The Role of Mechanical Resonance in Physiological Tremor
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Dynamic Manipulation of Mechanical Resonators in the High Amplitude Regime Through Optical Backaction
Dynamic manipulation of mechanical resonators in the high amplitude regime through optical backaction Mahmood Bagheri, Menno Poot, Mo Li, Wolfram P. H. Pernice, Hong X. Tang Department of Electrical Engineering, Yale University, New Haven, CT 06511 Cavity optomechanics enables active manipulation of mechanical resonators through backaction cooling and amplification1,2. This ability to control mechanical motion with retarded optical forces has recently spurred a race towards realizing a mechanical resonator in its quantum ground state3,4,5,6,7,8,9. Here, instead of quenching optomechanical motion, we demonstrate high amplitude operation of nanomechanical resonators by utilizing a highly efficient phonon generation process. In this regime, the nanomechanical resonators gain sufficient energy from the optical field to overcome the large energy barrier of a double well potential, leading to nanomechanical slow-down and zero frequency singularity, as predicted by early theories10. Besides fundamental studies and interests in parametric amplification of small forces11, optomechanical backaction is also projected to open new windows for studying discrete mechanical states12,13 and to foster applications14,15,16,17. Here we realize a non-volatile mechanical memory element, in which bits are written and reset via optomechanical backaction by controlling the mechanical damping across the barrier. Our study casts a new perspective on the energy dynamics in coupled mechanical resonator – cavity systems and enables novel functional devices that utilize the principles of cavity optomechanics. Classical and quantum dynamics of nanomechanical systems promise new applications in nanotechnology18,19 and fundamental tests of quantum mechanics in mesoscopic objects2,9. Recent development of nanoscale electromechanical (NEMS) and optomechanical systems has enabled cooling of mechanical systems to their quantum ground state7,8, which brings the possibility of quantum information processing with mechanical devices20,21. -
Tuning the Resonant Frequency and Damping of an Electromagnetic Energy Harvester Using Power Electronics Paul D
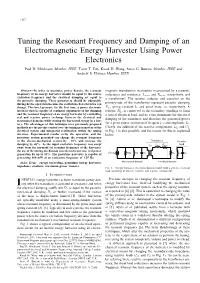
Tuning the Resonant Frequency and Damping of an Electromagnetic Energy Harvester Using Power Electronics Paul D. Mitcheson Member, IEEE, Tzern T. Toh, Kwok H. Wong, Steve G. Burrow Member, IEEE and Andrew S. Holmes Member, IEEE Abstract—In order to maximize power density, the resonant magnetic transduction mechanism (represented by a parasitic frequency of an energy harvester should be equal to the source inductance and resistance, Larm and Rarm, respectively, and excitation frequency and the electrical damping set equal to a transformer). The resistor, inductor and capacitor on the the parasitic damping. These parameters should be adjustable during device operation because the excitation characteristics can primary-side of the transformer represent parasitic damping change. This brief presents, for the first time, a power electronic Dp, spring constant k, and proof mass, m, respectively. A interface that is capable of continual adjustment of the damping resistor, RL, is connected to the secondary windings to form and the resonant frequency of an energy harvester by controlling a typical electrical load, and its value determines the electrical real and reactive power exchange between the electrical and damping of the transducer and therefore the generated power mechanical domains while storing the harvested energy in a bat- tery. The advantages of this technique over previously proposed for a given source excitation of frequency ω and amplitude Y0. methods are the precise control over the tuning parameters of the Clearly, the addition of the reactive components, LL and CL electrical system and integrated rectification within the tuning in Fig. 1 is also possible, and the reason for this is explained interface. -

In April 1831, a Brigade of Soldiers Marched in Step Across England's Broughton Suspension Bridge
In April 1831, a brigade of soldiers marched in step across England's Broughton Suspension Bridge. According to accounts of the time, the bridge broke apart beneath the soldiers, throwing dozens of men into the water. After this happened, the British Army reportedly sent new orders: Soldiers crossing a long bridge must "break stride," or not march in unison, to stop such a situation from occurring again. Structures like bridges and buildings, although they appear to be solid and immovable, have a natural frequency of vibration within them. A force that's applied to an object at the same frequency as the object's natural frequency will amplify the vibration of the object in an occurrence called mechanical resonance. Sometimes your car shakes hard when you hit a certain speed, and a girl on a swing can go higher with little effort just by swinging her legs. The same principle of mechanical resonance that makes these incidents happen also works when people walk in lockstep across a bridge. If soldiers march in unison across the structure, they apply a force at the frequency of their step. If their frequency is closely matched to the bridge's frequency, the soldiers' rhythmic marching will amplify the vibrational frequency of the bridge. If the mechanical resonance is strong enough, the bridge can vibrate until it collapses from the movement. A potent reminder of this was seen in June 2000, when London's Millennium Bridge opened to great fanfare. As crowds packed the bridge, their footfalls made the bridge vibrate slightly. "Many pedestrians fell spontaneously into step with the bridge's vibrations, inadvertently amplifying them," according to a 2005 report in Nature. -

Mechanical Stabilisation of Superconducting Quarter Wave Resonators A
MECHANICAL STABILISATION OF SUPERCONDUCTING QUARTER WAVE RESONATORS A. Facco, INFN- Laboratori Nazionali di Legnaro, via Romea 4, 35020 Legnaro (Padova) Italy; V. Zviagintsev, ITEP, B. Cheremushkinskaya 25, Moscow,117259, Russia. Abstract in the case of white noise; on the other hand, when a 42 Hz mechanical vibration is applied for a long enough A device which is capable to reduce significantly the time, the frequency error can reach such an amplitude amplitude of mechanical vibrations in superconducting that the phase-lock system capabilities are exceeded. In quarter wave resonators was designed, constructed and the ALPI linac cryostats this condition can appear, for a tested. This device can eliminate the necessity of fast few minutes, almost everyday; this could make the tuners and related electronics in many superconducting operation of many resonators at the same time cavities, resulting in a significant cost saving both in the problematic. We have exploited a new approach to this construction and in the operation of superconducting low problem: we have added to the resonator a mechanical beta linacs. dissipator, capable to absorb energy from the dangerous mechanical mode and, consequently, to reduce its 1 INTRODUCTION amplitude. One problem in this approach is the difficulty Mechanical stability is a very important requirement in of building a device with a linear, or at least smooth, superconducting cavities; their very small rf bandwidth, a response at liquid helium temperature; another problem is consequence of their very high quality factor, makes very that new resonant modes could be easily introduced by difficult to lock them to an external frequency, requiring adding to the resonator new parts. -

Tuning of a Vibration Absorber with Shunted Piezoelectric Transducers
Arch Appl Mech (2016) 86:1715–1732 DOI 10.1007/s00419-014-0972-5 SPECIAL Oliver Heuss · Rogério Salloum · Dirk Mayer · Tobias Melz Tuning of a vibration absorber with shunted piezoelectric transducers Received: 16 December 2013 / Accepted: 19 November 2014 / Published online: 13 December 2014 © The Author(s) 2014. This article is published with open access at Springerlink.com Abstract In order to reduce structural vibrations in narrow frequency bands, tuned mass absorbers can be an appropriate measure. A quite similar approach which makes use of applied piezoelectric elements, instead of additional oscillating masses, are the well-known resonant shunts, consisting of resistances, inductances, and possibly negative capacitances connected to the piezoelectric element. This paper presents a combined approach, which is based on a conventional tuned mass absorber, but whose characteristics can be strongly influenced by applying shunted piezoceramics. Simulations and experimental analyses are shown to be very effective in predicting the behavior of such electromechanical systems. The vibration level of the absorber can be strongly attenuated by applying different combinations of resistant, resonant, and negative capacitance shunt circuits. The damping characteristics of the absorber can be changed by applying a purely resistive or resonant resistant shunt. Additionally, the tuning frequency of the absorber can be adapted to the excitation frequency, using a negative capacitance shunt circuit, which requires only the energy to supply the electric components. Keywords Shunt damping · Tuned mass absorber · Active vibration control · Semi-active · Frequency tuning 1 Introduction Tuned vibration absorbers [1] are common means of vibration reduction in many technical applications. Basically, those devices are single degree of freedom oscillators comprising of a spring-damper element and of an inertial mass. -

Frequency Tuning of Vibration Absorber Using Topology
FREQUENCY TUNING OF VIBRATION ABSORBER USING TOPOLOGY OPTIMIZATION by SWAPNIL SUBHASH HAREL Presented to the Faculty of the Graduate School of The University of Texas at Arlington in Partial Fulfillment of the Requirements for the Degree of MASTER OF SCIENCE IN MECHANICAL ENGINEERING THE UNIVERSITY OF TEXAS AT ARLINGTON Copyright © by Swapnil Subhash Harel 2017 All Rights Reserved 2 Acknowledgements I would like to express my gratitude towards Dr. Robert Taylor for guiding and helping me throughout my thesis research. He always had time to discuss my work and helped solve any problem that I faced during my research work. I would like to thank Dr. Bo Wang for constantly supporting my research work with his ideas which were second to none. I would also like to thank Dr, Kent Lawrence for finding time out of their busy schedule to serve on my thesis defense committee. Lastly, I would like to thank my family. I would especially like to support my father, Subhash Harel, my mother Surekha Harel and my younger sister Apurva Harel for their support all these years. It was their continued support and belief that I have been able to do all that I have done so far. I would also like to offer regards to all those who have supported or helped me in any regards this period. May 04, 2017 3 Abstract FREQUENCY TUNING OF VIBRATION ABSORBER USING TOPOLOGY OPTIMIZATION by Swapnil Subhash Harel, MS The University of Texas at Arlington, 2017 Supervising Professors: Dr. Robert Taylor and Dr. Bo Wang A tuned mass absorber is a system for reducing the amplitude in one oscillator by coupling it to a second oscillator. -
Modulation of Mechanical Resonance by Chemical Potential Oscillation in Graphene
LETTERS PUBLISHED ONLINE: 7 DECEMBER 2015 | DOI: 10.1038/NPHYS3576 Modulation of mechanical resonance by chemical potential oscillation in graphene Changyao Chen1†, Vikram V. Deshpande2, Mikito Koshino3, Sunwoo Lee4, Alexander Gondarenko1, Allan H. MacDonald5, Philip Kim6 and James Hone1* The classical picture of the force on a capacitor assumes a investigated. Understanding the corrections to the classical model large density of electronic states, such that the electrochemical is of fundamental interest and important for modelling of nano- potential of charges added to the capacitor is given by mechanical systems in the atomically thin limit3,4. Here we examine the external electrostatic potential and the capacitance is the case of a resonant nano-mechanical device, and show that the determined purely by geometry1. Here we consider capacitively first-order correction to the resonant frequency consists of three driven motion of a nano-mechanical resonator with a low terms: one term proportional to µ and the other two proportional density of states, in which these assumptions can break to its derivative dµ/dn, with the latter represented through the in- 2–5 −1 D. = 2/. µ/ down . We find three leading-order corrections to the verse quantum capacitance CQ 1 Ae d dn)(A is the sample classical picture: the first of which is a modulation in the size and e is the electron charge). The phenomenon is explored static force due to variation in the internal chemical potential; experimentally by examining the behaviour of a graphene resonator, the second and third are changes in the static force and in which µ is tuned by a perpendicular magnetic field B at a dynamic spring constant due to the rate of change of chemical fixed electrochemical potential. -

Chapter 3 Theory of Phase Noise Mechanism of NEMS
Chapter 3 Theory of Phase Noise Mechanism of NEMS We present the theory of phase noise mechanism of NEMS. We examine both fundamental and nonfundamental noise processes to obtain expressons for phase noise density, Allan deviation, and mass sensitivity. Fundamental noise processes considered here include thermomechanical noise, momentum exchange noise, adsorption-desorption noise, diffusion noise, and temperature fluctuation noise. For nonfundamental noise processes, we develop a formalism to consider the Nyquist- Johnson noise from transducer amplifier implementations. The detailed analysis here not only reveals the achievable frequency stability of NEMS devices, but also provides a theoretical framework to fully optimize noise performance and the mass sensitivity for sensing applications. 29 3.1 Introduction So far we have considered how physical fluctuations convert into the noise sidebands of the carrier and give the conventional definition of phase noise, frequency noise, and Allan deviation, all commonly used to characterize the frequency stability of an oscillator. Here we proceed to investigate phase noise mechanisms affecting NEMS devices. First, we examine the fundamental noise processes intrinsic to NEMS devices.1-3 We begin our discussion from thermomechanical noise, originating from thermally driven random motion of the resonator, by considering the thermal fluctuating force acting on the resonator. We then consider momentum exchange noise, adsorption- desorption noise, and diffusion noise, all arising from gaseous molecules in resonator surroundings. The impinging gaseous molecules can impart momentum randomly to a NEMS device and induce momentum exchange noise. Moreover, when gaseous species adsorb on a NEMS device, typically from the surrounding environment, they can diffuse along the surface in and out of the device and produce diffusion noise. -

M 17E “Pohl's Wheel (Linear and Nonlinear Oscillations)”
Fakultät für Physik und Geowissenschaften Physikalisches Grundpraktikum M 17e “Pohl’s wheel (linear and nonlinear oscillations)” Tasks 1. Determine the frequency fd, the damping constant and the logarithmic decrement of the rotating pendulum after Pohl at eight different attenuations (currents IW of the eddy current brake). Plot the logarithmic decrement as a function of the square of the current IW and determine the straight line parameters via linear regression. 2. Experimentally, determine the directional torque D and the moment of inertia J of the rotating pendulum. 3. Record the resonance curve of the rotating pendulum at one of the given attenuations. Determine the resonance frequency and the damping constant and compare the values to those obtained in task 1. 4. Experimentally, try to observe for the nonlinear pendulum the first bifurcation and (qualitatively) the transition to chaotic motion. To this end measure the amplitudes close to the resonance of the forced oscillation for various values of the eddy current brake current IW (to be decreased in small steps) and plot them graphically. Additional task For the driven pendulum, simulate the first bifurcation and the transition to chaotic oscillations by changing the attenuation. A computer algebra program is available for download in the download area of the Undergraduate Physics Lab website. Literature Physics, M. Alonso, E. F. Finn, Chap. 10.10 The Physics of Vibrations and Waves, H. J. Pain, Wiley 1968, Chap. 3 Physikalisches Praktikum, 13. Auflage, Hrsg. W. Schenk, F. Kremer, -

Lesson 45: Resonance
Lesson 45: Resonance If we look at examples of SHM we may find that we can come up with some interesting effects. Imagine pushing a child on a swing. How do you make her go higher? ● Well, you make sure that you time your pushes so that you push in sync with the way she is already swinging. ● If you push randomly (out of sync), then the child will never go very high. ● This causes the simple harmonic motion of the child to have an increasing amplitude. We give this kind of "in sync" motion the special name "resonance." Resonant Frequency & Forced Frequency From the last lesson you learned that the only thing that changes the period of a pendulum is its length. ● Even if we change other things, like the mass on the end of the pendulum, the period will stay the same. ● Every pendulum that has the same length has the same period, and also the same frequency. ● This particular frequency is the natural frequency that the pendulum will always swing at. ● This particular frequency is the resonant frequency of the pendulum. This is like the example of the swinging child above. ● The important thing is that if you just walk away from the child on the swing, eventually the swing will stop. ● This is because over time friction will cause energy to be drained out of the system until it stops. ● In order to keep the child swinging, you must continue to push her at the natural resonant frequency of the swing. ● By doing this you are constantly adding energy back in to the swing to replace the energy that was lost due to friction. -

Going Into Resonance
thesis Going into resonance The notion of ‘resonance’ is among the most of the two frequencies, concluding that the to realize wireless communications. But familiar ideas in science. Two pendulum amplitude of the oscillation would increase all of this, it turns out, took place before clocks in resonance synchronize themselves, linearly in time, and potentially without bound. engineers really began appreciating the role sound waves of the right frequency drive One might expect this breakthrough in of resonance in more tangible mechanical strong vibrations in a drum, and photons mechanics to have propelled the resonance systems. The gradual acceptance of tuned to atomic transitions put atoms into phenomenon into the centre of physics and resonance as a mechanical phenomenon only excited states. Particle physicists often detect engineering, and yet it didn’t. Perhaps, as Bleck- took place as dramatic failures in bridges and new particles through the appearance of Neuhaus notes, that’s because Euler himself machines made engineers painfully aware of resonances in scattering data. And we all, only considered the problem as a mathematical the inadequacy of the static analysis of forces, of course, rely on resonance in our use of curiosity lacking any practical import. Euler’s and the need to consider the surprising wireless communications. results were then ignored for well over a century, effects of interactions at similar frequencies. In 1965, in his famous Lectures on Physics, until derived again independently in the Working mostly from original sources in Richard Feynman suggested that the resonance nineteenth century by Thomas Young. Oddly, Germany, Bleck-Neuhaus readily admits that concept had become so influential that every however, Young only considered the problem in his history of the resonance concept is weighted new volume of the Physical Review would connection with the analysis of tides, and so his towards German scientists. -

International Journal of Acoustics and Vibration, Vol
EDITORIAL OFFICE International Journal of EDITOR-IN-CHIEF Acoustics and Vibration Malcolm J. Crocker A quarterly publication of the International Institute of Acoustics and Vibration MANAGING EDITOR Marek Pawelczyk ASSOCIATE EDITORS Dariusz Bismor Volume 22, Number 2, June 2017 Nickolay Ivanov Zhuang Li ASSISTANT EDITORS Teresa Glowka EDITORIAL Sebastian Kurczyk ICSV24: London Calling Karol Jablonski Jian Kang and Barry Gibbs ....................... 142 Jan Wegehaupt EDITORIAL ASSISTANT ARTICLES Neha Patel Modeling and Vibration Suppression of Flexible Spacecraft Using Higher-Order Margarita Maksotskaya Sandwich Panel Theory Milad Azimi, Morteza Shahravi and Keramat Malekzadeh Fard ....... 143 Free Vibration Analysis of Functionally Heterogeneous Hollow Cylinder Based on Three Dimensional Elasticity Theory Masoud Asgari ............................. 151 EDITORIAL BOARD Electrically Forced Vibrations of Partially Electroded Rectangular Quartz Plate Piezoelectric Resonators Jorge P. Arenas Hui Chen, Ji Wang, Jianke Du and Jiashi Yang ............... 161 Valdivia, Chile Damping Performance of Dynamic Vibration Absorber in Nonlinear Simple Beam with 1:3 Internal Resonance Jonathan D. Blotter Yi-Ren Wang and Hsueh-Ghi Lu ..................... 167 Provo, USA Energy Harvesting Estimation from the Vibration of a Simply Supported Beam Leonid Gelman A. Rajora, A. Dwivedi, A. Vyas, S. Gupta and A. Tyagi ........... 186 Cranfield, UK Preparation and Experimental Study of Magnetorheological Fluids for Vibration Control Samir Gerges Ying-Qing Guo, Zhao-Dong Xu, Bing-Bing Chen, Cheng-Song Ran Florianopolis,´ Brazil and Wei-Yang Guo ........................... 194 Colin H. Hansen A Subjective Related Measure of Airborne Sound Insulation Adelaide, Australia Reinhard O. Neubauer and Jian Kang ................... 201 Mechanical Fault Diagnosis Method Based on LMD Shannon Entropy and Hugh Hunt Improved Fuzzy C-means Clustering Cambridge, England Shaojiang Dong, Xiangyang Xu and Jiayuan Luo .............