A Spatial Hierarchical Analysis of the Temporal Influences of the El Niño-Southern Oscillation and Weather on Dengue in Kalutara District, Sri Lanka
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Sri Lanka 2015 International Religious Freedom Report
SRI LANKA 2015 INTERNATIONAL RELIGIOUS FREEDOM REPORT Executive Summary The constitution states every person is “entitled to freedom of thought, conscience, and religion, including the freedom to have or to adopt a religion or belief of his choice.” It gives citizens the right to manifest their religion or belief in worship, observance, practice, or teaching both in public and in private. The constitution and other laws give Buddhism “foremost place” and commit the government to protecting it. Civil society organizations such as the Centre for Policy Alternatives (CPA), Center for Human Rights and Research, and others said the new government, which took office in January, pursued an agenda including a renewed commitment to the rule of law and willingness to investigate and prosecute state officials implicated in or responsible for inciting past religiously based violence. There were instances, however, in which local police and local government officials appeared to act in concert with Buddhist nationalist organizations, although not to the extent as previously. For example, police continued to cite outdated government circulars restricting the construction of religious facilities in attempts to force churches to cease operations. In multiple instances, police reportedly failed to respond or were reluctant to arrest or pursue criminal cases against individuals instigating attacks on minority religious sites. CPA noted in its “Advocacy Brief – Human Rights Violations and Surveillance in Sri Lanka,” which covered the period from January to September (hereafter CPA Brief), the government had not yet prosecuted hardline Buddhist monks involved in attacks in 2014 against Muslims and Christians. Parliament’s passage of the Assistance to and Protection of Victims of Crime and Witnesses Act in February strengthened safeguards for persons involved in legal actions against criminal perpetrators implicated in attacks upon religious sites. -
Priority Wsproject.Pdf
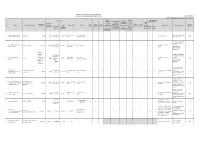
NATIONAL WATER SUPPLY & DRAINAGE BOARD PRIORITY WATER SUPPLY PROJECTS IN PIPE LINE As at 21.07.2016 Note: Not tabulated according to the priority rank. Technical Cabinet Loan Agreement Project Cost Official Review Project Review Sub Signed(Yes/No) Committee Commier Committee committee Committee No. of New on Economic cial Population to PAC Board NPD GM, approval (Mr. on Cabinet SCAPC Year of No Project Electorates Covered Connections Source of Funds Contractor Management Contract Current Status Works to be done be Served GOSL approval Approval Approval Addl.GM(WSP) Padmanadan, Mr. Economic approval approval Implement expected Contract Sum (Mr. singned Foreign Local Component , Jayasinghe, Mr. approval (million) paskaralinga or not Bank Bank (million) DGM(Sewerag Lal Premanath) (chired by m) e) approval PM) Anamaduwa Integrated Euro 26.8 + Deutsche Bank , •M/s SETA, Spain- Subsidiary Loan Agreement 1 Anamaduwa 81,741 18,160 Rs. 1,941.90 y y y y y y y y y y y y Contractor mobilized 2016 Water Supply (Phase I) Rs. 1,863.85 HNB ELLIPS JV,France under preparation. • Treasury Guarantee for the HNB loan is pending Kelani Right Bank Water Euro 108.86 + Credit Agricole CIB, Foreign & Local Loans are from TOD. 2 Gampaha, Colombo 1,744,000 387,500 Rs. 5,281.72 Degremont Sa y y y y y y y y y y y y 2016 Supply - Stage II Rs. 10,000 HNB, France signed. • Subsidiary Loan Agreement under preparation. 400,000 (includes EURO 123.73 • Treasury Guarantee for service the HNB loan is pending + EURO 23.42 Greater Matale Water enhancement BNP PARIBAS OTV-SADE Foreign & Local Loans are from TOD. -
CHAPTER 4 Perspective of the Colombo Metropolitan Area 4.1 Identification of the Colombo Metropolitan Area
Urban Transport System Development Project for Colombo Metropolitan Region and Suburbs CoMTrans UrbanTransport Master Plan Final Report CHAPTER 4 Perspective of the Colombo Metropolitan Area 4.1 Identification of the Colombo Metropolitan Area 4.1.1 Definition The Western Province is the most developed province in Sri Lanka and is where the administrative functions and economic activities are concentrated. At the same time, forestry and agricultural lands still remain, mainly in the eastern and south-eastern parts of the province. And also, there are some local urban centres which are less dependent on Colombo. These areas have less relation with the centre of Colombo. The Colombo Metropolitan Area is defined in order to analyse and assess future transport demands and formulate a master plan. For this purpose, Colombo Metropolitan Area is defined by: A) areas that are already urbanised and those to be urbanised by 2035, and B) areas that are dependent on Colombo. In an urbanised area, urban activities, which are mainly commercial and business activities, are active and it is assumed that demand for transport is high. People living in areas dependent on Colombo area assumed to travel to Colombo by some transport measures. 4.1.2 Factors to Consider for Future Urban Structures In order to identify the CMA, the following factors are considered. These factors will also define the urban structure, which is described in Section 4.3. An effective transport network will be proposed based on the urban structure as well as the traffic demand. At the same time, the new transport network proposed will affect the urban structure and lead to urban development. -

CHAP 9 Sri Lanka
79o 00' 79o 30' 80o 00' 80o 30' 81o 00' 81o 30' 82o 00' Kankesanturai Point Pedro A I Karaitivu I. Jana D Peninsula N Kayts Jana SRI LANKA I Palk Strait National capital Ja na Elephant Pass Punkudutivu I. Lag Provincial capital oon Devipattinam Delft I. Town, village Palk Bay Kilinochchi Provincial boundary - Puthukkudiyiruppu Nanthi Kadal Main road Rameswaram Iranaitivu Is. Mullaittivu Secondary road Pamban I. Ferry Vellankulam Dhanushkodi Talaimannar Manjulam Nayaru Lagoon Railroad A da m' Airport s Bridge NORTHERN Nedunkeni 9o 00' Kokkilai Lagoon Mannar I. Mannar Puliyankulam Pulmoddai Madhu Road Bay of Bengal Gulf of Mannar Silavatturai Vavuniya Nilaveli Pankulam Kebitigollewa Trincomalee Horuwupotana r Bay Medawachchiya diya A d o o o 8 30' ru 8 30' v K i A Karaitivu I. ru Hamillewa n a Mutur Y Pomparippu Anuradhapura Kantalai n o NORTH CENTRAL Kalpitiya o g Maragahewa a Kathiraveli L Kal m a Oy a a l a t t Puttalam Kekirawa Habarane u 8o 00' P Galgamuwa 8o 00' NORTH Polonnaruwa Dambula Valachchenai Anamaduwa a y O Mundal Maho a Chenkaladi Lake r u WESTERN d Batticaloa Naula a M uru ed D Ganewatta a EASTERN g n Madura Oya a G Reservoir Chilaw i l Maha Oya o Kurunegala e o 7 30' w 7 30' Matale a Paddiruppu h Kuliyapitiya a CENTRAL M Kehelula Kalmunai Pannala Kandy Mahiyangana Uhana Randenigale ya Amparai a O a Mah Reservoir y Negombo Kegalla O Gal Tirrukkovil Negombo Victoria Falls Reservoir Bibile Senanayake Lagoon Gampaha Samudra Ja-Ela o a Nuwara Badulla o 7 00' ng 7 00' Kelan a Avissawella Eliya Colombo i G Sri Jayewardenepura -

Results of Parliamentary General Election - 1947
RESULTS OF PARLIAMENTARY GENERAL ELECTION - 1947 No. and Name of Electoral District Name of the Elected Candidate Symbol allotted No of No of Total No. of Votes No of Votes Votes Polled including Registered Polled rejected rejected Electors 1 Colombo North George R. de Silva Umbrella 7,501 189 14,928 30,791 Lionel Cooray Elephant 6,130 E.C.H. Fernando Cup 501 A.P. de Zoysa House 429 H.C. Abeywardena Hand 178 2 Colombo Central A.E. Goonasinha Bicycle 23,470 3,489 102,772 55,994 T.B. Jayah Cart Wheel 18,439 Pieter Keuneman Umbrella 15,435 M.H.M. Munas House 8,600 Mrs. Ayisha Rauff Tree 8,486 V.J. Perera Elephant 5,950 V.A. Sugathadasa Lamp 4,898 G.W. Harry de Silva Pair of Scales 4,141 V.A. Kandiah Clock 3,391 S. Sarawanamuttu Chair 2,951 P. Givendrasingha Hand 1,569 K. Dahanayake Cup 997 K. Weeraiah Key 352 K.C.F. Deen Star 345 N.R. Perera Butterfly 259 3 Colombo South R. A. de Mel Key 6,452 149 18,218 31,864 P. Sarawanamuttu Flower 5,812 Bernard Zoysa Chair 3,774 M.G. Mendis Hand 1,936 V.J. Soysa Cup 95 Page 1 of 15 RESULTS OF PARLIAMENTARY GENERAL ELECTION - 1947 No. and Name of Electoral District Name of the Elected Candidate Symbol allotted No of No of Total No. of Votes No of Votes Votes Polled including Registered Polled rejected rejected Electors 4 Wellawatta-Galkissa Colvin R. de Silva Key 11,606 127 21,750 38,664 Gilbert Perera Cart Wheel 4,170 L.V. -

Index No Marks Sex Med Name 2200015 041 F 2200023 040 F 2200031 047 F 2200040 049 M 2200058 046 F 2200066 028 M 2200074 042 F 22
INDEX NO MARKS SEX MED NAME ADDRESS POSTAL ADDRESS 2200015 041 F SIN WASANTHI, M.K. DIVISIONAL SECRETARIAT, THIHAGODA. 2200023 040 F SIN KUMUDINI, E.V.S. DIVISIONAL SECRETARIAT, THIHAGODA. 2200031 047 F SIN WICKRAMASINGHE, W.M.K.P. DIVISIONAL SECRETARY OFFICE, UKUWELA. 2200040 049 M SIN BANDULA, B.G. DIVISIONAL SECRETARIAT, UKUWELA. 2200058 046 F SIN SAMARATHUNGE, S.M.N.R.K. DIVISIONAL SECRETARIAT, UKUWELA. 2200066 028 M SIN ABULASIN, S. DIVISIONAL SECRETARIAT, UKUWELA. 2200074 042 F SIN RANASINGHE, M.G.C. DIVISIONAL SECRETARIAT, UKUWELA. 2200082 040 F SIN MALIMAGE, G.M.P.S. A.G.A. OFFICE, KOLONNAWA. 2200090 044 M SIN PREMALAL, A.A.D.K. DIVISIONAL SECRETARIAT, KOLONNAWA. 2200104 042 F SIN GURUGE, I. DIVISIONAL SECRETARIAT, KOLONNAWA. 2200112 037 F SIN VIOLET, V.D.R. DIVISIONAL SECRETARIAT, KOLONNAWA. 2200120 051 F SIN BANNEHEKA, B.M.W.K. DIVISIONAL SECRETARIAT, ANAMADUWA. 2200139 044 F SIN HERATH, I.M.N.S.K. DISTRICT SECRETARIAT, SAMURDHI OFFICE, KURUNEGALA. 2200147 053 M SIN WIJESOORIYA, K.D.G. DISTRICT SECRETARIAT, KURUNEGALA. 2200155 046 M SIN CHAMINDA, K.M.R. SAMURDHI MANAGER, DIVISIONAL SECRETARIAT, PASSARA. 2200163 055 F SIN HETTIGE, D.H.S.L. DIVISIONAL SECRETARIAT, PASSARA. 2200171 066 F SIN KARUNAWATHI, J.M. DIVISIONAL SECRETARIAT, PASSARA. 2200180 053 F SIN DUNUSINGHE, P.N. DIVISIONAL SECRETARIAT, PASBAGE KORALE, NAWALAPITIYA. 2200198 060 F SIN SAMUDDIKA, W.P.N. DIVISIONAL SECERATARIAT, PASBAGE KORALE, NAWALAPITIYA. 2200201 042 M SIN RANAWEERA, K.S. DIVISIONAL SECRETARIAT, PASBAGE KORALE, NAWALAPITIYA. 2200228 041 F SIN INDRASEELI, K.M.N. DIVISIONAL SECRETARIAT, IMBULPE. 2200236 045 F SIN UDAGALADENIYA, S.M.I. -

Flood Situation Report
Flood Situation Report Colombo | Sri Lanka Flood Situation Update No.2 – Sri Lanka 18 May 2010 at 1830 hrs GLIDE: FL-2010-000092-LKA Situation Since Friday, 14 May 2010, heavy monsoon rains have resulted in flash floods, high-winds, landslides, lightning and thunder storms in 11 districts in Sri Lanka. Nine of the districts are in the southeast and include: Colombo, Gampaha, Kalutara, Ratnapura, Kegalle, Matara, Kegalle, Puttalam and Galle. Two of the affected districts are in the northeast: Trincomalee and Anuradhapura. See attached table breakdown and map. As of Tuesday, 18 May 2010, over 298,543 persons (62,261 families) have been affected by the heavy rains. This includes minor displacement of 7,477 people and 8 deaths. The Government of Sri Lanka is responding to the crisis through local and central levels and the Navy has been deployed with their boat teams to assist with evacuations. The Department of Irrigation has indicated that rising water levels exist for the following areas (see details in Annex 1): • Kelani River, Hanwella DS Division, Colombo District • Kalu Ganga (river), Palindanuwara DS Division, Kalutara District • Gin Ganga (river) The National Building Research Organisation has issued a Landslide warning (level 2 – be ready for evacuation) to the following districts and AGA Divisions under threat: • Ratnapura District – Palmadulla, Kuruvita, Eheliyagoda, Kalawana, Kolonna, Elapatha Divisions • Kalutara District – Kalutara, Bulathsinhala, Horana, Palinda Nuwara, Agalawatte, Walallawita, Bandaragama, Mathugama, Ingiriya, Panadura Divisions • Galle District – Neluwa, Hiniduma, Thawalama, Baddegama, Elpitiya, Bope Poddala, Nagoda, Karandeniya, Weliwitiya Divithura Divisions • Kegalle District – Deraniyagala, Yatiyantota, Dehiowita Divisions Warning of cut slope failures possible in Colombo and Gampaha Districts. -
Sri Lanka) Using Terrasar-X Satellite Data (28May2017)
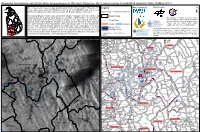
Mapping Inundation extent for Kalu Ganga basin in Western Province (Sri Lanka) using TerraSAR-X Satellite Data (28May2017) Due to heavy rains in past few days, landslides and floods in Sri Lanka killed 151 people, 111 Legend Map Prepared by Data Provider people still missing, displacing 100,000 and directly affecting 500,000 people across many districts according to the initial estimates by state-run Disaster Management Center. Satellite Image : TerraSAR-X 28 May 2017 ± International Disaster Charter was activated by Disaster Management Centre (DMC) and Division Map coordinated by International Water Management Institute (IWMI)/CGIAR. The first satellite The analysis excluded permanent water image obtained on 28-05-2017 by German Aerospace Centre (DLR) showed vast areas of ! Cities/Town bodies including reservoir, tanks and ponds standing flood waters along the Southern and South-Western Provinces. Initial estimates and this reflects only the inundation extent. from satellite images indicate that Matara (49.3) and Kalutara with 31.6 km2 flooded area, Please note the surface water extent Road Streams mapped has not yet been validated in the are the worst affected districts followed by Galle (20.2 km2), Rathnapura (14.9 km2), Flood extent Colombo (5.6 km2) and Gampaha (4.5 km2). Detailed Divisional Secretariat wise flood The depiction and use of boundaries, geographic names and affected area for these six districts are given in the attached excel file. Kalutara is reeling (28 May 2017) related data shown in these maps are based on the sources under worst flood since 2003. Residents in affected pockets are reluctant to move away from they have been drawn from and quoted. -
Name List of Sworn Translators in Sri Lanka
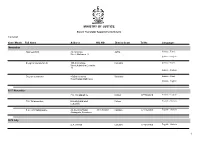
MINISTRY OF JUSTICE Sworn Translator Appointments Details 1/29/2021 Year / Month Full Name Address NIC NO District Court Tel No Languages November Rasheed.H.M. 76,1st Cross Jaffna Sinhala - Tamil Street,Ninthavur 12 Sinhala - English Sivagnanasundaram.S. 109,4/2,Collage Colombo Sinhala - Tamil Street,Kotahena,Colombo 13 Sinhala - English Dreyton senaratna 45,Old kalmunai Baticaloa Sinhala - Tamil Road,Kalladi,Batticaloa Sinhala - English 1977 November P.M. Thilakarathne Chilaw 0777892610 Sinhala - English P.M. Thilakarathne kirimathiyana East, Chilaw English - Sinhala Lunuwilla. S.D. Cyril Sadanayake 26, De silva Road, 331490350V Kalutara 0771926906 English - Sinhala Atabagoda, Panadura 1979 July D.A. vincent Colombo 0776738956 English - Sinhala 1 1/29/2021 Year / Month Full Name Address NIC NO District Court Tel No Languages 1992 July H.M.D.A. Herath 28, Kolawatta, veyangda 391842205V Gampaha 0332233032 Sinhala - English 2000 June W.A. Somaratna 12, sanasa Square, Gampaha 0332224351 English - Sinhala Gampaha 2004 July kalaichelvi Niranjan 465/1/2, Havelock Road, Colombo English - Tamil Colombo 06 2008 May saroja indrani weeratunga 1E9 ,Jayawardanagama, colombo English - battaramulla Sinhala - 2008 September Saroja Indrani Weeratunga 1/E/9, Jayawadanagama, Colombo Sinhala - English Battaramulla 2011 July P. Maheswaran 41/B, Ammankovil Road, Kalmunai English - Sinhala Kalmunai -2 Tamil - K.O. Nanda Karunanayake 65/2, Church Road, Gampaha 0718433122 Sinhala - English Gampaha 2011 November J.D. Gunarathna "Shantha", Kalutara 0771887585 Sinhala - English Kandawatta,Mulatiyana, Agalawatta. 2 1/29/2021 Year / Month Full Name Address NIC NO District Court Tel No Languages 2012 January B.P. Eranga Nadeshani Maheshika 35, Sri madhananda 855162954V Panadura 0773188790 English - French Mawatha, Panadura 0773188790 Sinhala - 2013 Khan.C.M.S. -

Spatial Variability of Rainfall Trends in Sri Lanka from 1989 to 2019 As an Indication of Climate Change
International Journal of Geo-Information Article Spatial Variability of Rainfall Trends in Sri Lanka from 1989 to 2019 as an Indication of Climate Change Niranga Alahacoon 1,2,* and Mahesh Edirisinghe 1 1 Department of Physics, University of Colombo, Colombo 00300, Sri Lanka; [email protected] 2 International Water Management Institute (IWMI), 127, Sunil Mawatha, Pelawatte, Colombo 10120, Sri Lanka * Correspondence: [email protected] Abstract: Analysis of long-term rainfall trends provides a wealth of information on effective crop planning and water resource management, and a better understanding of climate variability over time. This study reveals the spatial variability of rainfall trends in Sri Lanka from 1989 to 2019 as an indication of climate change. The exclusivity of the study is the use of rainfall data that provide spatial variability instead of the traditional location-based approach. Henceforth, daily rainfall data available at Climate Hazards Group InfraRed Precipitation corrected with stations (CHIRPS) data were used for this study. The geographic information system (GIS) is used to perform spatial data analysis on both vector and raster data. Sen’s slope estimator and the Mann–Kendall (M–K) test are used to investigate the trends in annual and seasonal rainfall throughout all districts and climatic zones of Sri Lanka. The most important thing reflected in this study is that there has been a significant increase in annual rainfall from 1989 to 2019 in all climatic zones (wet, dry, intermediate, and Semi-arid) of Sri Lanka. The maximum increase is recorded in the wet zone and the minimum increase is in the semi-arid zone. -

Kalutara District Secretariat for the Year 2016
ANNUAL PERPORMANCE REPORT & ACCOUNTS - 2016 KALUTARA DISTRICT T Table Of Contents Page 1.Message of the Government Agent / District Secretary ............................................................................ 4 2.Introduction on Kalutara District Secretariat ............................................................................................. 5 2.1 Vision and Mission Statement ............................................................................................................ 5 2.2 Objectives and Values of the District Secretariat .............................................................................. 6 2.3 Duties and Progress of the District Secretariat ................................................................................... 7 3. Introduction on the District ...................................................................................................................... 8 3.1 District Boundaries .............................................................................................................................. 9 3.2 Historical Background of Kalutara District. ......................................................................................... 9 3.3 Land Use of Kalutara District ............................................................................................................... 9 3.4 Agricultural Pattern of the People in the District ............................................................................ 10 3.5 Monthly Rainfall Pattern of the District ........................................................................................... -

A Case Study of Kalutara District, Sri Lanka K
KDU Journal of Multidisciplinary Studies (KJMS) Volume 1. Issue1, 2017 KJMS 2017 VOL.1 (1): 34-47 RECENT CHANGES IN POPULATION AND ITS IMPACT ON USAGE OF DRINKING WATER SOURCES IN HOUSEHOLDS: A CASE STUDY OF KALUTARA DISTRICT, SRI LANKA K. K. E. Perera [email protected] Computer Teaching Unit, Faculty of Arts, University of Colombo, Colombo 03, Sri Lanka ABSTRACT The major problem that arises with the rapid growth of population is whether it is possible to fulfil basic requirements of human beings such as food, water, shelter and air (De Silva, 2007). Especially, drinking water is a basic need of human life and in fact an essential component in primary healthcare and poverty alleviation (Amponsah, Aidam and Senadza, 2009). However, the growing intensity of population and development activities create tremendous pressure on available water resources. Therefore, it is essential to understand the relationships among a full range of population characteristics such as the size, growth, distribution, and density of population, total households and the usage of water sources. With this brief background, the aim of this paper is to identify the recent changes in population and its impact on the usage of drinking water sources in households in Kalutara district during the period of 2001-2012. Towards achieving this aim, population and households data on sources of drinking water was obtained from the reports of Census of Population and Housing in 2001 and 2012. The data were analyzed using thematic maps and correlation analyses. Accordingly, the highest population and population density were recorded in the west coast while the lowest were in rural areas and there was an increase both spatially and temporally.