Multigene Panels in Prostate Cancer Risk Assessment
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Molecular Profile of Tumor-Specific CD8+ T Cell Hypofunction in a Transplantable Murine Cancer Model
Downloaded from http://www.jimmunol.org/ by guest on September 25, 2021 T + is online at: average * The Journal of Immunology , 34 of which you can access for free at: 2016; 197:1477-1488; Prepublished online 1 July from submission to initial decision 4 weeks from acceptance to publication 2016; doi: 10.4049/jimmunol.1600589 http://www.jimmunol.org/content/197/4/1477 Molecular Profile of Tumor-Specific CD8 Cell Hypofunction in a Transplantable Murine Cancer Model Katherine A. Waugh, Sonia M. Leach, Brandon L. Moore, Tullia C. Bruno, Jonathan D. Buhrman and Jill E. Slansky J Immunol cites 95 articles Submit online. Every submission reviewed by practicing scientists ? is published twice each month by Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts http://jimmunol.org/subscription Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html http://www.jimmunol.org/content/suppl/2016/07/01/jimmunol.160058 9.DCSupplemental This article http://www.jimmunol.org/content/197/4/1477.full#ref-list-1 Information about subscribing to The JI No Triage! Fast Publication! Rapid Reviews! 30 days* Why • • • Material References Permissions Email Alerts Subscription Supplementary The Journal of Immunology The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2016 by The American Association of Immunologists, Inc. All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. This information is current as of September 25, 2021. The Journal of Immunology Molecular Profile of Tumor-Specific CD8+ T Cell Hypofunction in a Transplantable Murine Cancer Model Katherine A. -
5R)-5-Hydroxytriptolide (LLDT-8
www.nature.com/scientificreports OPEN (5R)-5-Hydroxytriptolide (LLDT- 8) induces substantial epigenetic mediated immune response Received: 24 October 2018 Accepted: 16 July 2019 network changes in fbroblast-like Published: xx xx xxxx synoviocytes from rheumatoid arthritis patients Shicheng Guo1, Jia Liu2,3, Ting Jiang2,3, Dungyang Lee4, Rongsheng Wang2,3, Xinpeng Zhou2, Yehua Jin2, Yi Shen2,3, Yan Wang3, Fengmin Bai2,3, Qin Ding2,3, Grace Wang5, Jianyong Zhang6, Xiaodong Zhou7, Steven J. Schrodi1,8 & Dongyi He2,3 Tripterygium is a traditional Chinese medicine that has widely been used in the treatment of rheumatic disease. (5R)-5-hydroxytriptolide (LLDT-8) is an extracted compound from Tripterygium, which has been shown to have lower cytotoxicity and relatively higher immunosuppressive activity when compared to Tripterygium. However, our understanding of LLDT-8-induced epigenomic impact and overall regulatory changes in key cell types remains limited. Doing so will provide critically important mechanistic information about how LLDT-8 wields its immunosuppressive activity. The purpose of this study was to assess the efects of LLDT-8 on transcriptome including mRNAs and long non-coding RNA (lncRNAs) in rheumatoid arthritis (RA) fbroblast-like synoviocytes (FLS) by a custom genome-wide microarray assay. Signifcant diferential expressed genes were validated by QPCR. Our work shows that 394 genes (281 down- and 113 up-regulated) were signifcantly diferentially expressed in FLS responding to the treatment of LLDT-8. KEGG pathway analysis showed 20 pathways were signifcantly enriched and the most signifcantly enriched pathways were relevant to Immune reaction, including cytokine- cytokine receptor interaction (P = 4.61 × 10−13), chemokine signaling pathway (P = 1.01 × 10−5) and TNF signaling pathway (P = 2.79 × 10−4). -

Human Induced Pluripotent Stem Cell–Derived Podocytes Mature Into Vascularized Glomeruli Upon Experimental Transplantation
BASIC RESEARCH www.jasn.org Human Induced Pluripotent Stem Cell–Derived Podocytes Mature into Vascularized Glomeruli upon Experimental Transplantation † Sazia Sharmin,* Atsuhiro Taguchi,* Yusuke Kaku,* Yasuhiro Yoshimura,* Tomoko Ohmori,* ‡ † ‡ Tetsushi Sakuma, Masashi Mukoyama, Takashi Yamamoto, Hidetake Kurihara,§ and | Ryuichi Nishinakamura* *Department of Kidney Development, Institute of Molecular Embryology and Genetics, and †Department of Nephrology, Faculty of Life Sciences, Kumamoto University, Kumamoto, Japan; ‡Department of Mathematical and Life Sciences, Graduate School of Science, Hiroshima University, Hiroshima, Japan; §Division of Anatomy, Juntendo University School of Medicine, Tokyo, Japan; and |Japan Science and Technology Agency, CREST, Kumamoto, Japan ABSTRACT Glomerular podocytes express proteins, such as nephrin, that constitute the slit diaphragm, thereby contributing to the filtration process in the kidney. Glomerular development has been analyzed mainly in mice, whereas analysis of human kidney development has been minimal because of limited access to embryonic kidneys. We previously reported the induction of three-dimensional primordial glomeruli from human induced pluripotent stem (iPS) cells. Here, using transcription activator–like effector nuclease-mediated homologous recombination, we generated human iPS cell lines that express green fluorescent protein (GFP) in the NPHS1 locus, which encodes nephrin, and we show that GFP expression facilitated accurate visualization of nephrin-positive podocyte formation in -

Pharmacological Targeting of the Mitochondrial Phosphatase PTPMT1 by Dahlia Doughty Shenton Department of Biochemistry Duke
Pharmacological Targeting of the Mitochondrial Phosphatase PTPMT1 by Dahlia Doughty Shenton Department of Biochemistry Duke University Date: May 1 st 2009 Approved: ___________________________ Dr. Patrick J. Casey, Supervisor ___________________________ Dr. Perry J. Blackshear ___________________________ Dr. Anthony R. Means ___________________________ Dr. Christopher B. Newgard ___________________________ Dr. John D. York Dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the Department of Biochemistry in the Graduate School of Duke University 2009 ABSTRACT Pharmacological Targeting of the Mitochondrial Phosphatase PTPMT1 by Dahlia Doughty Shenton Department of Biochemistry Duke University Date: May 1 st 2009 Approved: ___________________________ Dr. Patrick J. Casey, Supervisor ___________________________ Dr. Perry J. Blackshear ___________________________ Dr. Anthony R. Means ___________________________ Dr. Christopher B. Newgard ___________________________ Dr. John D. York An abstract of a dissertation submitted in partial fulfillment of the requirements for the degree of Doctor of Philosophy in the Department of Biochemistry in the Graduate School of Duke University 2009 Copyright by Dahlia Doughty Shenton 2009 Abstract The dual specificity protein tyrosine phosphatases comprise the largest and most diverse group of protein tyrosine phosphatases and play integral roles in the regulation of cell signaling events. The dual specificity protein tyrosine phosphatases impact multiple -
![RT² Profiler PCR Array (96-Well Format and 384-Well [4 X 96] Format)](https://docslib.b-cdn.net/cover/9005/rt%C2%B2-profiler-pcr-array-96-well-format-and-384-well-4-x-96-format-1459005.webp)
RT² Profiler PCR Array (96-Well Format and 384-Well [4 X 96] Format)
RT² Profiler PCR Array (96-Well Format and 384-Well [4 x 96] Format) Human Protein Phosphatases Cat. no. 330231 PAHS-045ZA For pathway expression analysis Format For use with the following real-time cyclers RT² Profiler PCR Array, Applied Biosystems® models 5700, 7000, 7300, 7500, Format A 7700, 7900HT, ViiA™ 7 (96-well block); Bio-Rad® models iCycler®, iQ™5, MyiQ™, MyiQ2; Bio-Rad/MJ Research Chromo4™; Eppendorf® Mastercycler® ep realplex models 2, 2s, 4, 4s; Stratagene® models Mx3005P®, Mx3000P®; Takara TP-800 RT² Profiler PCR Array, Applied Biosystems models 7500 (Fast block), 7900HT (Fast Format C block), StepOnePlus™, ViiA 7 (Fast block) RT² Profiler PCR Array, Bio-Rad CFX96™; Bio-Rad/MJ Research models DNA Format D Engine Opticon®, DNA Engine Opticon 2; Stratagene Mx4000® RT² Profiler PCR Array, Applied Biosystems models 7900HT (384-well block), ViiA 7 Format E (384-well block); Bio-Rad CFX384™ RT² Profiler PCR Array, Roche® LightCycler® 480 (96-well block) Format F RT² Profiler PCR Array, Roche LightCycler 480 (384-well block) Format G RT² Profiler PCR Array, Fluidigm® BioMark™ Format H Sample & Assay Technologies Description The Human Protein Phosphatases RT² Profiler PCR Array profiles the gene expression of the 84 most important and well-studied phosphatases in the mammalian genome. By reversing the phosphorylation of key regulatory proteins mediated by protein kinases, phosphatases serve as a very important complement to kinases and attenuate activated signal transduction pathways. The gene classes on this array include both receptor and non-receptor tyrosine phosphatases, catalytic subunits of the three major protein phosphatase gene families, the dual specificity phosphatases, as well as cell cycle regulatory and other protein phosphatases. -

Live-Cell Imaging Rnai Screen Identifies PP2A–B55α and Importin-Β1 As Key Mitotic Exit Regulators in Human Cells
LETTERS Live-cell imaging RNAi screen identifies PP2A–B55α and importin-β1 as key mitotic exit regulators in human cells Michael H. A. Schmitz1,2,3, Michael Held1,2, Veerle Janssens4, James R. A. Hutchins5, Otto Hudecz6, Elitsa Ivanova4, Jozef Goris4, Laura Trinkle-Mulcahy7, Angus I. Lamond8, Ina Poser9, Anthony A. Hyman9, Karl Mechtler5,6, Jan-Michael Peters5 and Daniel W. Gerlich1,2,10 When vertebrate cells exit mitosis various cellular structures can contribute to Cdk1 substrate dephosphorylation during vertebrate are re-organized to build functional interphase cells1. This mitotic exit, whereas Ca2+-triggered mitotic exit in cytostatic-factor- depends on Cdk1 (cyclin dependent kinase 1) inactivation arrested egg extracts depends on calcineurin12,13. Early genetic studies in and subsequent dephosphorylation of its substrates2–4. Drosophila melanogaster 14,15 and Aspergillus nidulans16 reported defects Members of the protein phosphatase 1 and 2A (PP1 and in late mitosis of PP1 and PP2A mutants. However, the assays used in PP2A) families can dephosphorylate Cdk1 substrates in these studies were not specific for mitotic exit because they scored pro- biochemical extracts during mitotic exit5,6, but how this relates metaphase arrest or anaphase chromosome bridges, which can result to postmitotic reassembly of interphase structures in intact from defects in early mitosis. cells is not known. Here, we use a live-cell imaging assay and Intracellular targeting of Ser/Thr phosphatase complexes to specific RNAi knockdown to screen a genome-wide library of protein substrates is mediated by a diverse range of regulatory and targeting phosphatases for mitotic exit functions in human cells. We subunits that associate with a small group of catalytic subunits3,4,17. -
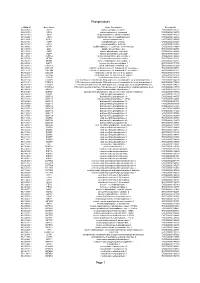
Phosphatases Page 1
Phosphatases esiRNA ID Gene Name Gene Description Ensembl ID HU-05948-1 ACP1 acid phosphatase 1, soluble ENSG00000143727 HU-01870-1 ACP2 acid phosphatase 2, lysosomal ENSG00000134575 HU-05292-1 ACP5 acid phosphatase 5, tartrate resistant ENSG00000102575 HU-02655-1 ACP6 acid phosphatase 6, lysophosphatidic ENSG00000162836 HU-13465-1 ACPL2 acid phosphatase-like 2 ENSG00000155893 HU-06716-1 ACPP acid phosphatase, prostate ENSG00000014257 HU-15218-1 ACPT acid phosphatase, testicular ENSG00000142513 HU-09496-1 ACYP1 acylphosphatase 1, erythrocyte (common) type ENSG00000119640 HU-04746-1 ALPL alkaline phosphatase, liver ENSG00000162551 HU-14729-1 ALPP alkaline phosphatase, placental ENSG00000163283 HU-14729-1 ALPP alkaline phosphatase, placental ENSG00000163283 HU-14729-1 ALPPL2 alkaline phosphatase, placental-like 2 ENSG00000163286 HU-07767-1 BPGM 2,3-bisphosphoglycerate mutase ENSG00000172331 HU-06476-1 BPNT1 3'(2'), 5'-bisphosphate nucleotidase 1 ENSG00000162813 HU-09086-1 CANT1 calcium activated nucleotidase 1 ENSG00000171302 HU-03115-1 CCDC155 coiled-coil domain containing 155 ENSG00000161609 HU-09022-1 CDC14A CDC14 cell division cycle 14 homolog A (S. cerevisiae) ENSG00000079335 HU-11533-1 CDC14B CDC14 cell division cycle 14 homolog B (S. cerevisiae) ENSG00000081377 HU-06323-1 CDC25A cell division cycle 25 homolog A (S. pombe) ENSG00000164045 HU-07288-1 CDC25B cell division cycle 25 homolog B (S. pombe) ENSG00000101224 HU-06033-1 CDKN3 cyclin-dependent kinase inhibitor 3 ENSG00000100526 HU-02274-1 CTDSP1 CTD (carboxy-terminal domain, -

Table SI. List of Differentially Expressed Genes Detected from Three Expression Profiling Datasets GSE18842, GSE30219 and GSE33532
Table SI. List of differentially expressed genes detected from three expression profiling datasets GSE18842, GSE30219 and GSE33532. DEGs Gene Upregulated (n=428) ABCB6, ACP1, ADAM12, ADAMDEC1, ADAMTS12, AFAP1-AS1, AKR1B10, ALDH3B2, ALYREF, ANKRD22, APOBEC3B, ARG2, ARNTL2, ARTN, ASF1B, ATAD2, ATP11B, AUNIP, AURKB, BAIAP2L1, BCL11A, BIK, BIRC5, BLM, BNIP3, BORA, BUB1, BYSL, C10orf2, C12orf56, C12orf66, C15orf48, C2CD4A, C4orf46, C5orf46, CABYR, CALU, CASC7, CBX2, CCNA2, CCNE1, CCNE2, CCT2, CCT6A, CDC25A, CDC25C, CDC45, CDCA2, CDCA3, CDCA8, CDH3, CDK1, CDK5R1, CDKN2A, CDT1, CEMIP, CENPF, CENPH, CENPI, CENPK, CENPL, CENPM, CENPN, MLF1IP, CENPW, CERS6, CHAC2, CHEK1, CIART, CKAP2, CKAP2L, CKAP4, CKS1B, CNFN, COCH, COL11A1, COL3A1, COL5A1, COL5A2, CPD, CRABP2, CST1, CTSV, CTTN, CXCL13, DARS2, DBF4, DCAF13, DCUN1D1, DCUN1D5, DENND1A, DEPDC1, DEPDC1B, DEPDC7, DHFR, DIO2, DONSON, DPY19L1, DSC2, DSCC1, DSG2, DST, DTL, DUS4L, E2F7, ECT2, EGLN3, EIF4EBP1, ELOVL6, ENAH, ENO1, EPT1, ERCC6L, ERO1A, ESPL1, ESRP1, ETV4, EZH2, F12, FAM169A, FAM210A, FAM64A, FAM69A, FAM83A, FAM83D, FAM83F, FAM83H, FANCD2, FANCI, FAP, FAXC, FBXO32, FBXO45, FBXO5, FERMT1, FGF11, FHL2, FLAD1, FNDC1, FOXM1, GAL, GALNT14, GALNT2, GALNT7, GART, GCLC, GCLM, GGH, GINS3, GJB2, GJB6, GMPS, GOLM1, GPX2, GRHL1, GRTP1, GTSE1, H2AFX, HELLS, HILPDA, HIST1H2AE, HIST1H2BC, HIST1H2BH, HIST1H2BJ, HIST1H3F, HIST3H2A, HLTF, HMGA1, HMGA2, HMGB3, HOOK1, HORMAD1, HOXA10, HOXC10, HOXD10, HRASLS, HS6ST2, HSPA4L, HYLS1, IDH2, IGF2BP3, IGFBP2, IGFBP3, IGHM, IGSF9, IL4I1, IQGAP3, IRF6, ITGA11, KCNK1, -

The Human Phosphatase Interactome
FEBS Letters 586 (2012) 2732–2739 journal homepage: www.FEBSLetters.org Review The human phosphatase interactome: An intricate family portrait ⇑ Francesca Sacco a,1, Livia Perfetto a,1, Luisa Castagnoli a, Gianni Cesareni a,b, a Department of Biology, University of Rome ‘‘Tor Vergata’’, Rome, Italy b Research Institute ‘‘Fondazione Santa Lucia’’, Rome, Italy article info abstract Article history: The concerted activities of kinases and phosphatases modulate the phosphorylation levels of Received 23 March 2012 proteins, lipids and carbohydrates in eukaryotic cells. Despite considerable effort, we are still miss- Revised 8 May 2012 ing a holistic picture representing, at a proteome level, the functional relationships between Accepted 8 May 2012 kinases, phosphatases and their substrates. Here we focus on phosphatases and we review and inte- Available online 21 May 2012 grate the available information that helps to place the members of the protein phosphatase super- Edited by Marius Sudol, Giulio Superti-Furga families into the human protein interaction network. In addition we show how protein interaction and Wilhelm Just domains and motifs, either covalently linked to the phosphatase domain or in regulatory/adaptor subunits, play a prominent role in substrate selection. Keywords: Ó 2012 Federation of European Biochemical Societies. Published by Elsevier B.V. All rights reserved. Human phosphatome Phosphatase family classification Substrate recognition specificity 1. Introduction protein kinases. 428 are known or predicted to phosphorylate ser- ine and threonine residues, while the remaining 90 are members of Phosphorylation is a widespread post-translational modifica- the tyrosine kinase family [3,12]. By contrast, in the human gen- tion governing signal propagation [1]. -

The Ancestor of Extant Japanese Fancy Mice Contributed to the Mosaic Genomes of Classical Inbred Strains
Downloaded from genome.cshlp.org on September 27, 2021 - Published by Cold Spring Harbor Laboratory Press Resource The ancestor of extant Japanese fancy mice contributed to the mosaic genomes of classical inbred strains Toyoyuki Takada,1,2 Toshinobu Ebata,3,4 Hideki Noguchi,4 Thomas M. Keane,5 David J. Adams,5 Takanori Narita,3 Tadasu Shin-I,3,4 Hironori Fujisawa,2,6 Atsushi Toyoda,4 Kuniya Abe,7 Yuichi Obata,7 Yoshiyuki Sakaki,8,9 Kazuo Moriwaki,7 Asao Fujiyama,4 Yuji Kohara,3 and Toshihiko Shiroishi1,2,10 1Mammalian Genetics Laboratory, National Institute of Genetics, Mishima, Shizuoka 411-8540, Japan; 2Transdisciplinary Research Integration Center, Research Organization of Information and Systems, Minato-ku, Tokyo 105-0001, Japan; 3Genome Biology Laboratory, National Institute of Genetics, Mishima, Shizuoka 411-8540, Japan; 4Comparative Genomics Laboratory, National Institute of Genetics, Mishima, Shizuoka 411-8540, Japan; 5The Wellcome Trust Sanger Institute, Hinxton, Cambridgeshire, CB10 1SA, United Kingdom; 6The Institute of Statistical Mathematics, 10-3 Midori-cho, Tachikawa, Tokyo 190-8562, Japan; 7RIKEN BioResource Center, Tsukuba, Ibaraki 305-0074, Japan; 8Genome Science Center, RIKEN Yokohama Institute, Yokohama, Kanagawa 230-0045, Japan Commonly used classical inbred mouse strains have mosaic genomes with sequences from different subspecific origins. Their genomes are derived predominantly from the Western European subspecies Mus musculus domesticus, with the remaining sequences derived mostly from the Japanese subspecies Mus musculus molossinus. However, it remains unknown how this intersubspecific genome introgression occurred during the establishment of classical inbred strains. In this study, we resequenced the genomes of two M. m. molossinus–derived inbred strains, MSM/Ms and JF1/Ms. -

Molecular Network of Collagen, Type III, Alpha-1 at the Gene Expression Level: Obstacles That Translational Research Must Overcome
Int. J. Mol. Sci. 2015, 16, 15031-15056; doi:10.3390/ijms160715031 OPEN ACCESS International Journal of Molecular Sciences ISSN 1422-0067 www.mdpi.com/journal/ijms Article Differences between Mice and Humans in Regulation and the Molecular Network of Collagen, Type III, Alpha-1 at the Gene Expression Level: Obstacles that Translational Research Must Overcome Lishi Wang 1,2, Hongchao Liu 3, Yan Jiao 1,4, Erjian Wang 3, Stephen H. Clark 5, Arnold E. Postlethwaite 6,7, Weikuan Gu 1,7,* and Hong Chen 3,* 1 Department of Orthopedic Surgery and BME-Campbell Clinic, University of Tennessee Health Science Center, Memphis, TN 38163, USA; E-Mails: [email protected] (L.W.); [email protected] (Y.J.) 2 Department of Basic Research, Inner Mongolia Medical College, Inner Mongolia 010110, China 3 Integrative Research Center, the first Hospital of Qiqihaer City, Qiqihaer 161005, China; E-Mails: [email protected] (H.L.); [email protected] (E.W.) 4 Department of Medicine, Mudanjiang Medical College, Mudanjiang 157001, China 5 Department of Genetics and Developmental Biology, University of Connecticut Health Center, Farmington, CT 06030, USA; E-Mail: [email protected] 6 Department of Medicine, University of Tennessee Health Science Center, Memphis, TN 38163, USA; E-Mail: [email protected] 7 Research Service, Veterans Affairs Medical Center, Memphis, TN 38104, USA * Authors to whom correspondence should be addressed; E-Mails: [email protected] (W.G.); [email protected] (H.C.); Tel.: +01-901-448-2258 (W.G.); +86-452-242-5981 (H.C.); Fax: +01-901-448-6062 (W.G.); +86-452-247-0942 (H.C.). -

A Genome-Wide Screen Reveals Functional Gene Clusters in the Cancer Genome and Identifies Epha2 As a Mitogen in Glioblastoma
Published OnlineFirst November 6, 2006; DOI: 10.1158/0008-5472.CAN-06-1408 Research Article A Genome-Wide Screen Reveals Functional Gene Clusters in the Cancer Genome and Identifies EphA2 as a Mitogen in Glioblastoma Fenghua Liu,1 Peter J. Park,3,7 Weil Lai,3 Elizabeth Maher,2,4,5 Arnab Chakravarti,1 Laura Durso,4,5 Xiuli Jiang,1 Yi Yu,1 Amanda Brosius,1 Meredith Thomas,1 Lynda Chin,4,6 Cameron Brennan,4,6 Ronald A. DePinho,4,5 Isaac Kohane,3,7 Rona S. Carroll,1 Peter M. Black,1,2 and Mark D. Johnson1,2 1Department of Neurological Surgery, Brigham and Women’s Hospital and Harvard Medical School; 2Program in Neuro-Oncology, Brigham and Women’s Hospital and Dana-Farber/Harvard Cancer Center; 3Harvard-Partners Center for Genetics and Genomics; 4Center for Applied Cancer Science, Belfer Foundation Institute for Innovative Cancer Science, Department of Medical Oncology, Dana-Farber Cancer Institute; Departments of 5Medicine and Genetics and 6Dermatology, Harvard Medical School; and 7Children’s Hospital Informatics Program, Boston, Massachusetts Abstract human cancers (2–4). However, hundreds of genes with altered A novel genome-wide screen that combines patient outcome expression may be identified in such analyses, and it is often analysis with array comparative genomic hybridization and difficult to determine from these analyses alone which of the mRNA expression profiling was developed to identify genes changes in mRNA expression are upstream, initiating determinants with copy number alterations, aberrant mRNA expression, and of tumor phenotype and which ones represent secondary changes relevance to survival in glioblastoma.