Mindanaohealth Project Program Year 6 Accomplishment Report (October 2017- September 2018)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
POPCEN Report No. 3.Pdf
CITATION: Philippine Statistics Authority, 2015 Census of Population, Report No. 3 – Population, Land Area, and Population Density ISSN 0117-1453 ISSN 0117-1453 REPORT NO. 3 22001155 CCeennssuuss ooff PPooppuullaattiioonn PPooppuullaattiioonn,, LLaanndd AArreeaa,, aanndd PPooppuullaattiioonn DDeennssiittyy Republic of the Philippines Philippine Statistics Authority Quezon City REPUBLIC OF THE PHILIPPINES HIS EXCELLENCY PRESIDENT RODRIGO R. DUTERTE PHILIPPINE STATISTICS AUTHORITY BOARD Honorable Ernesto M. Pernia Chairperson PHILIPPINE STATISTICS AUTHORITY Lisa Grace S. Bersales, Ph.D. National Statistician Josie B. Perez Deputy National Statistician Censuses and Technical Coordination Office Minerva Eloisa P. Esquivias Assistant National Statistician National Censuses Service ISSN 0117-1453 FOREWORD The Philippine Statistics Authority (PSA) conducted the 2015 Census of Population (POPCEN 2015) in August 2015 primarily to update the country’s population and its demographic characteristics, such as the size, composition, and geographic distribution. Report No. 3 – Population, Land Area, and Population Density is among the series of publications that present the results of the POPCEN 2015. This publication provides information on the population size, land area, and population density by region, province, highly urbanized city, and city/municipality based on the data from population census conducted by the PSA in the years 2000, 2010, and 2015; and data on land area by city/municipality as of December 2013 that was provided by the Land Management Bureau (LMB) of the Department of Environment and Natural Resources (DENR). Also presented in this report is the percent change in the population density over the three census years. The population density shows the relationship of the population to the size of land where the population resides. -
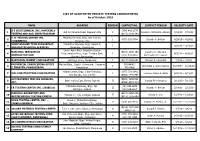
III III III III LIST of ACCREDITED PRIVATE TESTING LABORATORIES As of October 2019
LIST OF ACCREDITED PRIVATE TESTING LABORATORIES As of October 2019 NAME ADDRESS REGION CONTACT NO. CONTACT PERSON VALIDITY DATE A’S GEOTECHNICAL INC. MATERIALS (074) 442-2775 1 Old De Venecia Road, Dagupan City I Dioscoro Richard B. Alviedo 7/16/19 – 7/15/21 TESTING AND SOIL INVESTIGATION (0917) 1141-343 E. B. TESTING CENTER INC. McArthur Hi-way, Brgy. San Vicente, 2 I (075) 632-7364 Elnardo P. Bolivar 4/29/19 – 4/28/21 (URDANETA) Urdaneta City JORIZ GROUND TECH SUBSURFACE MacArthur Highway, Brgy. Surabnit, 3 I 3/20/18 – 3/19/20 AND GEOTECHNICAL SERVICES Binalonan, Pangasinan Lower Agno River Irrigation System NATIONAL IRRIGATION (0918) 8885-152 Ceferino C. Sta. Ana 4 Improvement Proj., Brgy. Tomana East, I 4/30/19 – 4/29/21 ADMINISTRATION (075) 633-3887 Rommeljon M. Leonen Rosales, Pangasinan 5 NORTHERN CEMENT CORPORATION Labayug, Sison, Pangasinan I (0917) 5764-091 Vincent F. Cabanilla 7/3/19 – 7/2/21 PROVINCIAL ENGINEERING OFFICE Malong Bldg., Capitol Compound, Lingayen, 542-6406 / 6 I Antonieta C. Delos Santos 11/23/17 – 11/22/19 (LINGAYEN, PANGASINAN) Pangasinan 542-6468 Valdez Center, Brgy. 1 San Francisco, (077) 781-2942 7 VVH CONSTRUCTION CORPORATION I Francisco Wayne B. Butay 6/20/19 – 6/19/21 San Nicolas, Ilocos Norte (0966) 544-8491 ACCURATEMIX TESTING SERVICES, (0906) 4859-531 8 Brgy. Muñoz East, Roxas, Isabela II Juanita Pine-Ordanez 3/11/19 – 3/10/21 INC. (0956) 4078-310 Maharlika Highway, Brgy. Ipil, (02) 633-6098 9 EB TESTING CENTER INC. (ISABELA) II Elnardo P. Bolivar 2/14/18 – 2/13/20 Echague, Isabela (02) 636-8827 MASUDA LABORATORY AND (0917) 8250-896 10 Marana 1st, City of Ilagan, Isabela II Randy S. -

Ethnic and Religious Conflict in Southern Philippines: a Discourse on Self-Determination, Political Autonomy, and Conflict Resolution
Ethnic and Religious Conflict in Southern Philippines: A Discourse on Self-Determination, Political Autonomy, and Conflict Resolution Jamail A. Kamlian Professor of History at Mindanao State University- ILigan Institute of Technology (MSU-IIT), ILigan City, Philippines ABSTRACT Filipina kini menghadapi masalah serius terkait populasi mioniritas agama dan etnis. Bangsa Moro yang merupakan salah satu etnis minoritas telah lama berjuang untuk mendapatkan hak untuk self-determination. Perjuangan mereka dilancarkan dalam berbagai bentuk, mulai dari parlemen hingga perjuangan bersenjata dengan tuntutan otonomi politik atau negara Islam teroisah. Pemberontakan etnis ini telah mengakar dalam sejarah panjang penindasan sejak era kolonial. Jika pemberontakan yang kini masih berlangsung itu tidak segera teratasi, keamanan nasional Filipina dapat dipastikan terancam. Tulisan ini memaparkan latar belakang historis dan demografis gerakan pemisahan diri yang dilancarkan Bangsa Moro. Setelah memahami latar belakang konflik, mekanisme resolusi konflik lantas diajukan dalam tulisan ini. Kata-Kata Kunci: Bangsa Moro, latar belakang sejarah, ekonomi politik, resolusi konflik. The Philippines is now seriously confronted with problems related to their ethnic and religious minority populations. The Bangsamoro (Muslim Filipinos) people, one of these minority groups, have been struggling for their right to self-determination. Their struggle has taken several forms ranging from parliamentary to armed struggle with a major demand of a regional political autonomy or separate Islamic State. The Bangsamoro rebellion is a deep- rooted problem with strong historical underpinnings that can be traced as far back as the colonial era. It has persisted up to the present and may continue to persist as well as threaten the national security of the Republic of the Philippines unless appropriate solutions can be put in place and accepted by the various stakeholders of peace and development. -
Nd Drrm C Upd Date
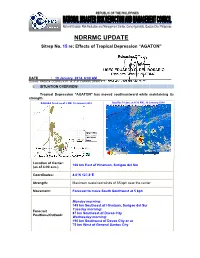
NDRRMC UPDATE Sitrep No. 15 re: Effects of Tropical Depression “AGATON” Releasing Officer: USEC EDUARDO D. DEL ROSARIO Executive Director, NDRRMC DATE : 19 January 2014, 6:00 AM Sources: PAGASA, OCDRCs V,VII, IX, X, XI, CARAGA, DPWH, PCG, MIAA, AFP, PRC, DOH and DSWD I. SITUATION OVERVIEW: Tropical Depression "AGATON" has moved southeastward while maintaining its strength. PAGASA Track as of 2 AM, 19 January 2014 Satellite Picture at 4:32 AM., 19 January 2014 Location of Center: 166 km East of Hinatuan, Surigao del Sur (as of 4:00 a.m.) Coordinates: 8.0°N 127.8°E Strength: Maximum sustained winds of 55 kph near the center Movement: Forecast to move South Southwest at 5 kph Monday morninng: 145 km Southeast of Hinatuan, Surigao del Sur Tuesday morninng: Forecast 87 km Southeast of Davao City Positions/Outlook: Wednesday morning: 190 km Southwest of Davao City or at 75 km West of General Santos City Areas Having Public Storm Warning Signal PSWS # Mindanao Signal No. 1 Surigao del Norte (30-60 kph winds may be expected in at Siargao Is. least 36 hours) Surigao del Sur Dinagat Province Agusan del Norte Agusan del Sur Davao Oriental Compostela Valley Estimated rainfall amount is from 5 - 15 mm per hour (moderate - heavy) within the 300 km diameter of the Tropical Depression Tropical Depression "AGATON" will bring moderate to occasionally heavy rains and thunderstorms over Visayas Sea travel is risky over the seaboards of Luzon and Visayas. The public and the disaster risk reduction and management councils concerned are advised to take appropriate actions II. -
R E G I O N Xi
Republic of the Philippines National Statistics Office R REPORT NO. 1-N E 2010 CENSUS G OF POPULATION I AND HOUSING POPULATION BY PROVINCE O CITY/MUNICIPALITY BARANGAY N DAVAO REGION XI CITATION: National Statistics Office, 2010 Census of Population and Housing Report No. 1-N REGION XI – DAVAO REGION Population by Province, City/Municipality, and Barangay April 2012 ISSN 0117-1453 2010 Census of Population and Housing Report No. 1 – N Population by Province, City/Municipality, and Barangay REGION XI DAVAO REGION REPUBLIC OF THE PHILIPPINES HIS EXCELLENCY PRESIDENT BENIGNO S. AQUINO III NATIONAL STATISTICAL COORDINATION BOARD Honorable Cayetano W. Paderanga Jr. Chairperson NATIONAL STATISTICS OFFICE Carmelita N. Ericta Administrator Paula Monina G. Collado Deputy Administrator Socorro D. Abejo Director III, Household Statistics Department ISSN 0117-1453 FOREWORD The 2010 Census of Population and Housing (2010 CPH) Report No. 1 is one of several publications designed to disseminate the results of the 2010 CPH. This report presents the population by province, city or municipality and barangay based on the 2010 CPH. This information will be useful for the formulation of the social and economic development policies, plans and programs of the Government. These are also important for purposes of the calculation of Internal Revenue Allocation, determination of number of congressional districts, and creation or conversion of various administrative geographic units. The 2010 CPH is the 13th census of population and the 6th census of housing that was conducted in the country since the first census undertaken in 1903. It was designed to take an inventory of the total population and housing units in the country and collect information about their characteristics as of the reference period May 1, 2010. -

First Quarter of 2019
TABLE OF CONTENTS I. Macroeconomic Performance . 1 Inflation . 1 Consumer Price Index . 1 Purchasing Power of Peso . 2 Labor and Employment . 2 II. Agriculture, Forestry and Fishery Sector Performance . 3 Crops . 3 Palay . 3 Corn . 3 Fruit Crops . 4 Vegetables . 4 Non-food and Industrial and Commercial Crops . 5 Livestock and Poultry . 5 Fishery . 6 Forestry . 6 III. Trade and Industry Services Sector Performance . 8 Business Name Registration . 8 Export . 8 Import . 9 Manufacturing . 9 Mining . 10 IV. Services Sector Performance . 11 Financing . 11 Tourism . 12 Air Transport . 12 Sea Transport . 13 Land Transport . 13 V. Peace and Security . 15 VI. Development Prospects . 16 MACROECONOMIC PERFORMANCE Inflation Rate Figure 1. Inflation Rate, Caraga Region The region’s inflation rate continued to move at a slower pace in Q1 2019. From 4.2 percent in December 2018, it declined by 0.5 percentage point in January 2019 at 3.7 percent (Figure 1) . It further decelerated in the succeeding months, registering 3.3 percent in February and 2.9 percent in March. This improvement was primarily due to the slow movement in the monthly increment in the price Source: PSA Caraga indices of heavily-weighted commodity groups, such as food and non-alcoholic beverages; Figure 2. Inflation Rate by Province housing, water, electricity, gas and other fuels; and transport. The importation of rice somehow averted the further increase in the market price of rice in the locality. In addition, the provision of government subsidies particularly to vulnerable groups (i.e. DOTr’s Pantawid Pasada Program) and free tuitions under Republic Act No. -

Counter Terrorist Trends and Analyses
Counter Terrorist Trends and Analyses www.rsis.edu.sg ISSN 2382-6444 | Volume 10, Issue 9 | September 2018 A JOURNAL OF THE INTERNATIONAL CENTRE FOR POLITICAL VIOLENCE AND TERRORISM RESEARCH (CTR) The Lamitan Bombing and Terrorist Threat in the Philippines Rommel C. Banlaoi Crime-Terror Nexus in Southeast Asia Bilveer Singh India and the Crime-Terrorism Nexus Ramesh Balakrishnan Crime -Terror Nexus in Pakistan Farhan Zahid Counter Terrorist Trends and Analyses Volume 9, Issue 4 | April 2017 1 Building a Global Network for Security Editorial Note Terrorist Threat in the Philippines and the Crime-Terror Nexus In light of the recent Lamitan bombing in the detailing the Siege of Marawi. The Lamitan Southern Philippines in July 2018, this issue bombing symbolises the continued ideological highlights the changing terrorist threat in the and physical threat of IS to the Philippines, Philippines. This issue then focuses, on the despite the group’s physical defeat in Marawi crime-terror nexus as a key factor facilitating in 2017. The author contends that the counter- and promoting financial sources for terrorist terrorism bodies can defeat IS only through groups, while observing case studies in accepting the group’s presence and hold in the Southeast Asia (Philippines) and South Asia southern region of the country. (India and Pakistan). The symbiotic Wrelationship and cooperation between terrorist Bilveer Singh broadly observes the nature groups and criminal organisations is critical to of the crime-terror nexus in Southeast Asia, the existence and functioning of the former, and analyses the Abu Sayyaf Group’s (ASG) despite different ideological goals and sources of finance in the Philippines. -

Typhoon Bopha (Pablo)
N MA019v2 ' N 0 ' Silago 3 0 ° 3 0 ° 1 0 Philippines 1 Totally Damaged Houses Partially Damaged Houses Number of houses Number of houses Sogod Loreto Loreto 1-25 2-100 717 376 Loreto Loreto 26-250 101-500 San Juan San Juan 251-1000 501-1000 1001-2000 1001-2000 2001-4000 2001-4000 Cagdianao Cagdianao 1 N ° N San Isidro 0 ° Dinagat 1 0 Dinagat San Isidro Philippines: 1 5 Dinagat (Surigao del Norte) Dinagat (Surigao 5 del Norte) Numancia 280 Typhoon Bopha Numancia Pilar Pilar Pilar Pilar (Pablo) - General 547 Surigao Dapa Surigao Dapa Luna General Totally and Partially Surigao Surigao Luna San San City Francisco City Francisco Dapa Dapa Damaged Housing in 1 208 3 4 6 6 Placer Placer Caraga Placer Placer 10 21 Bacuag Mainit Bacuag (as at 9th Dec 5am) Mainit Mainit 2 N 1 Mainit ' N 0 ' 3 0 ° Map shows totally and partially damaged 3 9 Claver ° 9 Claver housing in Davao region as of 9th Dec. 33 Bohol Sea Kitcharao Source is "NDRRMC sitrep, Effects of Bohol Sea Kitcharao 10 Typhoon "Pablo" (Bopha) 9th Dec 5am". 3 Province Madrid Storm track Madrid Region Lanuza Tubay Cortes ! Tubay Carmen Major settlements Carmen Cortes 513 2 127 21 Lanuza 10 Remedios T. Tandag Tandag City Tandag Remedios T. Tandag City Romualdez 3 Romualdez 15 N ° N 13 9 ° Bayabas 9 Buenavista Sibagat Buenavista Sibagat Bayabas Carmen Carmen Butuan 53 200 Butuan 127 Butuan 21 Butuan 3 City City Cagwait Cagwait 254 Prosperidad 12 17 Gingoog Buenavista 631 Gingoog Buenavista Marihatag Marihatag 43 1 38 19 San Las Nieves San Agustin Las Nieves Agustin 57 Prosperidad 56 2 4 0 10 -

Assessment of Impediments to Urban-Rural Connectivity in Cdi Cities
ASSESSMENT OF IMPEDIMENTS TO URBAN-RURAL CONNECTIVITY IN CDI CITIES Strengthening Urban Resilience for Growth with Equity (SURGE) Project CONTRACT NO. AID-492-H-15-00001 JANUARY 27, 2017 This report is made possible by the support of the American people through the United States Agency for International Development (USAID). The contents of this report are the sole responsibility of the International City/County Management Association (ICMA) and do not necessarily reflect the view of USAID or the United States Agency for International Development USAID Strengthening Urban Resilience for Growth with Equity (SURGE) Project Page i Pre-Feasibility Study for the Upgrading of the Tagbilaran City Slaughterhouse ASSESSMENT OF IMPEDIMENTS TO URBAN-RURAL CONNECTIVITY IN CDI CITIES Strengthening Urban Resilience for Growth with Equity (SURGE) Project CONTRACT NO. AID-492-H-15-00001 Program Title: USAID/SURGE Sponsoring USAID Office: USAID/Philippines Contract Number: AID-492-H-15-00001 Contractor: International City/County Management Association (ICMA) Date of Publication: January 27, 2017 USAID Strengthening Urban Resilience for Growth with Equity (SURGE) Project Page ii Assessment of Impediments to Urban-Rural Connectivity in CDI Cities Contents I. Executive Summary 1 II. Introduction 7 II. Methodology 9 A. Research Methods 9 B. Diagnostic Tool to Assess Urban-Rural Connectivity 9 III. City Assessments and Recommendations 14 A. Batangas City 14 B. Puerto Princesa City 26 C. Iloilo City 40 D. Tagbilaran City 50 E. Cagayan de Oro City 66 F. Zamboanga City 79 Tables Table 1. Schedule of Assessments Conducted in CDI Cities 9 Table 2. Cargo Throughput at the Batangas Seaport, in metric tons (2015 data) 15 Table 3. -

Indigenous Religion, Institutions and Rituals of the Mamanwas of Caraga Region, Philippines
Asian Journal of Social Sciences, Arts and Humanities Vol. 1, No.1, 2013 INDIGENOUS RELIGION, INSTITUTIONS AND RITUALS OF THE MAMANWAS OF CARAGA REGION, PHILIPPINES Ramel D. Tomaquin College of Arts and Sciences Surigao del Sur State University Tandag City, Philippines Email: [email protected] ABSTRACT The Mamanwas, one of the IP communities of Caraga region. Said to be one of the original settlers of Caraga and considered the Negrito group of Mindanao. Only very few literatures and studies written about them. Despite of massive acculturation of other IP groups of the region such the Agusan-Surigao Manobos, the Mansaka/Mandaya, Banwaon, Higaanon and Talaandig. The Mamanwas still on the process of integration to Philippine body-politic. It is in this scenario they were able to retain indigenous religion, institutions and rituals. Thus the study was conducted. It covers on the following sites: Mt. Manganlo in Claver, Lake Mainit in Alegria both Surigao Del Norte, Hitaob in Tandag City, Lubcon and Burgus in Cortes and Sibahay in Lanuza of Surigao Del Sur respectively. The study used ethnographic method with strict adherence of the right of pre- informed consent in accordance with RA 8371 or Indigenous Peoples Right Act of 1997. It can be deduced from the paper that despite of socio- cultural changes of the IP’s of Caraga the Mamanwas were able to retain these practices but for how long? Moreover, socio-cultural change is slowly taking place in the Mamanwa social milieu. Preservation of these worldviews is wanting as a part of national heritage and for posterity. -

Resettlement and Indigenous Peoples Plan PHI: Improving Growth Corridors in Mindanao Road Sector Project
Resettlement and Indigenous Peoples Plan Document stage: Draft August 2017 Project number: 41076-048 PHI: Improving Growth Corridors in Mindanao Road Sector Project PR07: Tampilisan-Sandayong Road Prepared by the Department of Public Works and Highways for the Asian Development Bank. Currency Equivalents (as of 21 July 2017) Currency unit – peso (P) P1.00 = $0.02 $1.00 = P50.75 Abbreviations AD – Ancestral Domain ADB – Asian Development Bank AH – Affected Households AP – Affected Persons BIR – Bureau of Internal Revenue CADC – Certificate of Ancestral Domain Claim CADT – Certificate of Ancestral Domain Title CCA – Community Consultative Assembly CALT – Community of Ancestral Land Title CLOA – Certificate of Land Ownership Award CAP – Corrective Action Plan COI – Corridor of Impact DEO – District Engineering Office DPWH – Department of Public Works and Highways DMS – Detailed Measurement Survey DDR – Due Diligence Report EA – Executing Agency EMA – External Monitoring – Agent EO – Executive Order ESSD – Environment and Social Safeguards Division FPIC – Free and Prior Informed Consent GOP – Government of the Philippines GRM – Grievance Redress Mechanism IGCMRSP – Improving Growth Corridors in Mindanao Road Sector Project IMA Internal Monitoring Agent IOL – Inventory of Loss IP/ICC – Indigenous Peoples/ Indigenous Cultural Communities IPP – Indigenous Peoples Plan IPRA – Indigenous Peoples Rights Act LA – Land Acquisition LARRIPP – Land Acquisition, Resettlement, Rehabilitation and Indigenous Peoples Policy (DPWH 2007) LGU – Local Government -

Counter-Insurgency Vs. Counter-Terrorism in Mindanao
THE PHILIPPINES: COUNTER-INSURGENCY VS. COUNTER-TERRORISM IN MINDANAO Asia Report N°152 – 14 May 2008 TABLE OF CONTENTS EXECUTIVE SUMMARY AND RECOMMENDATIONS................................................. i I. INTRODUCTION .......................................................................................................... 1 II. ISLANDS, FACTIONS AND ALLIANCES ................................................................ 3 III. AHJAG: A MECHANISM THAT WORKED .......................................................... 10 IV. BALIKATAN AND OPLAN ULTIMATUM............................................................. 12 A. EARLY SUCCESSES..............................................................................................................12 B. BREAKDOWN ......................................................................................................................14 C. THE APRIL WAR .................................................................................................................15 V. COLLUSION AND COOPERATION ....................................................................... 16 A. THE AL-BARKA INCIDENT: JUNE 2007................................................................................17 B. THE IPIL INCIDENT: FEBRUARY 2008 ..................................................................................18 C. THE MANY DEATHS OF DULMATIN......................................................................................18 D. THE GEOGRAPHICAL REACH OF TERRORISM IN MINDANAO ................................................19