DOWNLOAD STOMAEDUJ Volume 4, Issue 2 – 2017
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

(Alias Walter Lam Or Lam San Ping). A-5366278, Yokoya, Yoshi Or Sei Cho Or Shiqu Ono Or Yoshi Mori Or Toshi Toyoshima
B44 CONCURRENT RESOLUTIONS—MAY 23, 1951 [65 STAT. A-3726892, Yau, Lam Chai or Walter Lum or Lum Chai You (alias Walter Lam or Lam San Ping). A-5366278, Yokoya, Yoshi or Sei Cho or Shiqu Ono or Yoshi Mori or Toshi Toyoshima. A-7203890, Young, Choy Shie or Choy Sie Young or Choy Yong. A-96:87179, Yuen, Wong or Wong Yun. A-1344004, Yunger, Anna Steibel or Anna Kirch (inaiden name). A-2383005, Zainudin, Yousuf or Esouf Jainodin or Eusoof Jainoo. A-5819992, Zamparo, Frank or Francesco Zamparo. A-5292396, Zanicos, Kyriakos. A-2795128, Zolas, Astghik formerly Boyadjian (nee Hatabian). A-7011519, Zolas, Edward. A-7011518, Zolas, Astghik Fimi. A-4043587, Zorrilla, Jesus Aparicio or Jesus Ziorilla or Zorrilla. A-7598245, Mora y Gonzales, Isidoro Felipe de. Agreed to May 23, 1951. May 23, 1951 [S. Con. Res. 10] DEPORTATION SUSPENSIONS Resolved hy the Senate (the House of Representatives concurrmgr), That the Congress favors the suspension of deportation in the case of each alien hereinafter named, in which case the Attorney General has suspended deportation for more than six months: A-2045097, Abalo, Gelestino or George Abalo or Celestine Aballe. A-5706398, Ackerman, 2Jelda (nee Schneider). A-4158878, Agaccio, Edmondo Giuseppe or Edmondo Joseph Agaccio or Joe Agaccio or Edmondo Ogaccio. A-5310181, Akiyama, Sumiyuki or Stanley Akiyama. A-7112346, Allen, Arthur Albert (alias Albert Allen). A-6719955, Almaz, Paul Salin. A-3311107, Alves, Jose Lino. A-4736061, Anagnostidis, Constantin Emanuel or Gustav or Con- stantin Emannel or Constantin Emanuel Efstratiadis or Lorenz Melerand or Milerand. A-744135, Angelaras, Dimetrios. -

Icnaam 2020 Conference
ICNAAM 2020 CONFERENCE VIRTUAL PARTICIPATION PROGRAM 17 September 2020 Virtual Room 1 08.50-09.00 Opening Ceremony Professor Dr. T.E. Simos (Chairman) Please note that Greek timezone is :(GMT+3) : Time now in Greece (Click Here) - 2 - 17 September 2020 Virtual Room 1 THE TENTH SYMPOSIUM ON ADVANCED COMPUTATION AND INFORMATION Session Name: IN NATURAL AND APPLIED SCIENCES Chair Name: Dr. Claus-Peter Rückemann Program: Hours Paper Title Author Claus-Peter 09.00-09.05 Welcome Notes Rückemann Keynote Lecture / Information Science and Structure: Claus-Peter 09.05-09.50 Beware – Ex Falso Quod Libet Rückemann Information Science Approaches to Sustainable Claus-Peter 09.50-10.25 Structures: Rhodos Case Results From Knowledge and Rückemann Mining 10.25-11.00 Mathematics in the Heart of Brunelleschi’s Dome Raffaella Pavani Session Recent advances in nonlinear partial differential equations and systems and their Name: applications Chair Name: G. R. Cirmi, S. D'Asero, S. Leonardi Program: Sept. 17 Hours Paper Title Author 11.00-11.30 On a class of nonlinear partial differential equations of parabolic type M. M. Porzio 11.35-12.05 Scalar and vectorial degenerate elliptic problems F. Leonetti 12.10-12.40 On some singular elliptic systems in R^N S. A. Marano THE BOTTARO-MARINA SLICE METHOD FOR DISTRIBUTIONAL 12.45-13.15 SOLUTIONS TO ELLIPTIC EQUATIONS WITH DRIFT TERM S. Buccheri Please note that Greek timezone is :(GMT+3) : Time now in Greece (Click Here) - 3 - Session Name: Statistical Inference in Copula Models and Markov Processes V Chair Name: Veronica Andrea Gonzalez-Lopez Program: Hours Paper Title Author A Stochastic Inspection about Genetic Variants of Jesús E. -

Códigos De Las Ayudas Concedidas
FECHA: 28/05/2020 CÓDIGOS DE LAS AYUDAS CONCEDIDAS CODIGO AYUDA DESCRIPCION AYUDA 2 Beca Básica 3 Cuantía Fija Ligada a la Renta 4 Cuantía Fija Ligada a la Residencia 5-1 Excelencia Académica entre 8 y 8.49 5-2 Excelencia Académica entre 8.50 y 8.99 5-3 Excelencia Académica entre 9 y 9.49 5-4 Excelencia Académica 9.50 o más 6 Cuantía variable mínima 7 Cuantía variable 8 Suplemento transporte marítimo/aéreo entre islas (para domiciliados en Tenerife, Gran Canaria o Mallorca) y entre Ceuta/Melilla y Península 9 Suplemento transporte marítimo/aéreo entre islas (para domiciliados en Lanzarote, Fuerteventura, Gomera, Hierro, La Palma, Menorca, Ibiza y Formentera) 10 Suplemento para transporte marítimo/aéreo a la Península para domiciliados en Baleares 11 Suplemento para transporte marítimo/aéreo a la Península para domiciliados en Canarias PAG: 1 de 407 RELACIÓN ALFABÉTICA DE BECARIOS CON LAS AYUDAS CONCEDIDAS FECHA: 28/05/2020 SANTA CRUZ DE TENERIFE CURSO: 2019-2020 CONVOCATORIA: General APELLIDOS - NOMBRE NIF/NIE AYUDAS IMPORTE TOTAL AABIDA ETTABTI, KARIMA ***4430** 3, 7 2.284,01 € AAGUIED SANNAD, MOHAMED ***9737** 3, 7 2.127,75 € ABAD HUME, SINEAD ***8124** 2, 5-2 275,00 € ABAD MARTIN, IRENE ANMARI ***0853** 3, 5-2, 7 2.589,39 € ABAD MARTIN, MERIEM ***0853** 3, 4, 7 4.848,38 € ABAD MARTIN, NIEVES MARIA ***0853** 3, 4, 7 4.874,50 € ABAD MARTÍN, EMILIO ***5943** 2, 7 715,40 € ABAD MESA, LAURA ***4075** 3, 7 2.111,16 € ABAD ROSQUETE, NELSON ***8529** 2, 7 663,02 € ABAD VELÁZQUEZ, RUT ***4191** 2, 5-2, 7 751,17 € ABALLA, HASNA ****0161* 3, -
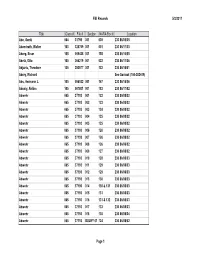
5/3/2011 FBI Records Page 1 Title Class # File # Section NARA Box
FBI Records 5/3/2011 Title Class # File # Section NARA Box # Location Abe, Genki 064 31798 001 039 230 86/05/05 Abendroth, Walter 100 325769 001 001 230 86/11/03 Aberg, Einar 105 009428 001 155 230 86/16/05 Abetz, Otto 100 004219 001 022 230 86/11/06 Abjanic, Theodore 105 253577 001 132 230 86/16/01 Abrey, Richard See Sovloot (100-382419) Abs, Hermann J. 105 056532 001 167 230 86/16/06 Abualy, Aldina 105 007801 001 183 230 86/17/02 Abwehr 065 37193 001 122 230 86/08/02 Abwehr 065 37193 002 123 230 86/08/02 Abwehr 065 37193 003 124 230 86/08/02 Abwehr 065 37193 004 125 230 86/08/02 Abwehr 065 37193 005 125 230 86/08/02 Abwehr 065 37193 006 126 230 86/08/02 Abwehr 065 37193 007 126 230 86/08/02 Abwehr 065 37193 008 126 230 86/08/02 Abwehr 065 37193 009 127 230 86/08/02 Abwehr 065 37193 010 128 230 86/08/03 Abwehr 065 37193 011 129 230 86/08/03 Abwehr 065 37193 012 129 230 86/08/03 Abwehr 065 37193 013 130 230 86/08/03 Abwehr 065 37193 014 130 & 131 230 86/08/03 Abwehr 065 37193 015 131 230 86/08/03 Abwehr 065 37193 016 131 & 132 230 86/08/03 Abwehr 065 37193 017 133 230 86/08/03 Abwehr 065 37193 018 135 230 86/08/04 Abwehr 065 37193 BULKY 01 124 230 86/08/02 Page 1 FBI Records 5/3/2011 Title Class # File # Section NARA Box # Location Abwehr 065 37193 BULKY 20 127 230 86/08/02 Abwehr 065 37193 BULKY 33 132 230 86/08/03 Abwehr 065 37193 BULKY 33 132 230 86/08/03 Abwehr 065 37193 BULKY 33 133 230 86/08/03 Abwehr 065 37193 BULKY 35 134 230 86/08/03 Abwehr 065 37193 EBF 014X 123 230 86/08/02 Abwehr 065 37193 EBF 014X 123 230 86/08/02 Abwehr -

Nicolau De Cusa: Olhar E Mística Nicholas of Cusa: Look and Mystic Maria Simone Marinho NOGUEIRA 1
Nicolau de Cusa: Olhar e Mística Nicholas of Cusa: Look and Mystic Maria Simone Marinho NOGUEIRA 1 Resumo : Partindo do pressuposto de que o De visione dei é um texto de caráter místico e tendo por base que a mística, na sua designação geral e em última instância, é uma experiência do divino, pensamos ser possível mostrar que, nesse opúsculo, Nicolau de Cusa (1401-1464) apresenta uma experiência mística, entendida no sentido de uma reflexão sobre o tema. Deste modo, a experiência sensível proposta por ele, e explicada no Prefácio do De visione dei , une a simplicidade de uma experiência visual com a mais alta e profunda especulação que o ser humano pode fazer: refletir de forma que possa experienciar sua relação com o divino. Abstract : Assuming that De visione dei is a mystical text and that the mystic, both in its generic and ultimate interpretations, is an experience of the divine, we think it is possible to show that, at the mentioned publication, Nicholas of Cusa (1401-1464) presents a mystical experience, understood as the reflection about the subject. Therefore, the sensible experience proposed by him, and explained in the Preface of De visione dei , unites the simplicity of a visual experience with the highest and most profound speculation that human beings can do: reflect in a manner that you can experience your relationship with the divine. Palavras-chave : Experiência – Reflexão – Olhar – Amar – Mística. Keywords : Experience – Reflection – Look – Love – Mystic. 1 Professora Doutora de Filosofia Medieval da Universidade Estadual da Paraíba. Professora Colaboradora do Programa de Pós-Graduação (Mestrado) em Filosofia da Universidade Federal da Paraíba. -

Possest: Indicações Para Se Pensar a Relacionalidade Do Princípio Em
Possest: indicações para se pensar a relacionalidade do princípio em Nicolau de Cusa Possest: indicaciones para pensarmos la relacionalidad del principio en Nicolás de Cusa Possest: indications for thinking relationality principle in Nicholas of Cusa José TEIXEIRA NETO1 Resumo: Com o termo possest esperamos alcançar aquele nome que, como os outros nomes divinos, conduzem à compreensão do princípio. Nesse caso, de modo mais específico, acreditamos que o possest indica, enquanto enigma, a trindade do princípio e mais ainda conduz aquele especula ao nexus que se mostra como elemento fundamental para a compreensão dessa mesma unitrinidade e, por isso mesmo, à ideia de que o princípio primeiro é em si mesmo relacional. Dentre todas as obras cusanas o termo “possest” aparecerá apenas em três textos do chamado “período tardio”. As duas últimas aparições do termo em questão se dão no De apice theoriae (1464) provavelmente a última obra escrita por Nicolau de Cusa. Por sua vez, no De venatione sapientiae (1463) o possest será considerado o segundo campo, logo após o da douta ignorância e antes do non aliud, no qual se dá a caça da sabedoria. As temáticas retomadas no De venatione sapientiae foram profundamente abordadas no De possest (1460) que se constitui como um “diálogo a três” entre Nicolau de Cusa, Bernardo de Krayburg, chanceler do Arcebispo de Salzburgo, e João André Vigévio, secretário do Cardeal e depois bispo de Aleria. Abstract: We hope to achieve with the term possest one name, like other divine names, leading to the understanding of the principle. In this case, more specifically, we believe that possest indicates as enigma, the trinity of principle and further speculates that leads to the nexus that shows how key element to understanding this same unitrinity and, therefore, the idea of the first principle in itself is relational. -

Eu Whoiswho Official Directory of the European Union
EUROPEAN UNION EU WHOISWHO OFFICIAL DIRECTORY OF THE EUROPEAN UNION EUROPEAN COMMISSION 16/09/2021 Managed by the Publications Office © European Union, 2021 FOP engine ver:20180220 - Content: - merge of files"Commission_root.xml", "The_College.XML1.5.xml", "temp/CRF_COM_CABINETS.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/CRF_COM_SG.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/ CRF_COM_SJ.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/CRF_COM_COMMU.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/CRF_COM_IDEA.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/CRF_COM_BUDG.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/ CRF_COM_HR.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/CRF_COM_DIGIT.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/CRF_COM_IAS.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/CRF_COM_OLAF.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/ CRF_COM_ECFIN.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/CRF_COM_GROW.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/CRF_COM_DEFIS.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/CRF_COM_COMP.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/ CRF_COM_EMPL.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/CRF_COM_AGRI.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/CRF_COM_MOVE.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/CRF_COM_ENER.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/ CRF_COM_ENV.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/CRF_COM_CLIMA.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/CRF_COM_RTD.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/CRF_COM_CNECT.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", "temp/ CRF_COM_JRC.RNS.FX.TRAD.DPO.dated.XML1.5.ANN.xml", -

Brian Mckinlay November, 2002 Contents Introduction
A BIBLIOGRAPHY OF WORKS BY NIKOLAI ALEXANDROVICH BERDYAEV (1874– 1948) AND ABOUT HIM AND HIS WORK. Brian McKinlay November, 2002 Contents Introduction 1 1 Primary sources in English 1.1 Published pre-1948 2 1.2 Posthumous English language publications, post 1948 8 2. Secondary sources in English and other Western European languages1 9 Introduction This bibliography grew out research for my Bachelor of Theology (Honours) dissertation, “By Method of Witness: Revelation in Nicholas Berdyaev’s Religious Philosophy”, Charles Sturt University, 2002. I tried comprehensively to identify translations of Berdyaev’s writings into English and secondary materials in English about Berdyaev and his work. This bibliography lists 130 English translations of Berdyaev and 422 secondary sources in English and other Western European languages.2 This partly duplicates the work of others, as there are standard bibliographies of primary Berdyaev materials and of secondary materials to 1992.3 However these were published in very limited runs and are almost unobtainable from libraries or through the used book trade. The list of primary sources relies considerably on Stephen Janos’s listing of translations of Berdyaev into English, including his own.4 Vallon also has a significant bibliography, especially of primary works, in his 1960 biography of Berdyaev.5 I have added some items found elsewhere. My listing of secondary materials began with a series of searches of electronic bibliographic 1 Catalan, Finnish, French, German, Italian, Norwegian, Portugese, Spanish and Swedish 2 The format of the Appendix and the bibliographic standards for the essay proper are based closely on: Charles Sturt University. Division of Library Services. -

The Afro-Portuguese Maritime World and The
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by ETD - Electronic Theses & Dissertations THE AFRO-PORTUGUESE MARITIME WORLD AND THE FOUNDATIONS OF SPANISH CARIBBEAN SOCIETY, 1570-1640 By David Wheat Dissertation Submitted to the Faculty of the Graduate School of Vanderbilt University in partial fulfillment of the requirements for the degree in DOCTOR OF PHILOSOPHY in History August, 2009 Nashville, Tennessee Approved: Jane G. Landers Marshall C. Eakin Daniel H. Usner, Jr. David J. Wasserstein William R. Fowler Copyright © 2009 by John David Wheat All Rights Reserved For Sheila iii ACKNOWLEDGEMENTS This dissertation could not have been completed without support from a variety of institutions over the past eight years. As a graduate student assistant for the preservation project “Ecclesiastical Sources for Slave Societies,” I traveled to Cuba twice, in Summer 2004 and in Spring 2005. In addition to digitizing late-sixteenth-century sacramental records housed in the Cathedral of Havana during these trips, I was fortunate to visit the Archivo Nacional de Cuba. The bulk of my dissertation research was conducted in Seville, Spain, primarily in the Archivo General de Indias, over a period of twenty months in 2005 and 2006. This extended research stay was made possible by three generous sources of funding: a Summer Research Award from Vanderbilt’s College of Arts and Sciences in 2005, a Fulbright-IIE fellowship for the academic year 2005-2006, and the Conference on Latin American History’s Lydia Cabrera Award for Cuban Historical Studies in Fall 2006. Vanderbilt’s Department of History contributed to my research in Seville by allowing me one semester of service-free funding. -

Individual Start List IRONMAN70.3 Barcelona 2021 (Last Update: July 19Th, 2021) Startlist Will Be Updated Once a Month
Individual Start List IRONMAN70.3 Barcelona 2021 (Last update: July 19th, 2021) Startlist will be updated once a month Last name First name Age Group Country Represented AWA TriClub Beaver Ella F18-24 GBR (United Kingdom) Canals Suñé Paula F18-24 ESP (Spain) Chapman-Hammond Evie F18-24 GBR (United Kingdom) Sisu Racing Coiffé Nadège F18-24 FRA (France) Coutinho Anneline F18-24 FRA (France) AWA Silver Dahan Carla F18-24 FRA (France) AWA Gold Team Nissa Triathlon Duvoisin Loanne F18-24 CHE (Switzerland) Gillard Deborah F18-24 BEL (Belgium) Orts Albane F18-24 BEL (Belgium) Seutin Zoé F18-24 BEL (Belgium) Sheldon Libby F18-24 ESP (Spain) Sikk Sigrid F18-24 EST (Estonia) Vangeneugden Sara F18-24 BEL (Belgium) Vanheiss Manon F18-24 FRA (France) Walters Jessie F18-24 GBR (United Kingdom) Abades Barclay Fiona F25-29 ESP (Spain) Abbas Aya F25-29 EGY (Egypt) Alcover Carmen F25-29 ESP (Spain) Moove All1 Anderson Kelly F25-29 ESP (Spain) Aranguri Maria Alejandra F25-29 PER (Peru) Argerich Bergadà Sara F25-29 ESP (Spain) Betegon Bleye Maria Teresa F25-29 ESP (Spain) Bohnenkamp Judith F25-29 ESP (Spain) Brand Rachel F25-29 GBR (United Kingdom) Bravaia Iana F25-29 RUS (Russian Federation) Bühler Lora F25-29 CHE (Switzerland) If your club is not listed, please log into your IRONMAN Account and connect your IRONMAN Athlete Profile with your club. If you are not able to find your club, please contact [email protected] for help Individual Start List IRONMAN70.3 Barcelona 2021 (Last update: July 19th, 2021) Startlist will be updated once a month Last name First name Age Group Country Represented AWA TriClub Bux Aalya F25-29 AUS (Australia) Cardus Agra Aida F25-29 ESP (Spain) Casado Rayo Estefanía F25-29 ESP (Spain) TRIENJOY TEAM Catley-Davies Megan F25-29 GBR (United Kingdom) Caudrelier Manon F25-29 FRA (France) AWA Bronze Elwood Rachel F25-29 GBR (United Kingdom) Escoda Ribo Marta F25-29 ESP (Spain) Escriba Planes Marina F25-29 ESP (Spain) Estival Garcia Monica F25-29 ESP (Spain) C.E. -
FY20 Old to New Values
PID OWNER NAME ST NUMBER STREET PREVIOUS ASSESSMENT PREVIOUS ASSESSMENT 1515 GRIFFIN GERALD T. (TE) 8 A ST 288,200 310,600 1516 NAMVAR NAZANIN (TE) 12 A ST 332,500 338,500 1379 SNYER WILLIAM R 13 A ST 468,300 457,000 1374 SUPRENANT SCOTT 18 A ST 204,100 214,900 1378 BREAULT DAVID R. & KAREN A., TRUSTEES 23 A ST 313,100 322,300 1373 DOWLING JOHN T (TE) 24 A ST 274,100 289,000 1371 LOUANGPHIXAI LILA L. (JTRS) 30 A ST 271,800 301,100 1514 PATTEN KAREN 38 A ST 346,300 343,500 11167 RYCHALSKY, ERIN J 65 A ST 356,500 381,900 1203 RIVERA ANDRES 71 A ST 366,300 387,600 1484 SCARVALAS GARY J 72 A ST 39,200 41,200 1485 MALCOLM DONNA J 76 A ST 39,200 41,200 1202 BEAUDOIN RONALD & BRENDA, TSTS 77 A ST 294,600 303,000 1201 APONTE, KIMBERLY L 83 A ST 316,200 341,700 1483 TOWN OF DRACUT 88 A ST 112,000 117,600 1482 KRUGH KENNETH W. (JTRS) 90 A ST 290,200 312,800 1191 BAILEY PAUL R 92 A ST 303,000 309,400 1200 KIGGUNDU SEPIRIA (TE) 93 A ST 272,000 326,300 1199 FITZGERALD RAYMOND J.(TE) 95 A ST 275,300 296,800 1190 PROVOST ALAN MICHAEL 98 A ST 249,000 254,600 1198 DARES KIMBERLY JEAN IND. 101 A ST 277,300 302,800 11649 COGAN MICHAEL (TE) 104 A ST 284,700 306,700 997 MELLO JEFFREY A. -
Croi 2021 Program Committee
General Information CONTENTS WELCOME . 2 General Information General Information OVERVIEW . 2 CONTINUING MEDICAL EDUCATION . 3 CONFERENCE SUPPORT . 4 VIRTUAL PLATFORM . 5 ON-DEMAND CONTENT AND WEBCASTS . 5 CONFERENCE SCHEDULE AT A GLANCE . 6 PRECONFERENCE SESSIONS . 9 LIVE PLENARY, ORAL, AND INTERACTIVE SESSIONS, AND ON-DEMAND SYMPOSIA BY DAY . 11 SCIENCE SPOTLIGHTS™ . 47 SCIENCE SPOTLIGHT™ SESSIONS BY CATEGORY . 109 CROI FOUNDATION . 112 IAS–USA . 112 CROI 2021 PROGRAM COMMITTEE . 113 Scientific Program Committee . 113 Community Liaison Subcommittee . 113 Former Members . 113 EXTERNAL REVIEWERS . .114 SCHOLARSHIP AWARDEES . 114 AFFILIATED OR PROXIMATE ACTIVITIES . 114 EMBARGO POLICIES AND SOCIAL MEDIA . 115 CONFERENCE ETIQUETTE . 115 ABSTRACT PROCESS Scientific Categories . 116 Abstract Content . 117 Presenter Responsibilities . 117 Abstract Review Process . 117 Statistics for Abstracts . 117 Abstracts Related to SARS-CoV-2 and Special Study Populations . 117. INDEX OF SPECIAL STUDY POPULATIONS . 118 INDEX OF PRESENTING AUTHORS . .122 . Version 9 .0 | Last Update on March 8, 2021 Printed in the United States of America . © Copyright 2021 CROI Foundation/IAS–USA . All rights reserved . ISBN #978-1-7320053-4-1 vCROI 2021 1 General Information WELCOME TO vCROI 2021 Welcome to vCROI 2021! The COVID-19 pandemic has changed the world for all of us in so many ways . Over the past year, we have had to put some of our HIV research on hold, learned to do our research in different ways using different tools, to communicate with each other in virtual formats, and to apply the many lessons in HIV research, care, and community advocacy to addressing the COVID-19 pandemic . Scientists and community stakeholders who have long been engaged in the endeavor to end the epidemic of HIV have pivoted to support and inform the unprecedented progress made in battle against SARS-CoV-2 .