Genetic Disorders Leading to Hypoglycaemia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

• Glycolysis • Gluconeogenesis • Glycogen Synthesis
Carbohydrate Metabolism! Wichit Suthammarak – Department of Biochemistry, Faculty of Medicine Siriraj Hospital – Aug 1st and 4th, 2014! • Glycolysis • Gluconeogenesis • Glycogen synthesis • Glycogenolysis • Pentose phosphate pathway • Metabolism of other hexoses Carbohydrate Digestion! Digestive enzymes! Polysaccharides/complex carbohydrates Salivary glands Amylase Pancreas Oligosaccharides/dextrins Dextrinase Membrane-bound Microvilli Brush border Maltose Sucrose Lactose Maltase Sucrase Lactase ‘Disaccharidase’ 2 glucose 1 glucose 1 glucose 1 fructose 1 galactose Lactose Intolerance! Cause & Pathophysiology! Normal lactose digestion Lactose intolerance Lactose Lactose Lactose Glucose Small Intestine Lactase lactase X Galactose Bacteria 1 glucose Large Fermentation 1 galactose Intestine gases, organic acid, Normal stools osmotically Lactase deficiency! active molecules • Primary lactase deficiency: อาการ! genetic defect, การสราง lactase ลด ลงเมออายมากขน, พบมากทสด! ปวดทอง, ถายเหลว, คลนไสอาเจยนภาย • Secondary lactase deficiency: หลงจากรบประทานอาหารทม lactose acquired/transient เชน small bowel เปนปรมาณมาก เชนนม! injury, gastroenteritis, inflammatory bowel disease! Absorption of Hexoses! Site: duodenum! Intestinal lumen Enterocytes Membrane Transporter! Blood SGLT1: sodium-glucose transporter Na+" Na+" •! Presents at the apical membrane ! of enterocytes! SGLT1 Glucose" Glucose" •! Co-transports Na+ and glucose/! Galactose" Galactose" galactose! GLUT2 Fructose" Fructose" GLUT5 GLUT5 •! Transports fructose from the ! intestinal lumen into enterocytes! -

Hereditary Galactokinase Deficiency J
Arch Dis Child: first published as 10.1136/adc.46.248.465 on 1 August 1971. Downloaded from Alrchives of Disease in Childhood, 1971, 46, 465. Hereditary Galactokinase Deficiency J. G. H. COOK, N. A. DON, and TREVOR P. MANN From the Royal Alexandra Hospital for Sick Children, Brighton, Sussex Cook, J. G. H., Don, N. A., and Mann, T. P. (1971). Archives of Disease in Childhood, 46, 465. Hereditary galactokinase deficiency. A baby with galactokinase deficiency, a recessive inborn error of galactose metabolism, is des- cribed. The case is exceptional in that there was no evidence of gypsy blood in the family concerned. The investigation of neonatal hyperbilirubinaemia led to the discovery of galactosuria. As noted by others, the paucity of presenting features makes early diagnosis difficult, and detection by biochemical screening seems desirable. Cataract formation, of early onset, appears to be the only severe persisting complication and may be due to the biosynthesis and accumulation of galactitol in the lens. Ophthalmic surgeons need to be aware of this enzyme defect, because with early diagnosis and dietary treatment these lens changes should be reversible. Galactokinase catalyses the conversion of galac- and galactose diabetes had been made in this tose to galactose-l-phosphate, the first of three patient (Fanconi, 1933). In adulthood he was steps in the pathway by which galactose is converted found to have glycosuria as well as galactosuria, and copyright. to glucose (Fig.). an unexpectedly high level of urinary galactitol was detected. He was of average intelligence, and his handicaps, apart from poor vision, appeared to be (1) Galactose Gackinase Galactose-I-phosphate due to neurofibromatosis. -

Early Modifications of Gene Expression Induced in Liver by Azo-Dye Diet
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector Volume 206, number 2 FEBS 4070 October 1986 Early modifications of gene expression induced in liver by azo-dye diet EugCnia Lamas, Fabien Schweighoffer and Axe1 Kahn Unit& de Recherches en GP&tique et Pathologie Mol&ulaires, INSERM U 129, CHU COCHIN, 24, Rue du Faubourg Saint Jacques, 75674 Paris Cedex 14, France Received 5 August 1986 The expression and regulation of the phosphoenolpyruvate carboxykinase gene were not grossly modified by feeding rats a 3’-methyl-4-(dimethylamino)azobenzene-containing diet despite maximum expression of the L-type pyruvate kinase gene being dramatically reduced as early as the 24th hour of the carcinogenic diet. Inhibition of aldolase B mRNA synthesis occurred more slowly, being maximum at the 3rd day. After stopping administration of the carcinogen, a very rapid, but transient increase of the L-type pyruvate kinase mRNA was observed at the 24th hour, whereas aldolase B mRNA increased only slowly. The amount of aldolase A mRNA fell quickly after termination of carcinogen administration, levels being normal at the 2nd-3rd day. At this time, the histological structure of the liver was indistinguishable from that of animals still receiving the azo-dye diet. It appears, therefore, that in the rat both administration and withdrawal of the azo-dye carcinogen induce rapid modifications of the expression of some genes, before any cellular modification is distinguishable. Azo-dye diet mRNA Hepatocarcinogenesis Phosphoenolpyruvate carboxykinase Aldolase Pyruvate kinase 1. INTRODUCTION some genes. Such a possibility is of theoretical im- portance because it could constitute the basis for The azo-dye 3’-methyl-4-(dimethylamino)azo- the carcinogenic action of the dye. -

A Computational Approach for Defining a Signature of Β-Cell Golgi Stress in Diabetes Mellitus
Page 1 of 781 Diabetes A Computational Approach for Defining a Signature of β-Cell Golgi Stress in Diabetes Mellitus Robert N. Bone1,6,7, Olufunmilola Oyebamiji2, Sayali Talware2, Sharmila Selvaraj2, Preethi Krishnan3,6, Farooq Syed1,6,7, Huanmei Wu2, Carmella Evans-Molina 1,3,4,5,6,7,8* Departments of 1Pediatrics, 3Medicine, 4Anatomy, Cell Biology & Physiology, 5Biochemistry & Molecular Biology, the 6Center for Diabetes & Metabolic Diseases, and the 7Herman B. Wells Center for Pediatric Research, Indiana University School of Medicine, Indianapolis, IN 46202; 2Department of BioHealth Informatics, Indiana University-Purdue University Indianapolis, Indianapolis, IN, 46202; 8Roudebush VA Medical Center, Indianapolis, IN 46202. *Corresponding Author(s): Carmella Evans-Molina, MD, PhD ([email protected]) Indiana University School of Medicine, 635 Barnhill Drive, MS 2031A, Indianapolis, IN 46202, Telephone: (317) 274-4145, Fax (317) 274-4107 Running Title: Golgi Stress Response in Diabetes Word Count: 4358 Number of Figures: 6 Keywords: Golgi apparatus stress, Islets, β cell, Type 1 diabetes, Type 2 diabetes 1 Diabetes Publish Ahead of Print, published online August 20, 2020 Diabetes Page 2 of 781 ABSTRACT The Golgi apparatus (GA) is an important site of insulin processing and granule maturation, but whether GA organelle dysfunction and GA stress are present in the diabetic β-cell has not been tested. We utilized an informatics-based approach to develop a transcriptional signature of β-cell GA stress using existing RNA sequencing and microarray datasets generated using human islets from donors with diabetes and islets where type 1(T1D) and type 2 diabetes (T2D) had been modeled ex vivo. To narrow our results to GA-specific genes, we applied a filter set of 1,030 genes accepted as GA associated. -

Repercussions of Inborn Errors of Immunity on Growth☆ Jornal De Pediatria, Vol
Jornal de Pediatria ISSN: 0021-7557 ISSN: 1678-4782 Sociedade Brasileira de Pediatria Goudouris, Ekaterini Simões; Segundo, Gesmar Rodrigues Silva; Poli, Cecilia Repercussions of inborn errors of immunity on growth☆ Jornal de Pediatria, vol. 95, no. 1, Suppl., 2019, pp. S49-S58 Sociedade Brasileira de Pediatria DOI: https://doi.org/10.1016/j.jped.2018.11.006 Available in: https://www.redalyc.org/articulo.oa?id=399759353007 How to cite Complete issue Scientific Information System Redalyc More information about this article Network of Scientific Journals from Latin America and the Caribbean, Spain and Journal's webpage in redalyc.org Portugal Project academic non-profit, developed under the open access initiative J Pediatr (Rio J). 2019;95(S1):S49---S58 www.jped.com.br REVIEW ARTICLE ଝ Repercussions of inborn errors of immunity on growth a,b,∗ c,d e Ekaterini Simões Goudouris , Gesmar Rodrigues Silva Segundo , Cecilia Poli a Universidade Federal do Rio de Janeiro (UFRJ), Faculdade de Medicina, Departamento de Pediatria, Rio de Janeiro, RJ, Brazil b Universidade Federal do Rio de Janeiro (UFRJ), Instituto de Puericultura e Pediatria Martagão Gesteira (IPPMG), Curso de Especializac¸ão em Alergia e Imunologia Clínica, Rio de Janeiro, RJ, Brazil c Universidade Federal de Uberlândia (UFU), Faculdade de Medicina, Departamento de Pediatria, Uberlândia, MG, Brazil d Universidade Federal de Uberlândia (UFU), Hospital das Clínicas, Programa de Residência Médica em Alergia e Imunologia Pediátrica, Uberlândia, MG, Brazil e Universidad del Desarrollo, -
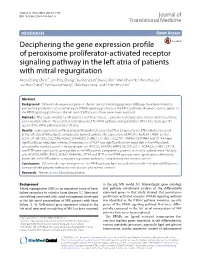
Deciphering the Gene Expression Profile of Peroxisome Proliferator
Chen et al. J Transl Med (2016) 14:157 DOI 10.1186/s12967-016-0871-3 Journal of Translational Medicine RESEARCH Open Access Deciphering the gene expression profile of peroxisome proliferator‑activated receptor signaling pathway in the left atria of patients with mitral regurgitation Mien‑Cheng Chen1*, Jen‑Ping Chang2, Yu‑Sheng Lin3, Kuo‑Li Pan3, Wan‑Chun Ho1, Wen‑Hao Liu1, Tzu‑Hao Chang4, Yao‑Kuang Huang5, Chih‑Yuan Fang1 and Chien‑Jen Chen1 Abstract Background: Differentially expressed genes in the left atria of mitral regurgitation (MR) pigs have been linked to peroxisome proliferator-activated receptor (PPAR) signaling pathway in the KEGG pathway. However, specific genes of the PPAR signaling pathway in the left atria of MR patients have never been explored. Methods: This study enrolled 15 MR patients with heart failure, 7 patients with aortic valve disease and heart failure, and 6 normal controls. We used PCR assay (84 genes) for PPAR pathway and quantitative RT-PCR to study specific genes of the PPAR pathway in the left atria. Results: Gene expression profiling analysis through PCR assay identified 23 genes to be differentially expressed in the left atria of MR patients compared to normal controls. The expressions of APOA1, ACADM, FABP3, ETFDH, ECH1, CPT1B, CPT2, SLC27A6, ACAA2, SMARCD3, SORBS1, EHHADH, SLC27A1, PPARGC1B, PPARA and CPT1A were significantly up-regulated, whereas the expression of PLTP was significantly down-regulated in the MR patients compared to normal controls. The expressions of HMGCS2, ACADM, FABP3, MLYCD, ECH1, ACAA2, EHHADH, CPT1A and PLTP were significantly up-regulated in the MR patients compared to patients with aortic valve disease. -

Biochemistry Entry of Fructose and Galactose
Paper : 04 Metabolism of carbohydrates Module : 06 Entry of Fructose and Galactose Dr. Vijaya Khader Dr. MC Varadaraj Principal Investigator Dr.S.K.Khare,Professor IIT Delhi. Paper Coordinator Dr. Ramesh Kothari,Professor UGC-CAS Department of Biosciences Saurashtra University, Rajkot-5, Gujarat-INDIA Dr. S. P. Singh, Professor Content Reviewer UGC-CAS Department of Biosciences Saurashtra University, Rajkot-5, Gujarat-INDIA Dr. Charmy Kothari, Assistant Professor Content Writer Department of Biotechnology Christ College, Affiliated to Saurashtra University, Rajkot-5, Gujarat-INDIA 1 Metabolism of Carbohydrates Biochemistry Entry of Fructose and Galactose Description of Module Subject Name Biochemistry Paper Name 04 Metabolism of Carbohydrates Module Name/Title 06 Entry of Fructose and Galactose 2 Metabolism of Carbohydrates Biochemistry Entry of Fructose and Galactose METABOLISM OF FRUCTOSE Objectives 1. To study the major pathway of fructose metabolism 2. To study specialized pathways of fructose metabolism 3. To study metabolism of galactose 4. To study disorders of galactose metabolism 3 Metabolism of Carbohydrates Biochemistry Entry of Fructose and Galactose Introduction Sucrose disaccharide contains glucose and fructose as monomers. Sucrose can be utilized as a major source of energy. Sucrose includes sugar beets, sugar cane, sorghum, maple sugar pineapple, ripe fruits and honey Corn syrup is recognized as high fructose corn syrup which gives the impression that it is very rich in fructose content but the difference between the fructose content in sucrose and high fructose corn syrup is only 5-10%. HFCS is rich in fructose because the sucrose extracted from the corn syrup is treated with the enzyme that converts some glucose in fructose which makes it more sweet. -
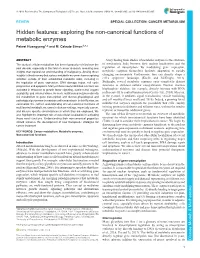
Exploring the Non-Canonical Functions of Metabolic Enzymes Peiwei Huangyang1,2 and M
© 2018. Published by The Company of Biologists Ltd | Disease Models & Mechanisms (2018) 11, dmm033365. doi:10.1242/dmm.033365 REVIEW SPECIAL COLLECTION: CANCER METABOLISM Hidden features: exploring the non-canonical functions of metabolic enzymes Peiwei Huangyang1,2 and M. Celeste Simon1,3,* ABSTRACT A key finding from studies of metabolic enzymes is the existence The study of cellular metabolism has been rigorously revisited over the of mechanistic links between their nuclear localization and the past decade, especially in the field of cancer research, revealing new regulation of transcription. By modulating gene expression, insights that expand our understanding of malignancy. Among these metabolic enzymes themselves facilitate adaptation to rapidly insights isthe discovery that various metabolic enzymes have surprising changing environments. Furthermore, they can directly shape a ’ activities outside of their established metabolic roles, including in cell s epigenetic landscape (Kaelin and McKnight, 2013). the regulation of gene expression, DNA damage repair, cell cycle Strikingly, several metabolic enzymes exert completely distinct progression and apoptosis. Many of these newly identified functions are functions in different cellular compartments. Nuclear fructose activated in response to growth factor signaling, nutrient and oxygen bisphosphate aldolase, for example, directly interacts with RNA ́ availability, and external stress. As such, multifaceted enzymes directly polymerase III to control transcription (Ciesla et al., 2014), -

Structure, Function, and Regulation of Intestinal Lactase-Phlorizin Hydrolase and Sucrase- Isomaltase in Health and Disease
Gastrointestinal Functions, edited by Edgard E. Delvin and Michael J. Lentze. Nestle Nutrition Workshop Series, Pediatric Program, Vol. 46. Nestec Ltd.. Vevey/Lippincott Williams & Wilkins. Philadelphia © 2001. Structure, Function, and Regulation of Intestinal Lactase-Phlorizin Hydrolase and Sucrase- Isomaltase in Health and Disease Hassan Y. Nairn Department of Physiological Chemistry, School of Veterinary Medicine Hannover, Hannover, Germany Carbohydrates are essential constituents of the mammalian diet. They occur as oligosaccharides, such as starch and cellulose (plant origin), as glycogen (animal origin), and as free disaccharides such as sucrose (plant) and lactose (animal). These carbohydrates are hydrolyzed in the intestinal lumen by specific enzymes to mono- saccharides before transport across the brush border membrane of epithelial cells into the cell interior. The specificity of the enzymes is determined by the chemical structure of the carbohydrates. The monosaccharide components of most of the known carbohydrates are linked to each other in an a orientation. Examples of this type are starch, glycogen, sucrose, and maltose. (3-Glycosidic linkages are minor. Nevertheless, this type of covalent bond is present in one of the major and most essential carbohydrates in mammalian milk, lactose, which constitutes the primary diet source for the newborn. The enzymes implicated in the digestion of carbohydrates in the intestinal lumen are membrane-bound glycoproteins that are expressed at the apical or microvillus membrane of the enterocytes (1-3). In this chapter, the structural and biosynthetic features of the most important disaccharidases, sucrase-isomaltase and lac- tase-phlorizin hydrolase, and the molecular basis of sugar malabsorption (i.e., en- zyme deficiencies) are discussed. -

Datasheet: VPA00226
Datasheet: VPA00226 Description: RABBIT ANTI ALDOA Specificity: ALDOA Format: Purified Product Type: PrecisionAb™ Polyclonal Isotype: Polyclonal IgG Quantity: 100 µl Product Details Applications This product has been reported to work in the following applications. This information is derived from testing within our laboratories, peer-reviewed publications or personal communications from the originators. Please refer to references indicated for further information. For general protocol recommendations, please visit www.bio-rad-antibodies.com/protocols. Yes No Not Determined Suggested Dilution Western Blotting 1/1000 PrecisionAb antibodies have been extensively validated for the western blot application. The antibody has been validated at the suggested dilution. Where this product has not been tested for use in a particular technique this does not necessarily exclude its use in such procedures. Further optimization may be required dependant on sample type. Target Species Human Species Cross Reacts with: Mouse, Rat Reactivity N.B. Antibody reactivity and working conditions may vary between species. Product Form Purified IgG - liquid Preparation Rabbit Ig fraction prepared by ammonium sulphate precipitation Buffer Solution Phosphate buffered saline Preservative 0.09% Sodium Azide (NaN3) Stabilisers Immunogen KLH conjugated synthetic peptide between 66-95 amino acids from the N-terminal region of human ALDOA External Database UniProt: Links P04075 Related reagents Entrez Gene: 226 ALDOA Related reagents Page 1 of 2 Synonyms ALDA Specificity Rabbit anti Human ALDOA antibody recognizes fructose-bisphosphate aldolase A, also known as epididymis secretory sperm binding protein Li 87p, fructose-1,6-bisphosphate triosephosphate-lyase, lung cancer antigen NY-LU-1 and muscle-type aldolase. Encoded by the ALDOA gene, fructose-bisphosphate aldolase A is a glycolytic enzyme that catalyzes the reversible conversion of fructose-1,6-bisphosphate to glyceraldehyde 3-phosphate and dihydroxyacetone phosphate. -

Dismetabolic Cataracts
ndrom Sy es tic & e G n e e n G e f T o Journal of Genetic Syndromes Cavallini et al., J Genet Syndr Gene Ther 2013, 4:7 h l e a r n a r p u DOI: 10.4172/2157-7412.1000165 y o J & Gene Therapy ISSN: 2157-7412 Case Report Open Access Dismetabolic Cataracts: Clinicopathologic Overview and Surgical Management with B-MICS Technique Cavallini GM1, Forlini M1, Masini C1, Campi L1, Chiesi C1, Rejdak R2 and Forlini C3* 1Institute of Ophthalmology, University of Modena, Modena, Italy 2Department of Ophthalmology, Medical University of Lublin, Lublin, Poland 3Department of Ophthalmology, “Santa Maria Delle Croci” Hospital, Ravenna, Italy Abstract Background: Dismetabolic cataract is a loss of lens transparency due to an insult to the nuclear or lenticular fibers, caused by a metabolic disorder. The lens opacification may occur early or later in life, and may be isolated or associated to particular syndromes. We describe some of these metabolic conditions associated with cataract formation, and in particular we report our experience with a patient affected by lathosterolosis that presented bilateral cataracts. Methods: Our patient was a 7-years-old little girl diagnosed with lathosterolosis at age 2 years, through gas cromatography/mass spectrometry method for plasma sterol profile that revealed a peak corresponding to cholest- 7-en-3β-ol (lathosterol). Results: The lens samples obtained during surgical removal with B-MICS technique were sent to the Department of Pathology and routinely processed and stained with haematoxylin-eosin and PAS; then, they were examined under a light microscope. Histological examination revealed lens fragments with the presence of fibers disposed in a honeycomb way, samples characterized by the presence of homogeneous eosinophilic lens fibers, and other fragments characterized by bulgy elements referable to cortical fibers with degenerative characteristics. -

Prevalence and Incidence of Rare Diseases: Bibliographic Data
Number 1 | January 2019 Prevalence and incidence of rare diseases: Bibliographic data Prevalence, incidence or number of published cases listed by diseases (in alphabetical order) www.orpha.net www.orphadata.org If a range of national data is available, the average is Methodology calculated to estimate the worldwide or European prevalence or incidence. When a range of data sources is available, the most Orphanet carries out a systematic survey of literature in recent data source that meets a certain number of quality order to estimate the prevalence and incidence of rare criteria is favoured (registries, meta-analyses, diseases. This study aims to collect new data regarding population-based studies, large cohorts studies). point prevalence, birth prevalence and incidence, and to update already published data according to new For congenital diseases, the prevalence is estimated, so scientific studies or other available data. that: Prevalence = birth prevalence x (patient life This data is presented in the following reports published expectancy/general population life expectancy). biannually: When only incidence data is documented, the prevalence is estimated when possible, so that : • Prevalence, incidence or number of published cases listed by diseases (in alphabetical order); Prevalence = incidence x disease mean duration. • Diseases listed by decreasing prevalence, incidence When neither prevalence nor incidence data is available, or number of published cases; which is the case for very rare diseases, the number of cases or families documented in the medical literature is Data collection provided. A number of different sources are used : Limitations of the study • Registries (RARECARE, EUROCAT, etc) ; The prevalence and incidence data presented in this report are only estimations and cannot be considered to • National/international health institutes and agencies be absolutely correct.