VISTARIL ® (Hydroxyzine Pamoate)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

XYZAL (Levocetirizine Dihydrochloride)
HIGHLIGHTS OF PRESCRIBING INFORMATION • Patients with end-stage renal impairment at less than 10 mL/min These highlights do not include all the information needed to use XYZAL creatinine clearance or patients undergoing hemodialysis (2.3, 4) safely and effectively. See full prescribing information for XYZAL. • Children 6 to 11 years of age with renal impairment (2.3, 4) ® XYZAL (levocetirizine dihydrochloride) ------------------------WARNINGS AND PRECAUTIONS----------------------- 5 mg tablets 2.5 mg/5 mL (0.5 mg/mL) oral solution • Avoid engaging in hazardous occupations requiring complete mental Initial U.S. Approval: 1995 alertness such as driving or operating machinery when taking XYZAL (5.1). ---------------------------RECENT MAJOR CHANGES--------------------------- • Avoid concurrent use of alcohol or other central nervous system Dosage and Administration (2) 01/2008 depressants with XYZAL (5.1). Dosage and Administration, Adults & Children 12 Years & Older (2.1) 01/2008 ------------------------------ADVERSE REACTIONS------------------------------ Dosage and Administration, Children 6 to 11 Years (2.2) 01/2008 The most common adverse reactions (rate ≥2% and > placebo) were ---------------------------INDICATIONS AND USAGE---------------------------- somnolence, nasopharyngitis, fatigue, dry mouth, and pharyngitis in subjects XYZAL is a histamine H1-receptor antagonist indicated for: 12 years of age and older, and pyrexia, somnolence, cough, and epistaxis in • The relief of symptoms associated with seasonal and perennial allergic -

Components of Respiratory Depression After Narcotic Premedication in Adolescents
COMPONENTS OF RESPIRATORY DEPRESSION AFTER NARCOTIC PREMEDICATION IN ADOLESCENTS R. KNILL*, J.F. Coscnowr P. M. OLLEY,AND H. LEVISON N~d~COTIC ACENTS are potent depressants of ventilation. 1-5 Although this effect is generally assumed to result from decreased output of the central respiratory "'centres," some of the effect could be due to direct action on the ventilatory apparatus itself, by increasing respiratory impendance. For example, both morphine and meperidine can cause bronchoconstriction;" furthermore they can increase the tonic activity of abdominal and intercostal muscles, r-l~ The mechanical effects of this increase in abdominal wall tone have not been assessed after thera- peutic doses of these agents, but large doses of narcotics administered intravenously produce board-like rigidity of the abdominal wall r-lo and markedly decrease total respiratory compliance? As the magnitude of this effect appears to be dose related 1~ it may well be present to a lesser extent after therapeutic doses of these agents. The purpose of this work was to determine whether the ventilatory depression associated with morphine and a meperidine-phenothiazine mixture is solely the result of impairment of the neuromuscular or force-generating mechanisms, or is in part due to increased impedance of the ventilatory pump. Even small increases in ventilatory load with narcotics probably contribute to ventilatory depression, as load compensation is poor when central neural mechanisms are pharmacologi- cally imp aired. 11,1a The conventional technique for examining the effect of narcotics on ventilation is to apply rebreathing and steady-state.methods before and after medication, to measure changes in minute ventilation (V~) and tidal volume (VT).13,~4 However, these measurements depend on both central output and the properties of the ventilatory apparatus, ~,16 without distinction between them. -
Journal Watch 1805 TCCC.Pdf
TCCC Journal Watch May 2018 Abou El Fadl M, O’Phelan K: Management of traumatic brain injury: an update. Neurosurg Clin N Am 2018;29:213-221 Abraham P,Russell D, Huffman S, et al: Army combat medic resilience: the process of forging loyalty. Mil Med 2018;183:364-370 Adravanti P, Di Salvo E, Calafiore G, et al: A prospective, randomized, comparative study of intravenous alone and combine intravenous and intraarticular administration of tranexamic acid in primary total knee replacement. Arthoplast Today 2017;4:85-88 Aggarwal N, Brower R, Hager D, et al: Oxygen exposure resulting in arterial oxygen tensions above the protocol goal was associated with worse clinical outcomes in acute respiratory distress syndrome. Crit Care Med 2018;46:517-524 Agimi Y, Regasa L, Ivins B, et al: Role of Department of Defense policies in identifying traumatic brain injuries among deployed US Service members 2001- 2016. Aiolfi A, Benjamin E, Recinos G, et al: Air versus ground transportation in isolated severe head trauma: a national trauma bank study. J Emerg Med 2018;54:328- 334 Aji Y, Apriawan T, Bajamal A: Traumatic supra- and infra-tentorial extradural hematoma: case series and literature review. Asian J Neurosurg 2018;13:453- 457 Akbari E, Safari S, Hatamabadi H: The effect of fibrinogen concentrate and fresh frozen plasma on the outcome of patients with acute traumatic coagulopathy: a quasi-experimental study. Am J Emerg Med 2018;Epub ahead of print. Aries M, Donnelly J: Brain oxygenation optimization after severe traumatic brain injury: an ode to preventing brain hypoxia. Crit Care Med 2018;46:e350 Armstrong R: Visual problems associated with traumatic brain injury. -
SIGHI-Leaflet Histamine Elimination Diet Simplified Histamine Elimination Diet for Histamine Intolerance (DAO Degradation Disorder)
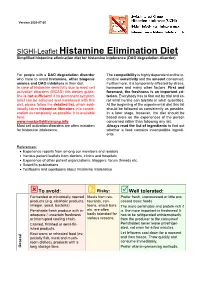
Version 2020-07-20 SIGHI-Leaflet Histamine Elimination Diet Simplified histamine elimination diet for histamine intolerance (DAO degradation disorder) For people with a DAO degradation disorder The compatibility is highly dependent on the in- who have to avoid histamine, other biogenic dividual sensitivity and the amount consumed. amines and DAO inhibitors in their diet. Furthermore, it is temporarily affected by stress, In case of histamine sensitivity due to mast cell hormones and many other factors. First and activation disorders (MCAD) this dietary guide- foremost, the freshness is an important cri- line is not sufficient! If no permanent symptom terion. Everybody has to find out by trial and er- relief can be achieved and maintained with this ror what he/she can tolerate in what quantities. diet, please follow the detailed list, which addi- At the beginning of the experimental diet this list tionally takes histamine liberators into consid- should be followed as consistently as possible. eration as completely as possible. It is available In a later stage, however, the diet should be here: based more on the experiences of the person www.mastzellaktivierung.info concerned rather than following any list. Mast cell activation disorders are often mistaken Always read the list of ingredients to find out for histamine intolerance. whether a food contains incompatible ingredi- ents. References: • Experience reports from among our members and readers • Various patient leaflets from doctors, clinics and hospitals • Experience of other patient organizations, bloggers, forum threads etc. • Scientific publications • Textbooks and cookbooks about histamine intolerance To avoid: ? Risky: Well tolerated: Fermented or microbially ripened Meals from res- Prefer fresh, unprocessed or little pro- products (e.g. -

Medications and Alcohol Craving
Medications and Alcohol Craving Robert M. Swift, M.D., Ph.D. The use of medications as an adjunct to alcoholism treatment is based on the premise that craving and other manifestations of alcoholism are mediated by neurobiological mechanisms. Three of the four medications approved in the United States or Europe for treating alcoholism are reported to reduce craving; these include naltrexone (ReVia™), acamprosate, and tiapride. The remaining medication, disulfiram (Antabuse®), may also possess some anticraving activity. Additional medications that have been investigated include ritanserin, which has not been shown to decrease craving or drinking levels in humans, and ondansetron, which shows promise for treating early onset alcoholics, who generally respond poorly to psychosocial treatment alone. Use of anticraving medications in combination (e.g., naltrexone plus acamprosate) may enhance their effectiveness. Future studies should address such issues as optimal dosing regimens and the development of strategies to enhance patient compliance. KEY WORDS: AOD (alcohol and other drug) craving; anti alcohol craving agents; alcohol withdrawal agents; drug therapy; neurobiological theory; alcohol cue; disulfiram; naltrexone; calcium acetylhomotaurinate; dopamine; serotonin uptake inhibitors; buspirone; treatment outcome; reinforcement; neurotransmitters; patient assessment; literature review riteria for defining alcoholism Results of craving research are often tions (i.e., pharmacotherapy) to improve vary widely. Most definitions difficult to interpret, -

New York State Medicaid Drug Utilization Review Board Meeting Agenda
New York State Medicaid Drug Utilization Review Board Meeting Agenda The Drug Utilization Review (DUR) Board will meet on April 27, 2016, from 9:00 a.m. to 4:00 p.m., Meeting Room 6, Concourse, Empire State Plaza, Albany, New York Agenda Items A. Preferred Drug Program (PDP) The DUR Board will review therapeutic classes listed below, as they pertain to the PDP. The DUR Board will review clinical and financial information, to recommend preferred and non-preferred drugs. For therapeutic classes currently subject to the PDP^, the DUR Board will only consider clinical information which is new since the previous review of the therapeutic class and then consider financial information. New clinical information may include a new drug or drug product information, new indications, new safety information or new published clinical trials (comparative evidence is preferred, or placebo controlled when no head-to-head trials are available). Information in abstract form alone, posters, or unpublished data are poor quality evidence for the purpose of re-review and submission is discouraged. Those wishing to submit new clinical information must do so in an electronic format by April 12, 2016 or the Board may not have ample time to review the information. ^ The current preferred and non-preferred status of drugs subject to the Preferred Drug List (PDL) may be viewed at https://newyork.fhsc.com/downloads/providers/NYRx_PDP_PDL.pdf 1. Non-Steroidal Anti-Inflammatory Drugs (NSAIDS) – Prescription (Previous review date: April 22, 2015) Anaprox DS (naproxen -

THE USE of MIRTAZAPINE AS a HYPNOTIC O Uso Da Mirtazapina Como Hipnótico Francisca Magalhães Scoralicka, Einstein Francisco Camargosa, Otávio Toledo Nóbregaa
ARTIGO ESPECIAL THE USE OF MIRTAZAPINE AS A HYPNOTIC O uso da mirtazapina como hipnótico Francisca Magalhães Scoralicka, Einstein Francisco Camargosa, Otávio Toledo Nóbregaa Prescription of approved hypnotics for insomnia decreased by more than 50%, whereas of antidepressive agents outstripped that of hypnotics. However, there is little data on their efficacy to treat insomnia, and many of these medications may be associated with known side effects. Antidepressants are associated with various effects on sleep patterns, depending on the intrinsic pharmacological properties of the active agent, such as degree of inhibition of serotonin or noradrenaline reuptake, effects on 5-HT1A and 5-HT2 receptors, action(s) at alpha-adrenoceptors, and/or histamine H1 sites. Mirtazapine is a noradrenergic and specific serotonergic antidepressive agent that acts by antagonizing alpha-2 adrenergic receptors and blocking 5-HT2 and 5-HT3 receptors. It has high affinity for histamine H1 receptors, low affinity for dopaminergic receptors, and lacks anticholinergic activity. In spite of these potential beneficial effects of mirtazapine on sleep, no placebo-controlled randomized clinical trials of ABSTRACT mirtazapine in primary insomniacs have been conducted. Mirtazapine was associated with improvements in sleep on normal sleepers and depressed patients. The most common side effects of mirtazapine, i.e. dry mouth, drowsiness, increased appetite and increased body weight, were mostly mild and transient. Considering its use in elderly people, this paper provides a revision about studies regarding mirtazapine for sleep disorders. KEYWORDS: sleep; antidepressive agents; sleep disorders; treatment� A prescrição de hipnóticos aprovados para insônia diminuiu em mais de 50%, enquanto de antidepressivos ultrapassou a dos primeiros. -

An Evidence-Based Guideline for the Pre-Operative Sedation of Children
Journal of Pediatrics and Neonatal Care An Evidence-Based Guideline for the Pre-Operative Sedation of Children Abstract Review Article There are numerous sedative pharmacological agents currently administered to Volume 2 Issue 6 - 2015 children as premedicants to facilitate the induction of anaesthesia. When pre- operative sedation is required, selection of the appropriate drug is imperative to Deborah M Fradkin*, Victoria L Scott- provide adequate anxiolysis whilst minimising unwanted side effects. We review Warren, Rita Vashisht and Sian E Rolfe the literature regarding the merits and limitations of the commonly used agents and suggest evidence based practical guidance. For the anxious but cooperative Department of Paediatric Anaesthesia, Royal Manchester Children’s Hospital, England child, oral midazolam is often adequate; however with more anxious younger and uncooperative children, combined oral midazolam and ketamine is more *Corresponding author: DM. Fradkin, Department of effective. Other oral benzodiazepines and oral clonidine all have their role when Paediatric Anaesthesia, Royal Manchester Children’s used in the appropriate circumstances. Intranasal clonidine is useful in the child Hospital, Oxford Road, Manchester, M13 9WL, England, Tel: refusing oral medication. Intramuscular ketamine should be reserved for extreme 0161 701 1264; Email: circumstances, administered only by anaesthetists experienced in its use, with full monitoring and resuscitative equipment immediately available. Received: August 15, 2015 | Published: September -

Safety and Efficacy of a Continuous Infusion, Patient Controlled Anti
Bone Marrow Transplantation, (1999) 24, 561–566 1999 Stockton Press All rights reserved 0268–3369/99 $15.00 http://www.stockton-press.co.uk/bmt Safety and efficacy of a continuous infusion, patient controlled anti- emetic pump to facilitate outpatient administration of high-dose chemotherapy SP Dix, MK Cord, SJ Howard, JL Coon, RJ Belt and RB Geller Blood and Marrow Transplant Program, Oncology and Hematology Associates and Saint Luke’s Hospital of Kansas City, Kansas City, MO, USA Summary: and colleagues1 described an outpatient BMT care model utilizing intensive clinic support following inpatient admin- We evaluated the combination of diphenhydramine, lor- istration of HDC. This approach facilitated early patient azepam, and dexamethasone delivered as a continuous discharge and significantly decreased the total number of i.v. infusion via an ambulatory infusion pump with days of hospitalization associated with BMT. More patient-activated intermittent dosing (BAD pump) for recently, equipped BMT centers have extended the out- prevention of acute and delayed nausea/vomiting in patient care approach to include administration of HDC in patients receiving high-dose chemotherapy (HDC) for the clinic setting. Success of the total outpatient care peripheral blood progenitor cell (PBPC) mobilization approach is dependent upon the availability of experienced (MOB) or prior to autologous PBPC rescue. The BAD staff and necessary resources as well as implementation of pump was titrated to patient response and tolerance, supportive care strategies designed to minimize morbidity and continued until the patient could tolerate oral anti- in the outpatient setting. emetics. Forty-four patients utilized the BAD pump Despite improvements in supportive care strategies, during 66 chemotherapy courses, 34 (52%) for MOB chemotherapy-induced nausea and vomiting continues to be and 32 (48%) for HDC with autologous PBPC rescue. -

Premedication in Pedodontics Attitudes and Agents
PEDIATRICDENTISTRY/Copyright ~) 1979 by The American Academyof Pedodontics/ Vol. 1, No. 4 / Printed in U.S.A. Premedication in Pedodontics Attitudes and Agents David L. King, D.D.S., Ph.D. William C. Berlocher, D.D.S. Abstract a dentist should find it necessary to resort to premed- icating children to obtain their cooperation. Garfin The goals of premedicationin children’s dentistry are to feels that the routine use of sedatives and tranquiliz- allay excessive apprehensionand to prevent resistance to treatment efforts. With judicious use, premedicatingagents ers may rbflect a "decreased interest in the care and are a valuable and necessary adjunct for the pedodontis~. treatment of the complete child," and Olsen proposes Whenintegrated with proper psychological approaches, that dentists examine their motives to see if they em- premedicationmay enable the anxious child to accept his ploy premedication as a "crutch." Both of these au- first dental experiences without undueemotional turmoil thors emphasize that when faced with a potential or it mayoften allow outpatient treatment of very young management problem, proper psychological ap- "precooperative" children wherethe only alternative might proaches by the dentist will obviate the need for drugs be hospitalization and general anesthesia. Prudent employ- in most instances. MacGregorbelieves the dentist who ment of drugs [or behavior managementis dependent on resorts to premedication or general anesthesia may the training, experience, and iudgementof the operator. actually be treating his own fears and admitting his A regimen of premedicant drugs and dosages is presented inability to manage children. which may serve as base line guidance [or more successful 7 managementof the difficult child patient. -

Acute Migraine Treatment
Acute Migraine Treatment Morris Levin, MD Professor of Neurology Director, Headache Center UCSF Department of Neurology San Francisco, CA Mo Levin Disclosures Consulting Royalties Allergan Oxford University Press Supernus Anadem Press Amgen Castle Connolly Med. Publishing Lilly Wiley Blackwell Mo Levin Disclosures Off label uses of medication DHE Antiemetics Zolmitriptan Learning Objectives At the end of the program attendees will be able to 1. List all important options in the acute treatment of migraine 2. Discuss the evidence and guidelines supporting the major migraine acute treatment options 3. Describe potential adverse effects and medication- medication interactions in acute migraine pharmacological treatment Case 27 y/o woman has suffered ever since she can remember from “sick headaches” . Pain is frontal, increases over time and is generally accompanied by nausea and vomiting. She feels depressed. The headache lasts the rest of the day but after sleeping through the night she awakens asymptomatic 1. Diagnosis 2. Severe Headache relief Diagnosis: What do we need to beware of? • Misdiagnosis of primary headache • Secondary causes of headache Red Flags in HA New (recent onset or change in pattern) Effort or Positional Later onset than usual (middle age or later) Meningismus, Febrile AIDS, Cancer or other known Systemic illness - Neurological or psych symptoms or signs Basic principles of Acute Therapy of Headaches • Diagnose properly, including comorbid conditions • Stratify therapy rather than treat in steps • Treat early -
Hydroxyzine Prescribing Information
Hydroxyzine Hydroxyzine Hydrochloride Hydrochloride Injection, USP Injection, USP (For Intramuscular Use Only) (For Intramuscular Use Only) Rx Only Rx Only DESCRIPTION: Hydroxyzine hydrochloride has the chemical name of (±)-2-[2-[4-( p-Chloro- a- phenylbenzyl)-1-piperazinyl]ethoxy]ethanol dihydrochloride and occurs as a white, odorless powder which is very soluble in water. It has the following structural formula: Molecular Formula: C 21 H27 ClN 2O2•2HCl Molecular Weight: 447.83 Hydroxyzine Hydrochloride Injection, USP is a sterile aqueous solution intended for intramuscular administration. Each mL contains: Hydroxyzine HCl 25 mg or 50 mg, Benzyl Alcohol 0.9%, and Water for Injection q.s. pH adjusted with Sodium Hydroxide and/or Hydrochloric Acid. CLINICAL PHARMACOLOGY: Hydroxyzine hydrochloride is unrelated chemically to phenothiazine, reserpine, and meprobamate. Hydroxyzine has demonstrated its clinical effectiveness in the chemotherapeutic aspect of the total management of neuroses and emotional disturbances manifested by anxiety, tension, agitation, apprehension or confusion. Hydroxyzine has been shown clinically to be a rapid-acting true ataraxic with a wide margin of safety. It induces a calming effect in anxious, tense, psychoneurotic adults and also in anxious, hyperkinetic children without impairing mental alertness. It is not a cortical depressant, but its action may be due to a suppression of activity in certain key regions of the subcortical area of the central nervous system. Primary skeletal muscle relaxation has been demonstrated experimentally. Hydroxyzine has been shown experimentally to have antispasmodic properties, apparently mediated through interference with the mechanism that responds to spasmogenic agents such as serotonin, acetylcholine, and histamine. Antihistaminic effects have been demonstrated experimentally and confirmed clinically.