Micro Strategic Action Plan for Malaria
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

014 5891Ny0504 88 93
New York Science Journal 2012;5(7) http://www.sciencepub.net/newyork Estimation of Area under Winter Vegetables in Punjab Districts: through Remote Sensing & GIS Technology 1 Singh Avtar, 2 Khanduri Kamlesh 1 Technical Associate, JRF,Forest Survey of India(FSI),Dehradun,India 2D.Phil Research Scholar,Dpt. of Geography,HNBGU,JRF(FSI), Uttrakhand,India [email protected] Abstract: The Study area consists of five northern districts (ex.Gurdaspur) of Punjab State, namely, Amritsar, Tarn Taran, Kapurthala, Jalandhar and Hoshiarpur. In this study, Acreage Estimation of Vegetables in northern Punjab is carried out by using Multidate IRS - P6 AWiFS Data sets of seven dates viz., September (30), October (14, 24), November (17), December (25), January (4, 13). The aim of this study is to detect area estimation under winter vegetables in Punjab districts between 2005 - 2008 using satellite images. Vegetable area carried out by decision rule based classification: two models are created, one for acreage estimation of vegetables the other for generation of NDVI of all date satellite data. After classification of the image, classified image is recoded to merge different classes of the single output category in one category. Winter Vegetables have been detected by image processing method in EDRAS imagine9.3, ArcGIS9.3. In study area, as a whole there is positive change (14.9%) in area under vegetable crop. But two districts, namely, Kapurthala and Jalandhar have experienced negative change .But in another three districts Amritsar, Tarn Taran and Hoshiarpur districts have recorded positive change in area under vegetable. [Singh Avtar, Khanduri Kamlesh. Estimation of Area under Winter Vegetables in Punjab Districts: through Remote Sensing & GIS Technology. -
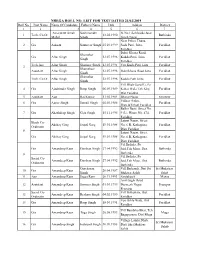
NREGA ROLL NO. LIST for TEST DATED 21/02/2019 Roll No
NREGA ROLL NO. LIST FOR TEST DATED 21/02/2019 Roll No. Post Name Name Of Candidate Father's Name Dob Address District 1 2 3 4 5 6 7 Amarpreet Singh Sukhmander St.No.1,Sahibjada Jujar 1 Tech. Co.Or. 13.02.1990 Bathinda Mahal Singh Singh Nagar Near Police Thana, 2 Grs Aakash Sukhveer Singh 25.10.1999 Sada Patti, Jaito, Faridkot Faridkot Dabri Khana Road, Shemsher Grs Aftar Singh 12.07.1996 Kuddo Patti, Jaito, Faridkot Singh Faridkot Tech.Ass. Aftar Singh Shamser Singh 12.07.1996 Vpo Kudo Patti Jaitu Faridkot 3 Shamsheer Assistant Aftar Singh 12.07.1996 Dabrikhana Road Jaitu Faridkot Singh Shamsher Tech. Co.Or. Aftar Singh 12.07.1996 Kaddo Patti Jaito Faridkot Singh Vill Dhab Guru Ki, Po 4 Grs Ajadvinder Singh Roop Singh 06.09.1989 Kohar Wala Teh:Kkp, Faridkot Dist Faridkot 5 Assistant Ajay Raj Kumar 13.02.1989 Bharat Nagar, Ferozpur Village Sadiq, 6 Grs Ajmer Singh Jarnail Singh 05.03.1988 Faridkot Distt.&Tehsel Faridkot Balbir Basti, Street No. 7 Grs Akashdeep Singh Geja Singh 15.11.1995 9 (L), House No. 474, Faridkot Faridkot Lajpat Nagar, Street Block Co- Akshay Garg Jaipal Garg 19.01.1988 No. 6 B, Kotkapura, Faridkot Ordinator 8 Distt Faridkot Lajpat Nagar, Street Grs Akshay Garg Jaipal Garg 19.01.1988 No. 6 B, Kotkapura, Faridkot Distt Faridkot Vil Badiala, Po Grs Amandeep Kaur Darshan Singh 27.04.1992 Jaid,Teh Mour, Dist Bathinda 9 Bathinda Vil Badiala, Po Social Co- Amandeep Kaur Darshan Singh 27.04.1992 Jaid,Teh Mour, Dist Bathinda Ordinator Bathinda Gurcharan Vill Barkandi, Dist Sri Sri Mukatsar 10 Grs Amandeep Kaur 20.04.1987 -

Village & Townwise Primary Census Abstract, Ludhiana, Part
CENSUS OF INDIA 1991 SERIES-20 PUNJAB DISTRICT 'CENSUS HANDBOOK PART XII - A & B VILLAGE &TOWN DIRECTORY VILLAGE & TOWNWISE PRIMARY CENSUS ABSTRACT DISTRICT LUDHIANA Director of· Census Operations Punjab I I • G ~ :x: :x: ~.• Q - :r i I I@z@- ~ . -8. till .11:: I I ,~: : ,. 1l •., z ... , z . Q II) · 0 w ::t ; ~ ~ :5 ... ...J .... £ ::::> ~ , U , j:: .. « c.. tJ) ~ 0 w . ~ c.. t,! ' !!; I! 0 II) <> I « w .... ... 0 i3 z « ~ Vi at: 0 U .· [Il (J) W :x: ;::: U Z 0 « « « ii. 0- 0 c;: J: .., Z 0 ... u .~ « a ::::> u_ w t- 0 ;:: : : c.. 0 ... ~ U at: « ~ a ~ '0 x I- : :x: a: II) 0 c.. 0 .. U 0 c.. ... z ~ 0 Iii w ~ 8 « ... ...J :x: :x: « .. U ~~ i5~ ...J « : 0:: ;; 0- II) t: W => ~ C2 oct '"~ w 0- 5: :x: c:i Vi::: ;: 0:: 0 w I.!l .. Iii W I- ... W . ~ « at::x: ~ IJ) ~ i5 U w~ ~ w «z w ... .... ... s: «w> w<t t- <:l .w ~ &:3: :x: 0- 6 e at: ...J :X:z: 0 ulI) U ~ « ... I.!l Z «~ ::::> ";;: « « x <t w« z w. a A 0 z ~ ~ I.!lZ ZH'" « WI :x: .... Z t a0 0 w (l: ' 5: a::: «,.. ;j o .J W :3:x: [Il .... a::: ::::> « ;:: ~ c.. - _,O- Iii I.!l Iii a w « 0- > 0:":: 0 W W tS- [Il ~_ «(l: :x: z . Ul ii1 >s: ::::> .... c.. e, 0:: ui a: w <t. (i -z. « « a0 <[ w I :x: 0 --' m iii ::> :x: ...J « ~ 0- z l- < 0 ::::> 0:: UI t- e/) :g N ...J --' o. -

State Profiles of Punjab
State Profile Ground Water Scenario of Punjab Area (Sq.km) 50,362 Rainfall (mm) 780 Total Districts / Blocks 22 Districts Hydrogeology The Punjab State is mainly underlain by Quaternary alluvium of considerable thickness, which abuts against the rocks of Siwalik system towards North-East. The alluvial deposits in general act as a single ground water body except locally as buried channels. Sufficient thickness of saturated permeable granular horizons occurs in the flood plains of rivers which are capable of sustaining heavy duty tubewells. Dynamic Ground Water Resources (2011) Annual Replenishable Ground water Resource 22.53 BCM Net Annual Ground Water Availability 20.32 BCM Annual Ground Water Draft 34.88 BCM Stage of Ground Water Development 172 % Ground Water Development & Management Over Exploited 110 Blocks Critical 4 Blocks Semi- critical 2 Blocks Artificial Recharge to Ground Water (AR) . Area identified for AR: 43340 sq km . Volume of water to be harnessed: 1201 MCM . Volume of water to be harnessed through RTRWH:187 MCM . Feasible AR structures: Recharge shaft – 79839 Check Dams - 85 RTRWH (H) – 300000 RTRWH (G& I) - 75000 Ground Water Quality Problems Contaminants Districts affected (in part) Salinity (EC > 3000µS/cm at 250C) Bhatinda, Ferozepur, Faridkot, Muktsar, Mansa Fluoride (>1.5mg/l) Bathinda, Faridkot, Ferozepur, Mansa, Muktsar and Ropar Arsenic (above 0.05mg/l) Amritsar, Tarantaran, Kapurthala, Ropar, Mansa Iron (>1.0mg/l) Amritsar, Bhatinda, Gurdaspur, Hoshiarpur, Jallandhar, Kapurthala, Ludhiana, Mansa, Nawanshahr, -
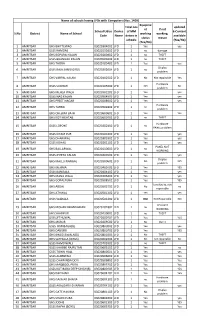
List of Schools Having Lfds
Name of schools having LFDs with Computers (Nos. 1400) Equipme Total nos updated nt If not School Udise Device of MM E-Content S.No District Name of School working working, Code Name deices in available status reason schools (Yes/No) (Yes/No) 1 AMRITSAR GHS BHITTEWAD 03020304002 LFD 1 Yes yes 2 AMRITSAR GSSS RAMDAS 03020111602 LFD 1 no damage 3 AMRITSAR GHS BOPARAI KALAN 03020200402 LFD 1 no THEFT 4 AMRITSAR GSSS BHANGALI KALAN 03020503002 LFD 1 no THEFT 5 AMRITSAR GHS THOBA 03020105402 LFD 1 Yes yes Display 6 AMRITSAR GSSS RAJA SANSI GIRLS 03020302604 LFD 1 no problem 7 AMRITSAR GHS VARPAL KALAN 03020402502 LFD 1 No Not repairable Yes Hardware 8 AMRITSAR GSSS SUDHAR 03020105002 LFD 1 NO No problem 9 AMRITSAR GHS MEHLA WALA 03020302202 LFD 1 Yes yes 10 AMRITSAR GSSS NAG KALAN 03020504903 LFD 1 Yes yes 11 AMRITSAR GHS PREET NAGAR 03020208902 LFD 1 Yes yes Hardware 12 AMRITSAR GHS TARPAI 03020502802 LFD 1 no problem 13 AMRITSAR GHS CHEEMA BATH 03020600602 LFD 1 Yes Yes 14 AMRITSAR GHS KOT MEHTAB 03020600702 LFD 1 no THEFT Hardware 15 AMRITSAR GSSS LOPOKE 03020202402 LFD 1 no PANEL problem 16 AMRITSAR GSSS KIYAM PUR 03020101002 LFD 1 Yes yes 17 AMRITSAR GHS DHARIWAL 03020303302 LFD 1 Yes yes 18 AMRITSAR GSSS KOHALI 03020201102 LFD 1 Yes yes PANEL NOT 19 AMRITSAR GHS BALLARWAL 03020110002 LFD 1 no WORKING 20 AMRITSAR GSSS JHEETA KALAN 03020400102 LFD 1 Yes yes Display 21 AMRITSAR GHS MALLU NANGAL 03020300602 LFD 1 No NO problem 22 AMRITSAR GHS MEHMA 03020400702 LFD 1 Yes YES 23 AMRITSAR GSSS BANDALA 03020404402 LFD 1 Yes yes 24 AMRITSAR GHS -
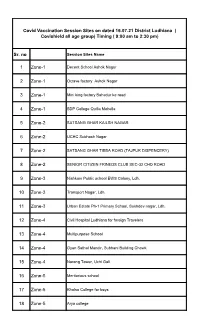
Sr. No 1 Zone-1 2 Zone-1 3 Zone-1 4 Zone-1 5 Zone-2 6 Zone-2 7 Zone-2
Covid Vaccination Session Sites on dated 16.07.21 District Ludhiana ( Covishield all age group) Timing ( 9:00 am to 2:30 pm) Sr. no Session Sites Name 1 Zone-1 Decent School Ashok Nagar 2 Zone-1 Octave factory Ashok Nagar 3 Zone-1 Mini king factory Bahadur ke road 4 Zone-1 SDP College Quilla Mohella 5 Zone-2 SATSANG GHAR KAILSH NAGAR 6 Zone-2 UCHC Subhash Nagar 7 Zone-2 SATSANG GHAR TIBBA ROAD (TAJPUR DISPENCERY) 8 Zone-2 SENIOR CITIZEN FRINEDS CLUB SEC-32 CHD ROAD 9 Zone-3 Nishkam Public school EWS Colony, Ldh. 10 Zone-3 Transport Nagar, Ldh. 11 Zone-3 Urban Estate Ph-1 Primary School, Sukhdev nagar, Ldh. 12 Zone-4 Civil Hospital Ludhiana for foreign Travelers 13 Zone-4 Multipurpose School 14 Zone-4 Gyan Sathal Mandir, Subhani Building Chowk 15 Zone-4 Narang Tower, Uchi Gali 16 Zone-5 Meritorious school 17 Zone-5 Khalsa College for boys 18 Zone-5 Arya college 19 Zone-5 GSS kalan 20 Zone-5 GSS kundanpuri. 21 Zone-6 uphc bhagwan nagar 22 Zone-6 uphc dholewal 23 Zone-6 Gurdwara Singh Sabha Akal Sahib Partap Nagar 24 Zone-6 Preach convent international school krishna nagar , Giaspura 25 Zone-7 UCHC SHIMALAPURI 26 Zone-7 GNE COLLEGE GILL ROAD 27 Zone-7 ITI,SKILL DEVLOPMENT CENTRE GILL ROAD GURUDWARA KARAM SAR SAHIB WARD NO 42 ARJAN NAGAR 28 Zone-7 RADHA SWAMI ROAD GILL ROAD 29 Zone-7 BHOGAL SONS IND AREA B732 NEAR PAHWA HOSPITAL 30 Zone-8 MGM SCHOOL PH-1 DUGRI 31 Zone-8 MANJIT NAGAR DHARAMSHALA GALI NO 12 32 Zone-8 GAD MODEL GRAM 33 Zone-8 AMBEDKAR NAGAR NEAR PURI NURSING HOME 34 Zone-9 UCHC JAWADDI 35 Zone-9 ROTARY CLUB 36 Jagraon GOVT SCHOOL BOYS 37 Jagraon GOVT SCHOOL GIRLS 38 Jagraon SDH JAGRAON 39 Khanna GOVT.SEN.SEC.SCHOOL ,BACK SIDE GTB MARKET KHANNA 40 Khanna CIVIL HOSPITAL KHANNA 41 Khanna LADY HOSPITAL,JARAG CHOWNK KHANNA 42 Samrala Sdh samrala 43 Samrala Govt. -

Pincode Officename Statename Minisectt Ropar S.O Thermal Plant
pincode officename districtname statename 140001 Minisectt Ropar S.O Rupnagar PUNJAB 140001 Thermal Plant Colony Ropar S.O Rupnagar PUNJAB 140001 Ropar H.O Rupnagar PUNJAB 140101 Morinda S.O Ropar PUNJAB 140101 Bhamnara B.O Rupnagar PUNJAB 140101 Rattangarh Ii B.O Rupnagar PUNJAB 140101 Saheri B.O Rupnagar PUNJAB 140101 Dhangrali B.O Rupnagar PUNJAB 140101 Tajpura B.O Rupnagar PUNJAB 140102 Lutheri S.O Ropar PUNJAB 140102 Rollumajra B.O Ropar PUNJAB 140102 Kainaur B.O Ropar PUNJAB 140102 Makrauna Kalan B.O Rupnagar PUNJAB 140102 Samana Kalan B.O Rupnagar PUNJAB 140102 Barsalpur B.O Ropar PUNJAB 140102 Chaklan B.O Rupnagar PUNJAB 140102 Dumna B.O Ropar PUNJAB 140103 Kurali S.O Mohali PUNJAB 140103 Allahpur B.O Mohali PUNJAB 140103 Burmajra B.O Rupnagar PUNJAB 140103 Chintgarh B.O Rupnagar PUNJAB 140103 Dhanauri B.O Rupnagar PUNJAB 140103 Jhingran Kalan B.O Rupnagar PUNJAB 140103 Kalewal B.O Mohali PUNJAB 140103 Kaishanpura B.O Rupnagar PUNJAB 140103 Mundhon Kalan B.O Mohali PUNJAB 140103 Sihon Majra B.O Rupnagar PUNJAB 140103 Singhpura B.O Mohali PUNJAB 140103 Sotal B.O Rupnagar PUNJAB 140103 Sahauran B.O Mohali PUNJAB 140108 Mian Pur S.O Rupnagar PUNJAB 140108 Pathreri Jattan B.O Rupnagar PUNJAB 140108 Rangilpur B.O Rupnagar PUNJAB 140108 Sainfalpur B.O Rupnagar PUNJAB 140108 Singh Bhagwantpur B.O Rupnagar PUNJAB 140108 Kotla Nihang B.O Ropar PUNJAB 140108 Behrampur Zimidari B.O Rupnagar PUNJAB 140108 Ballamgarh B.O Rupnagar PUNJAB 140108 Purkhali B.O Rupnagar PUNJAB 140109 Khizrabad West S.O Mohali PUNJAB 140109 Kubaheri B.O Mohali PUNJAB -

RMSA-HEAD MASTER Page 1
RMSA-HEAD MASTER Govt Comm Ex- Physical Registration Mother's Catego Freedom Sports . ittee SR.NO Name Father's Name Servicem Handica P_Address P_District Observations Number Name ry Fighter Person Serv No an p ant 1. EXPERIENCE CERTIFICATE IS NOT COUNTER Not Not Not V&PO SIGNED BY DEO HEM RAJ SHAKUNTLA 2. EXPERIENCE AS PRT CADRE . 1 1 R001-00036123 KAMINI MANRO General Applicabl Applicabl Applicabl No No MULLANPUR S.A.S. NAGAR MANRO MANRO 3. TWO EXPERIENCE CERTIFICATES ISSUED ON 10- e e e GARIBDASS 02-14. 4.INSUFFICIENT EXPERIENCE. 1. INSUFFICIENT EXPERIENCE 2. EXPERIENCE CERTIFICATES ISSUED ON 10-02-14 Not Not Not AMANDEEP HARBANS SARDOOL SINGH VPO & 11-02-14. 1 2 R001-00033669 BALTEJ SINGH General Applicabl Applicabl Applicabl No No FARIDKOT 3. EXP. CERT. HAS NOT BEEN COUNTERSIGNED BY KAUR KAUR BHAGTHALA KHURD e e e DEO 4. EXP. CERT. NOT PRODUCED ON REQUIRED PERFORMA Not Not Not 1) BPED AND MPED FROM NAGPUR UNI IN 1998- NIRANJAN NEAR BOYS SCHOOL, 2001 1 3 R001-00006154 HARJIT SINGH BALDEV SINGH General Applicabl Applicabl Applicabl No No MANSA KAUR VPO JOGA 2) MPHILL FROM VINAYAKA UNIV IN 2009. e e e 3) EXPERIENCE CERTIFICATE ISSUED ON 07-02-14 W/O ANIL JASUJA Not Not Not SUBHASH SANTOSH RADHA SWAMI 1 4 R001-00032469 SHIVANI General Applicabl Applicabl Applicabl No No FAZILKA 1. INSUFFICIENT EXPERIENCE CHANDER SACHDEVA COLONY STREET NO 1 e e e HOUSE NO A 1049 FAZILKA H NO 2449 2ND Not Not Not RAM CHANDER MEENA CROSSING ST NO 6 1 5 R001-00002246 DEEPTY THAKUR General Applicabl Applicabl Applicabl No No FAZILKA 1.EXPERIENCE CERTIFICATE ISSUED ON 29-12-13 THAKUR THAKUR SIDHU NAGRI e e e ABOHAR RAJIV MONGA C/O 1. -
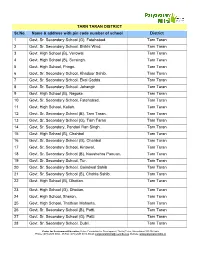
TARN TARAN DISTRICT Sr.No. Name & Address With
TARN TARAN DISTRICT Sr.No. Name & address with pin code number of school District 1 Govt. Sr. Secondary School (G), Fatehabad. Tarn Taran 2 Govt. Sr. Secondary School, Bhikhi Wind. Tarn Taran 3 Govt. High School (B), Verowal. Tarn Taran 4 Govt. High School (B), Sursingh. Tarn Taran 5 Govt. High School, Pringri. Tarn Taran 6 Govt. Sr. Secondary School, Khadoor Sahib. Tarn Taran 7 Govt. Sr. Secondary School, Ekal Gadda. Tarn Taran 8 Govt. Sr. Secondary School, Jahangir Tarn Taran 9 Govt. High School (B), Nagoke. Tarn Taran 10 Govt. Sr. Secondary School, Fatehabad. Tarn Taran 11 Govt. High School, Kallah. Tarn Taran 12 Govt. Sr. Secondary School (B), Tarn Taran. Tarn Taran 13 Govt. Sr. Secondary School (G), Tarn Taran Tarn Taran 14 Govt. Sr. Secondary, Pandori Ran Singh. Tarn Taran 15 Govt. High School (B), Chahbal Tarn Taran 16 Govt. Sr. Secondary School (G), Chahbal Tarn Taran 17 Govt. Sr. Secondary School, Kirtowal. Tarn Taran 18 Govt. Sr. Secondary School (B), Naushehra Panuan. Tarn Taran 19 Govt. Sr. Secondary School, Tur. Tarn Taran 20 Govt. Sr. Secondary School, Goindwal Sahib Tarn Taran 21 Govt. Sr. Secondary School (B), Chohla Sahib. Tarn Taran 22 Govt. High School (B), Dhotian. Tarn Taran 23 Govt. High School (G), Dhotian. Tarn Taran 24 Govt. High School, Sheron. Tarn Taran 25 Govt. High School, Thathian Mahanta. Tarn Taran 26 Govt. Sr. Secondary School (B), Patti. Tarn Taran 27 Govt. Sr. Secondary School (G), Patti. Tarn Taran 28 Govt. Sr. Secondary School, Dubli. Tarn Taran Centre for Environment Education, Nehru Foundation for Development, Thaltej Tekra, Ahmedabad 380 054 India Phone: (079) 2685 8002 - 05 Fax: (079) 2685 8010, Email: [email protected], Website: www.paryavaranmitra.in 29 Govt. -

Unpaid Dividend Details 2017-18
Proposed Date Folio Amount Member Name Father/Husband Name Address Country State PIN Code Investment Type of Transfer to Number Transferred IEPF VILL. BALIAL BHAWANIGARH MOONAK Amount for unclaimed and JAGJIT SINGH GURTEJ SINGH INDIA PUNJAB 148026 0000010 280.00 02-Nov-2025 TEHSIL &, DISTT. SANGRUR PUNJAB, unpaid dividend CHATHA NANHERA SUNAM CHATHA Amount for unclaimed and CHARANJIT KAUR BIKAR SINGH INDIA PUNJAB 148028 0000018 40.00 02-Nov-2025 NANHERA 148028 SA, NGRUR PUNJAB, unpaid dividend GUJRAN SUNAM GUJRAN SANGRUR Amount for unclaimed and MUKHTIAR KAUR LAL DEEN INDIA PUNJAB 148028 0000026 40.00 02-Nov-2025 PUNJAB, , unpaid dividend Amount for unclaimed and RANO RANI RULDU RAM GUJRAN,SUNAM, GUJRAN, SANGRUR INDIA PUNJAB 148028 0000027 40.00 02-Nov-2025 unpaid dividend RETGARH BHWAWANIGARH Amount for unclaimed and AJMER KAUR DALIP SINGH INDIA PUNJAB 148026 0000055 40.00 02-Nov-2025 BHAWANIGARH SANGR, UR PUNJAB, unpaid dividend BILASPUR NIHAL SINGH WALA BILASPUR Amount for unclaimed and JASVIR KAUR JAGROOP SINGH INDIA PUNJAB 142039 0000063 40.00 02-Nov-2025 142039 MOG, A PUNJAB, unpaid dividend GHANDA BANnA RAMPURA PHUL Amount for unclaimed and JARNAIL SINGH MAHINDAR SINGH GHANDA BANA 151106, BATHINDA INDIA PUNJAB 151106 0000068 40.00 02-Nov-2025 unpaid dividend PUNJAB, MAJHI,BHAWANIGARH, MAJHI, Amount for unclaimed and SINDER KAUR SATGUR SINGH INDIA PUNJAB 148026 0000116 40.00 02-Nov-2025 SANGRUR unpaid dividend MAJHI BHAWANIGARH MAJHI Amount for unclaimed and SAROJ RANI KARAMJIT SINGH INDIA PUNJAB 148026 0000117 40.00 02-Nov-2025 -
1 Proceedings of the 155Thmeeting of State Environment Impact
Proceedings of the 155thmeeting of State Environment Impact Assessment Authority held on14.11.2019 at 11:00 AM in the Conference Hall No 3 (Ist Floor), Punjab State Council for Science and Technology, MGSIPA Complex, Sector-26, Chandigarh. The following were present: 1) Sh. Kuldip Singh, IFS (Retd.), Chairman, SEIAA 2) Sh. Charandeep Singh, PCS Member Secretary, SEIAA At the outset, the Member Secretary, SEIAA welcomed the Chairman of the State Environment Impact Assessment Authority (SEIAA) in its 155thmeeting. Item No.01: Confirmation of the minutes of 154th meeting of SEIAA held on 22.10.2019. SEIAA was apprised that the proceedings of 154th meeting of SEIAA held on 22.10.2019 has been circulated to all concerned vide email dated 04.11.2019. The said proceedings were not uploaded on Punjab State portal of MoEF&CC being only offline items of the agenda of the said meeting. No observation was received from any of the members. SEIAA confirmed the minutes of the said meeting. Item No.02: Action on the proceedings of 153rd and 154th meeting of SEIAA held on 17.10.2019 and 22.10.2019, respectively. SEIAA was apprised that the action on the proceedings of 153rd and 154thmeeting of SEIAA held on 17.10.2019 and 22.10.2019 respectively was being taken and the action taken report would be placed in the next meeting of SEIAA.SEIAA asked to take the action on said proceedings without any further delay. Item No.155.01: Application for obtaining Environmental clearance under EIA notification dated 14.09.2006 for establishment of 18 MW Biomass based Power Plant located in revenue estate of Village Sedha Singh Wala, Tehsil Jaito, District Faridkot by M/s Sukhbir Agro Energy Ltd. -

Guru Har Sahai Block Firozpur District
GURU HAR SAHAI BLOCK M A M D O T B L O C K FIROZPUR DISTRICT BAHADUR KE CHAK SARKAR 301 MEGA BORDER VILLAGES MAP BAHADARKE MEHTAM CHAK SOMIAN KOAR 306 326 WALA SINGH WALA CHAK CHHANGA 239 238 CHAK MEGHA DONA MAHTAM BAHADAR KE MAHANTAN 308 CHAK JAMIAT 307 CHHANGA 325 BAJA KE SINGH WALA RAI HITHAR 300 309 237 MARE ® BOOLA MAHTAM CHHANGA KALAN N DONA HITHAR MAHATAM 0 1.5 3 6 A PINDI 166 F T KHUNG KE 310 298 312 BOOLA MAHTAM 169 A S MARE I MEGHA PANJ UTTAR NAUNARI VIRAK Kilometers K KHURD R DONA GRAIN HITHAR 297 KHOKHER UTTAR WASAL KHURD A DONA GUDAR 167 I P BHADRU 311 MEGHA PANJ 299 MOHAN KE 165 PANJ GRAIN D 318 314 PANJE GRAIN UTTAR 170 GUDDAR KE HITHAR 295 MOHAN K HAJI KE HITHAR PANJ GRAIN 316 MOHAN KE O RANA ISSA PANJ BETTU 172 317 PANJE UTTAR GRAIAN 296 MANDI T KE UTTAR 168 320 SAIDO WALA CHUGA 294 KE MOHAN 171 164 D 173 GURU ISSA NAUBRAMAD SHER SINGH CHAK HAR SAHAI I PANJ GRAIN RUKNA QUTAB SHER SINGH WAL WALA PANJE KE 162 S 287 BODLA GARH BAGUWALA 327 326 SWAYA 288 JIWAN T SWAYA MATTAM UTTAR 293 ARAIN 174 NIDHANA 163 MAHTAM HITHAR RAHIM SHAH R N 286 TILU 292 175 A GATI AJAIB 322 NURE KEBODLA I BILLIMAR ARAIN CHAK T SINGH WALA 285 276 C 324 289 NIDHANA S 331 SHEKH T I KHERE KHERE 177 SHATIA K KE HITHAR SHAMAN PIR KE KE UTTAR KUTTI WALA A BALE 325 277 MALIK THETHERAN 155 HITHAR DULLE KE 284 SULLAH 176 P KE UTTAR TRIPAL KE ZADA WALA 341 NATH WALA GHULLAH 279 337 BADAL THARA SINGH 290 291 182 MEHMOOD KHANEKE 330 280 KE HITHAR WALA HITHAR BHURAN PIRKE 342 BAME 333 335 MAHANTAN MOTHANWALA WALA BHATTI BODLA DULE KE BADAL KE GURU HAR SAHAI