stanforth, Tetrahedron, 1985, 41, 2239 N - N - - N O O O NH- O O O NH Betaines are compounds that bear a positively charged cationic functional group (such R sydnone sydnone imine as a quaternary ammonium group) and a negatively charged functional group (such as a münchnone münchnone imine isomünchnone carboxylate). R1 R1 S- Mesomeric betaines are neutral conjugated molecules which can be represented by S+ R + N+ N+ dipolar structures in which both the positive and negative charges are delocalized within N+ S the π-system O- N - N O- N O- O O N N R S i. acyclic (1,3- and 1,5-dipoles) R2 R2 ii. conjugated heterocyclic mesomeric betaines thioisomünchnone thiomünchnone iii. cross-conjugated heterocyclic mesomeric betaines iv. pseudo-cross-conjugated heterocyclic mesomeric betaines Other common mesoionic compounds: Zwitterionic compounds are neutral molecules with both positive and negative charges O PR3 (amino acids). O+ S+ O+ 2 3 1 3 O R + R R R R - - - N Me O O O N+ + - + 4 R O S S 1 N CO2 N R N R R2 N - Me Me + oxamünchnone 1,3-dithiolium-4-olate 1,3-dithiolium-4-olate Montréalone O O 5 N R R O- Outline: mesoionic betaine acyclic mesomeric betaine conjugated heterocyclic (azomethine ylide) mesomeric betaine I. -

Evaluation of Betaine and Methionine Replacement for Improving
University of Arkansas, Fayetteville ScholarWorks@UARK Theses and Dissertations 12-2014 Evaluation of Betaine and Methionine Replacement for Improving Performance and Meat Quality for Broilers reared under Higher Temperature Conditions Malea Graham Frank University of Arkansas, Fayetteville Follow this and additional works at: http://scholarworks.uark.edu/etd Part of the Molecular, Genetic, and Biochemical Nutrition Commons, and the Poultry or Avian Science Commons Recommended Citation Frank, Malea Graham, "Evaluation of Betaine and Methionine Replacement for Improving Performance and Meat Quality for Broilers reared under Higher Temperature Conditions" (2014). Theses and Dissertations. 2064. http://scholarworks.uark.edu/etd/2064 This Dissertation is brought to you for free and open access by ScholarWorks@UARK. It has been accepted for inclusion in Theses and Dissertations by an authorized administrator of ScholarWorks@UARK. For more information, please contact [email protected], [email protected]. Evaluation of Betaine and Methionine Replacement for Improving Performance and Meat Quality for Broilers reared under Higher Temperature Conditions Evaluation of Betaine and Methionine Replacement for Improving Performance and Meat Quality for Broilers reared under Higher Temperature Conditions A dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in Poultry Science Malea Frank University of Arkansas Bachelor of Science in Agriculture, Food & Life Sciences, 2001 December 2014 University of Arkansas This dissertation is approved for recommendation to the Graduate Council. Dr. Susan E. Watkins Dissertation Director Dr. Randolph J. Chick Dr. Nicholas B. Anthony Committee Member Committee Member Dr. Charles V. Maxwell Committee Member ABSTRACT 4,096 broiler chicks were randomly allocated to 128 floor pens (32 birds/pen). -

Arkivoc Template P
Reviews and Accounts ARKIVOC 2013 (i) 424-469 Recent advances in neutral and anionic N-heterocyclic carbene – betaine interconversions. Synthesis, characterization, and applications Andreas Schmidt,* Sascha Wiechmann, and Tyll Freese Clausthal University of Technology, Institute of Organic Chemistry, Leibnizstrasse 6, D-38678 Clausthal-Zellerfeld, Germany E-mail: [email protected] DOI: http://dx.doi.org/10.3998/ark.5550190.p008.251 Abstract Some mesoionic compounds, i.e. five-membered representatives of the class of conjugated mesomeric betaines (CMB), are in equilibrium with their tautomeric normal N-heterocyclic carbenes (nNHC). In addition, anionic N-heterocyclic carbenes, generated by deprotonation of mesoionic compounds, have been described. The first examples of conversions of cross- conjugated mesomeric betaines (CCMB), 6-oxopyrimidinium-4-olates, into normal N- heterocyclic carbenes have been reported as well. CCMB such as imidazolium-4-carboxylate and pyrazolium-4-carboxylate can decarboxylate to form abnormal (aNHC) or remote N-heterocyclic carbenes (rNHC). Most conversions of betaines into N-heterocyclic carbenes start from pseudo- cross-conjugated mesomeric betaines (PCCMB) which can be regarded as heterocumulene adducts of nNHC. Thus, decarboxylations of imidazolium-2-carboxylates, 1,2,4-triazole-3- carboxylates, pyrazolium-3-carboxylates or indazolium-3-carboxylates yield N-heterocyclic carbenes which have been used in catalysis, complex chemistry, heterocyclic synthesis, and organocatalysis. Keywords: Mesoionic compounds, mesoionic carbenes, ylides, borane adducts, zwitterions, sydnones, heterocumulene adducts, decarboxylation, mesomeric betaine Table of Contents 1. Introduction 2. Interconversion Reactions 2.1. Interconversions of normal (nNHC) and anionic N-heterocyclic carbenes and conjugated mesomeric betaines (CMB) including mesoionic compounds 2.2. Interconversions of normal N-heterocyclic carbenes (nNHC) and ylides Page 424 ©ARKAT-USA, Inc. -

Betaine Chemistry, Roles, and Potential Use in Liver Disease
BBAGEN-15-673 R2 Betaine chemistry, roles, and potential use in liver disease Christopher R Day and Stephen A Kempson Laboratory of Receptor Biology and Gene Expression, Center for Cancer Research, National Cancer Institute, NIH, Bethesda, MD 20892, USA and Department of Cellular & Integrative Physiology, Indiana University School of Medicine, Indianapolis, IN 46202-5120, USA Running header: Betaine and liver disease Correspondence to: Dr SA Kempson, MS 306, 635 Barnhill Dr, Indianapolis, IN 46202-5120, USA Tel: 317-274-7772. Email: [email protected] Abbreviations ALD, alcoholic liver disease. AMPK, AMP-activated protein kinase. BGT1, Na+/Cl-- dependent betaine-GABA transporter. BHMT, betaine-homocysteine methyltransferase. DMG, dimethylglycine. NAFLD, non-alcoholic fatty liver disease. NASH, non- alcoholic steatohepatitis. OCTN2, organic cation/carnitine transporter. SAH, S- adenosylhomocysteine. SAM, S-adenosylmethionine. SIT1, Na+-dependent imino acid transporter. SNAT, Na+-dependent neutral amino acid transporter. _________________________________________________________________________________ 1 This is the author's manuscript of the article published in final edited form as: Day, C. R., & Kempson, S. A. (2016). Betaine chemistry, roles, and potential use in liver disease. Biochimica et Biophysica Acta (BBA) - General Subjects, 1860(6), 1098–1106. http://doi.org/10.1016/j.bbagen.2016.02.001 BBAGEN-15-673 R2 Abstract Background. Betaine is the trimethyl derivative of glycine and is normally present in human plasma due to dietary intake and endogenous synthesis in liver and kidney. Betaine is utilized in the kidney primarily as an osmoprotectant whereas in the liver its primary role is in metabolism as a methyl group donor. In both organs a specific betaine transporter mediates cellular uptake of betaine from plasma. -

Betaine Concentration of Common Foods in the US
Betaine Concentration of Common Foods in the US. Juhi R. Williams1, Juliette Howe1 , Steven H. Zeisel 2 , Mei-Heng Mar2, Joanne M. Holden 1; 1 Nutrient Data Lab., USDA – ARS- Beltsville Human Nutrition Research Center, 10300 Baltimore Ave, Bldg 005, Rm 201, Beltsville, MD 20705-2325., 2 Department of Nutrition, University of North Carolina at Chapel Hill, Chapel Hill, NC 27599 Abstract. Betaine, a choline derivative, is produced in the human body from choline and contributes methyl groups for the conversion of homocysteine to methionine. Elevated levels of plasma homocysteine can be harmful to blood vessels leading to the development of heart disease, stroke, and peripheral vascular disease. Betaine also assists the liver to process lipids and protect against chemical damages. Our objective is to develop the first comprehensive database determining the amount of betaine concentration in a nationally representative sampling of common foods consumed in the United States. Various food items were obtained from 12 – 24 retail outlets using the sampling plan developed for the USDA’s National Food and Nutrient Analysis Program (Pehrsson, P. et al. J. Food Comp. Anal 13:379, 2000). Products (530) were analyzed for betaine concentration as purchased or after cooking using liquid chromatography with electrospray ionization – isotope dilution mass spectrometry. Quality assurance methods included the use of duplicate sampling, in-house control methods and standard reference materials. The results showed that of the foods analyzed, wheat bran and wheat germ have the highest concentration of betaine (>1gm/100g). Baked products (33 – 226 mg/100g), spinach, beets, crustaceans and finfish are also good sources of betaine. -

A Potassium Chloride to Glycine Betaine Osmoprotectant Switch in the Extreme Halophile Halorhodospira Halophila Ratnakar Deole1,2 & Wouter D
www.nature.com/scientificreports OPEN A potassium chloride to glycine betaine osmoprotectant switch in the extreme halophile Halorhodospira halophila Ratnakar Deole1,2 & Wouter D. Hof1* Halophiles utilize two distinct osmoprotection strategies. The accumulation of organic compatible solutes such as glycine betaine does not perturb the functioning of cytoplasmic components, but represents a large investment of energy and carbon. KCl is an energetically attractive alternative osmoprotectant, but requires genome-wide modifcations to establish a highly acidic proteome. Most extreme halophiles are optimized for the use of one of these two strategies. Here we examine the extremely halophilic Proteobacterium Halorhodospira halophila and report that medium K+ concentration dramatically alters its osmoprotectant use. When grown in hypersaline media containing substantial K+ concentrations, H. halophila accumulates molar concentrations of KCl. However, at limiting K+ concentrations the organism switches to glycine betaine as its major osmoprotectant. In contrast, the closely related organism Halorhodospira halochloris is limited to using compatible solutes. H. halophila performs both de novo synthesis and uptake of glycine betaine, matching the biosynthesis and transport systems encoded in its genome. The medium K+ concentration (~10 mM) at which the KCl to glycine betaine osmoprotectant switch in H. halophila occurs is near the K+ content of the lake from which it was isolated, supporting an ecological relevance of this osmoprotectant strategy. All halophilic organisms face the risk of cellular dehydration caused by the high osmotic activity of saline envi- ronments, and require osmoprotection strategies to survive. Since saline oceans, saline lakes, inland seas, and saline groundwater constitute ~97% of all water on earth1, and salt deposits underlay roughly one quarter of the land on earth2, saline and hypersaline environments are of great ecological signifcance. -

Structures and Synthesis of Zwitterionic Polymers
Polymers 2014, 6, 1544-1601; doi:10.3390/polym6051544 OPEN ACCESS polymers ISSN 2073–4360 www.mdpi.com/journal/polymers Review Structures and Synthesis of Zwitterionic Polymers André Laschewsky 1,2 1 Fraunhofer Institute of Applied Polymer Research IAP, Geiselbergstr.69, 14476 Potsdam-Golm, Germany; E-Mail: [email protected]; Fax: +49-331-568-3000 2 Department of Chemistry, Universität Potsdam, Karl-Liebknechtstr.24–25, 14476 Potsdam-Golm, Germany; E-Mail: [email protected]; Tel.: +49-331-977-5225; Fax: +49-331-977-5036 Received: 16 April 2014; in revised form: 3 May 2014 / Accepted: 8 May 2014 / Published: 23 May 2014 Abstract: The structures and synthesis of polyzwitterions (“polybetaines”) are reviewed, emphasizing the literature of the past decade. Particular attention is given to the general challenges faced, and to successful strategies to obtain polymers with a true balance of permanent cationic and anionic groups, thus resulting in an overall zero charge. Also, the progress due to applying new methodologies from general polymer synthesis, such as controlled polymerization methods or the use of “click” chemical reactions is presented. Furthermore, the emerging topic of responsive (“smart”) polyzwitterions is addressed. The considerations and critical discussions are illustrated by typical examples. Keywords: review; polyzwitterion; polyampholyte; zwitterionic group; betaine; synthesis; monomer; polymerization; post-polymerization modification 1. Introduction This review is focused on the structure and synthesis of zwitterionic polymers. Polyzwitterions or synonymous polybetaines bear, within their constitutional repeat unit, the same number of anionic and cationic groups [1]. Essentially, the ionic groups are functional over a large pH-window. Accordingly, the overall charge of polyzwitterions is zero under normal conditions, notwithstanding that they are characterized by a high density of polymer-bound ion pairs attached to the polymer chain.