Licorice Root
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mint in the Garden Kristie Buckland and Dan Drost Vegetable Specialist
Revised May 2020 Mint in the Garden Kristie Buckland and Dan Drost Vegetable Specialist Summary Plants: Mint can be grown from seed or Mint is a rapid growing perennial herb with transplants. Since mints readily hybridize between many varieties that grow up to 3 feet tall and are quite different types, plants grown from seed often fail to be invasive. Mint grows best in full sun to partial shade, true to type. For specific cultivars or varieties, buy should be planted early in the growing season and is established plants from reputable sources, take cuttings generally hardy to -20° F. Mint prefers moist soil from known plants, or divide an established plant. conditions, but excess water will promote root and leaf Divide and replant established plants in the spring diseases. Harvest leaves and stems throughout the before growth starts or early in the fall. season, or cut back within an inch of the ground about Planting and Spacing: Sow seeds ¼ inch deep three times a season, just before the plant blooms. and then thin seedlings once they emerge. Transplants should be planted with roots just beneath the soil Varieties surface. Row spacing should be at least 2 feet apart to allow for growth. Use care when selecting mint varieties. The taste Water: Water regularly during the growing and smell varies greatly between varieties. For cold areas season, supplying up to 1 to 2 inches per week, of Utah, peppermint, spearmint, and woolly mints are depending on temperatures, exposure and soil very hardy. All varieties are well suited to areas of Utah conditions. -

Sage Salvia Officinalis Garden Sage, Red Sage, Salvia Salvatrix Photo
Sage Salvia officinalis Garden Sage, Red Sage, Salvia salvatrix Photo: LuvlyMikimoto 9/1/07 Botanical Description Salvia officinalis can be used for both culinary and medical needs. Sage generally grows to be approximately a foot tall with leaves one and a half to two inches long. The leaves grow in pairs on the thin stems. Over time the plant eventually becomes woody and much like a shrubbery. All parts of the plant have a strong scent due to the essential oils within them.1 The essential oil is made up of thujone, 1,8-cineole, camphor, borneol, isobutyl acetate, camphene, linalool, alpha- and beta-pinene, viridiflorol, alpa- and beta-caryphyllene. Sage blossoms in August. The flowers are labiate (lip-like) with a light purple, white, or pink color.2 Cultivation Sage grows well in almost all types of garden soil. It thrives in partial shade and warm, dryer soil. Though sage is a perennial, it usually needs to be replanted every few years due to the thinning of the plant.3 Origins The name scientific classification, salvia officinalis comes from the Latin verb salvare meaning to save. It was valued for its healing attributes as illustrated in a common Latin translation, “How can a man die who has Sage in his garden?” Some claim that the Virgin Mary used sage’s “extraordinary virtues” to guide her to Egypt and seek shelter.4 History The Ancients and Arabians considered sage linked to immortality. It was first found northern Mediterranean countries and eventually spread to England, France and Switzerland in the fourteenth century. -

Therapeutic Uses of Peppermint –A Review
Aishwarya Balakrishnan /J. Pharm. Sci. & Res. Vol. 7(7), 2015, 474-476 Therapeutic Uses of Peppermint –A Review Aishwarya Balakrishnan, Saveetha Dental College,Chennai-77 Abstract: Peppermint (Mentha piperita, also known as M. balsamea Willd), is a hybrid mint, a cross between watermint and spearmint. The plant, indigenous to Europe and the Middle East, is now widespread in cultivation in many regions of the world. It is found wild occasionally with its parent species. The concentrated oil of peppermint has a high menthol content. The oil also contains menthone and menthyl esters, particularly menthyl acetate. Dried peppermint typically has volatile oil containing menthol, menthone , menthyl acetate ,menthofuran and 1,8-cineol. Peppermint oil also contains small amounts of many additional compounds including limonene, pulegone, caryophyllene and pinene. According to the German Commission E monographs, peppermint oil (as well as peppermint leaf) has been used internally as an antispasmodic (upper gastrointestinal tract and bile ducts) and to treat irritable bowel syndrome, catarrh of the respiratory tract, and inflammation of the oral mucosa. Externally, peppermint oil has been used for myalgia and neuralgia. According to Commission E, peppermint oil may also act as a carminative, cholagogue, antibacterial, and secretolytic, and it has a cooling action. Enteric-coated peppermint oil capsules (Colpermin) have been used as an orally administered antispasmodic premedication in colonoscopy. Key Words : Mentha piperita, peppermint, menthone. INTRODUCTION: important aromatic and medicinal crops produced in the Peppermint or mentha piperta is a common herb that is U.S. The world production of peppermint oil is about 8000 grown in Europe and north America. -

Hazard Assessment of Glycyrrhizic Acid from Liquorice
VKM Report 2018: 09 Hazard assessment of glycyrrhizic acid from liquorice Opinion of the Panel on Food Additives, Flavourings, Processing Aids, Materials in Contact with Food and Cosmetics of the Norwegian Scientific Committee for Food and Environment Report from the Norwegian Scientific Committee for Food and Environment (VKM) 2018: 09 Hazard assessment of glycyrrhizic acid from liquorice Opinion of Panel on Food Additives, Flavourings, Processing Aids, Materials in Contact with Food and Cosmetics of the Norwegian Scientific Committee for Food and Environment 08.05.2018 ISBN: 978-82-8259-306-9 ISSN: 2535-4019 Norwegian Scientific Committee for Food and Environment (VKM) Po 4404 Nydalen N – 0403 Oslo Norway Phone: +47 21 62 28 00 Email: [email protected] vkm.no vkm.no/English Cover photo: ColourBox Suggested citation: VKM, Inger-Lise Steffensen, Gro Haarklou Mathisen, Ellen Bruzell, Berit Brunstad Granum, Jens Rohloff, Ragna Bogen Hetland (2018) Hazard assessment of glycyrrhizic acid from liquorice. Opinion of the Panel on Food Additives, Flavourings, Processing Aids, Materials in Contact with Food and Cosmetics. ISBN: 978-82-8259-306-9. Norwegian Scientific Committee for Food and Environment (VKM), Oslo, Norway. VKM Report 2018: 09 Hazard assessment of glycyrrhizic acid from liquorice Preparation of the opinion The Norwegian Scientific Committee for Food and Environment (Vitenskapskomiteen for mat og miljø, VKM) appointed a project group to answer the request from the Norwegian Food Safety Authority. The project group consisted of two VKM members of the Panel on Food Additives, Flavourings, Processing Aids, Materials in Contact with Food and Cosmetics and a project leader from the VKM secretariat. -

Featuring Lemon Balm Herbal Water Lillian's
Recipes Featuring Lemon Balm Herbal Water 1 handful of lemon balm ½ handful of pineapple sage ½ handful orange mint ¼ handful mystery herb (like rose, lime basil, or rose scented geranium) in 2 quarts of water Six hours before drinking it, gather the herbs, wash them gently in cold water and place them in a jug of water. Place the jug in the fridge so that is refreshingly chilled for family or guests. For a morning garden tour, make this the night before. Any citrus, pleasant scented geranium, mint or other pleasing herbs can be substituted. © 2009 Lemon Balm: An Herb Society of America Guide, Recipe Karen Langan Lillian's Lemon Noodles 1 cup butter (no substitutions) Blend in: 1½ cups sugar 2¾ cups flour 2 eggs 1 teaspoon cream of tartar 6-8 leaves of lemon balm that have been 1 teaspoon baking soda finely chopped (can put in blender with Zest of one fresh lemon or a tablespoon eggs to be chopped) of dried grated lemon peel 1 teaspoon vanilla Chill batter 1 hour or longer. Roll small balls the size of a cherry or walnut depending on the size of cookie you like; bake at 350°F, 8-12 minutes, till golden. Batter can be kept up to a week covered, in refrigerator. While still warm, frost with small dollop of lemon butter icing. Lemon Butter Icing: Beat one stick of room temperature butter with 1 box 4X sugar. Add the juice of ½ lemon, 1 teaspoon vanilla; beat well. If too stiff, add a drop or two of milk. -
Using Garden Sage Wisely
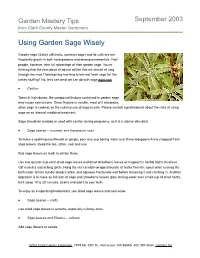
Garden Mastery Tips September 2003 from Clark County Master Gardeners Using Garden Sage Wisely Garden sage (Salvia officinalis, common sage) and its cultivars are frequently grown in both herb gardens and among ornamentals. Few people, however, take full advantage of their garden sage. You’re thinking that the next piece of advice will be that we should all slog through the mud Thanksgiving morning to harvest fresh sage for the turkey stuffing? No, let’s see what we can do with sage right now. ♦ Caution Taken in high doses, the compound thujone contained in garden sage may cause convulsions. Since thujone is volatile, most of it dissipates when sage is cooked, so the culinary use of sage is safe. Please consult a professional about the risks of using sage as an internal medicinal treatment. Sage should be avoided or used with caution during pregnancy, as it is a uterine stimulant. ♦ Sage Leaves – cosmetic and therapeutic uses To make a soothing mouthwash or gargle, pour one cup boiling water over three teaspoons finely chopped fresh sage leaves, steep the tea, strain, cool and use. Rub sage leaves on teeth to whiten them. Use one quarter cup each dried sage leaves and dried strawberry leaves or mugwort in herbal baths to relieve stiff muscles and aching joints. Hang the cheesecloth-wrapped bundle of herbs from the spout while running the bath water, let the bundle steep a while, and squeeze the bundle well before removing it and climbing in. Another approach is to make an infusion of sage and strawberry leaves (pour boiling water over a half-cup of dried herbs; let it steep 10 to 20 minutes; strain) and add it to your bath. -

The Chemotaxonomy of Common Sage (Salvia Officinalis)
medicines Article The Chemotaxonomy of Common Sage (Salvia officinalis) Based on the Volatile Constituents Jonathan D. Craft, Prabodh Satyal and William N. Setzer * Department of Chemistry, University of Alabama in Huntsville, Huntsville, AL 35899, USA; [email protected] (J.D.C.); [email protected] (P.S.) * Correspondence: [email protected]; Tel.: +1-256-824-6519 Academic Editors: João Rocha and James D. Adams Received: 2 May 2017; Accepted: 26 June 2017; Published: 29 June 2017 Abstract: Background: Common sage (Salvia officinalis) is a popular culinary and medicinal herb. A literature survey has revealed that sage oils can vary widely in their chemical compositions. The purpose of this study was to examine sage essential oil from different sources/origins and to define the possible chemotypes of sage oil. Methods: Three different samples of sage leaf essential oil have been obtained and analyzed by GC-MS and GC-FID. A hierarchical cluster analysis was carried out on 185 sage oil compositions reported in the literature as well as the three samples in this study. Results: The major components of the three sage oils were the oxygenated monoterpenoids α-thujone (17.2–27.4%), 1,8-cineole (11.9–26.9%), and camphor (12.8–21.4%). The cluster analysis revealed five major chemotypes of sage oil, with the most common being a α-thujone > camphor > 1,8-cineole chemotype, of which the three samples in this study belong. The other chemotypes are an α-humulene-rich chemotype, a β-thujone-rich chemotype, a 1,8-cineole/camphor chemotype, and a sclareol/α-thujone chemotype. -

Herbs and Spices
Herbs and Spices spices bo bs and ost flav Shop and Save Her or, Fresh or Dried? - and < In bulk foods, you can buy a are salt sugar-f Both fresh and dried herbs add nd ree! small amount to use while the a flavor. Adjust amounts to your flavor is strongest. Or try taste. something new. Most Herbs: < Check for a “BEST by” date 3 teaspoons fresh = on packaged spices and herbs. 1 They are still safe after the date teaspoon dried but the flavor will be weaker. Garlic: 1 clove fresh = < Fresh herbs should be a color ¼ teaspoon garlic powder typical for the herb. Avoid Ginger: 1 teaspoon wilted or yellowed leaves. fresh ginger root = < If you garden, grow some ¼ teaspoon ground herbs. Try basil, parsley, chives ginger powder and others in the ground or a container. I Whole dried spices keep their a bowl of water; lift out flavor for up to 4 years; ground of the water; repeat in fresh ore We spices for 2 to 3 years and dried water until no dirt appears in St ll herbs for 1 to 3 years. Smell them the bowl. ste Le to check for strength of flavor. I Freeze fresh herbs and use in a ss I Refrigerate fresh herbs like W cooked dishes within one year. parsley, basil or cilantro upright Remove clean, dry leaves from I Store dried herbs and spices in in a glass of water like flowers. main stems, spread on a tray a cool, dark location away from Cover with a loose plastic bag. -

Glycyrrhiza Glabra (Liquorice) - a Potent Medicinal Herb Received: 13-04-2014 Accepted: 20-05-2014 Monica Damle
International Journal of Herbal Medicine 2014; 2(2): 132-136 ISSN 2321-2187 Glycyrrhiza glabra (Liquorice) - a potent medicinal herb IJHM 2014; 2(2): 132-136 Received: 13-04-2014 Accepted: 20-05-2014 Monica Damle Monica Damle Abstract SVKM’s Dr. Bhanuben Nanavati There is an increasing demand for herbal medicines, health products, pharmaceuticals. Glycyrrhiza College of Pharmacy glabra Linn is a plant used in traditional medicine across the world for its ethnopharmacological value. It Gate No.1, 1st Floor, is found to contain important phytoconstituents such as glycyrrhizin, glycyrrhizinic acid, glabrin A and B Mithibai College Campus, and isoflavones. It is effectively used as anti-inflammatory, anti-bacterial, anti-fungal, anti-diabetic, anti- V.M. Road , viral, anti-ulcer, antitussive, anti-oxidant, skin whitening, anti-diuretic agent. The present article is an Vile Parle (West), effort to compile the available literature on Glycyrrhiza glabra with respect to its traditional uses, Mumbai 400 056, India. bioactive constituents and pharmacologic activities. This may be useful in discovering potential therapeutic effects and developing new formulations. Keywords: Glycyrrhiza glabra, glycyrrhizin, antitussive, anti-oxidant, skin lightening 1. Introduction Incontrovertibly there are worldwide changes in healthcare industry in the third millennium. Ayurvedic system of healthcare has gained importance and is becoming popular. It is a comprehensive system of healthcare that originated in India. Because of the effectiveness and less adverse reactions compared to the synthetic chemicals, Ayurvedic system has attained popularity globally. The classical text of Ayurveda mentions number of plants for the management of several diseases. Undoubtedly several researchers had given their contributions for finding hidden therapeutic potentials of number of Ayurvedic drugs, but still number of plants need a comprehensive study on them. -

Glycyrrhiza Glabra) Herb As a Feed Additive in Poultry: Current Knowledge and Prospects
animals Review Use of Licorice (Glycyrrhiza glabra) Herb as a Feed Additive in Poultry: Current Knowledge and Prospects Mahmoud Alagawany 1,* , Shaaban S. Elnesr 2 , Mayada R. Farag 3, Mohamed E. Abd El-Hack 1 , Asmaa F. Khafaga 4, Ayman E. Taha 5, Ruchi Tiwari 6, Mohd. Iqbal Yatoo 7 , Prakash Bhatt 8, Gopi Marappan 9 and Kuldeep Dhama 10,* 1 Department of Poultry, Faculty of Agriculture, Zagazig University, Zagazig 44511, Egypt 2 Department of Poultry Production, Faculty of Agriculture, Fayoum University, Fayoum 63514, Egypt 3 Forensic Medicine and Toxicology Department, Faculty of Veterinary Medicine, Zagazig University, Zagazig 44511, Egypt 4 Department of Pathology, Faculty of Veterinary Medicine, Alexandria University, Edfina 22758, Egypt 5 Department of Animal Husbandry and Animal Wealth Development, Faculty of Veterinary Medicine, Alexandria University, Edfina 22758, Egypt 6 Department of Veterinary Microbiology and Immunology, College of Veterinary Sciences, UP Pandit Deen Dayal Upadhayay Pashu Chikitsa Vigyan Vishwavidyalay Evum Go-Anusandhan Sansthan (DUVASU), Mathura-281001, Uttar Pradesh, India 7 Division of Veterinary Clinical Complex, Faculty of Veterinary Sciences and Animal Husbandry, Jammu and Kashmir, Srinagar 190006, India 8 Teaching Veterinary Clinical Complex, College of Veterinary and Animal Sciences, Govind Ballabh Pant University of Agriculture and Technology, Pantnagar-263145 (Udham Singh Nagar), Uttarakhand, India 9 Division of Avian Physiology and Reproduction, ICAR-Central Avian Research Institute, Izatnagar, -

Belgian Week of Gastroenterology 2019 Belgian Association for The
Belgian Week of Gastroenterology 2019 http://www.bwge.be Belgian Association for the Study of the Liver (BASL) / Belgian Liver Intestine Committee (BLIC) A01 The sPDGFR-beta containing PRTA-score is a novel diagnostic algorithm for significant liver fibrosis in patients with viral, alcoholic, and metabolic liver disease J. LAMBRECHT (1), S. VERHULST (1), I. MANNAERTS (1), J. SOWA (2), J. BEST (2), A. CANBAY (2), H. REYNAERT (1), L. VAN GRUNSVEN (1) / [1] Vrije Universiteit Brussel (VUB), Jette, Belgium, Department of Basic Biomedical Sciences, Liver Cell Biology Laboratory, [2] University Hospital Magdeburg, , Germany, Department of Gastroenterology, Hepatology and Infectious Diseases Introduction: Diagnosis of liver fibrosis onset and regression remains a controversial subject in the current clinical setting, as the gold standard remains the invasive liver biopsy. Multiple novel non-invasive markers have been proposed but lack sufficient sensitivity and specificity for diagnosis of early stage liver fibrosis. Platelet Derived Growth Factor Receptor beta (PDGFRβ) has been associated to hepatic stellate cell activation and has been the target of multiple therapeutic studies. However, little is known concerning its use as a diagnostic agent. Aim: In this study, we analysed the diagnostic potential of PDGFRβ for liver fibrosis in a heterogenous patient population. Methods: The study cohort consisted of 148 patients with liver fibrosis/cirrhosis due to various causes of liver injury (metabolic, alcoholic, viral), and 14 healthy individuals as control population. A validation cohort of 57 patients with metabolic liver disease, who underwent liver biopsy to stage fibrosis, were gathered. Circulating soluble PDGFRβ (sPDGFRβ) levels were determined using a commercial ELISA kit. -

RIVM Report 340630001 the Health and Addiction Risk of the Glycyrrhizic
RIVM report 340630001/2003 The health and addiction risk of the glycyrrhizic acid component of liquorice root used in tobacco products I. van Andel, G. Wolterink, G. van de Werken, H. Stevenson, L.A.G.J.M. van Aerts, and W. Vleeming This investigation is carried out for the account of the Directorate for Public Health of the Ministry of Health, Welfare and Sports and of the Inspectorate for Health Protection and Veterinary Public Health, within the framework of project 340630 RIVM, P.O. Box 1, 3720 BA Bilthoven, telephone: 31 - 30 - 274 91 11; telefax: 31 - 30 - 274 29 71 RIVM report 340630001 page 2 of 35 Abstract Reported here is the evaluation of the health effects and possible addictive effects of liquorice preparations as a conditioning and flavouring agent in tobacco products. Based on the literature survey, the evaluation describes the exposure to, and the pharmacology, pharmacokinetics and toxicology of glycyrrhizic acid, the main biologically active component of liquorice preparations. The report also goes into the addictive aspects of glycyrrhizic acid. The level of glycyrrhizic acid in cigarette smoke or in tobacco products is not known. Furthermore, it is improbable that the intake of glycyrrhizic acid during cigarette smoking will exceed the daily oral intake. A point of concern is the nature of the combustion products formed during cigarette smoking. It is unlikely that smoking-related exposure to glycyrrhizic acid will increase mineralocorticoid activity and result under some conditions in hypertension. The statement that glycyrrhizic acid acts as a bronchodilatator could not be confirmed from the currently available literature.