Equivalence of Cell Survival Data for Radiation Dose and Thermal
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

In0000721 Redistribution of Thermal X-Ray Radiation In
IN0000721 BARC/1999/E/043 CO > O CO to m o>»» REDISTRIBUTION OF THERMAL X-RAY RADIATION IN CAVITIES: VIEW-FACTOR METHOD AND COMPARISON WITH DSN CALCULATIONS by M.K. Srivastava Theoretical Physics Division and Vinod Kumar and S.V.G. Menon Solid State & Spectroscopy Group 31/30 1999 BARC/1999/E/043 GOVERNMENT OF INDIA ATOMIC ENERGY COMMISSION REDISTRIBUTION OF THERMAL X-RAY RADIATION IN CAVITIES: VIEW-FACTOR METHOD AND COMPARISON WITH DSN CALCULATIONS by M.K. Srivastava Theoretical Physics Division and Vinod Kumar and S.V.G. Menon Solid State & Spectroscopy Group BHABHA ATOMIC RESEARCH CENTRE MUMBAI, INDIA 1999 BARC/199S/E/043 BIBLIOGRAPHIC DESCRIPTION SHEET FOR TECHNICAL REPORT (as per IS : 9400 -1980) 01 Security classification: Unclassified 02 Distribution: External 03 Report status: New 04 Series : BARC External 05 Report type: Technical Report 06 Report No.: BARC/1999/E/043 07 Part No. or Volume No.: 08 Contract No.: 10 Title and subtitle: Redistribution of thermal x-ray radiation in cavities: view factor method and comparison with DSN calculations 11 Collation: 39 p., 9 figs. 13 Project No. : 20 Personal authors): 1) M.K. Srivastava 2) Vinod Kumar, S.V.G. Menon 21 Affiliation of authors): 1) Theoretical Physics Division, Bhabha Atomic Research Centre, Mumbai 2) Solid State and Spectroscopy Group, Bhabha Atomic Research Centre, Mumbai 22 Corporate authors): Bhabha Atomic Research Centre, Mumbai - 400 085 23 Originating unit: Theoretical Physics Division, BARC, Mumbai 24 Sponsors) Name: Department of Atomic Energy Type: Government Contd... (ii) -l- 30 Date of submission: December 1999 31 Publication/Issuedate: January 2000 40 Publisher/Distributor: Head, Library and Information Services Division, Bhabha Atomic Research Centre, Mumbai 42 Form of distribution: Hard copy 50 Language of text: English 51 Language ofsummary: English 52 No. -

Chapter 3 the Mechanisms of Electromagnetic Emissions
BASICS OF RADIO ASTRONOMY Chapter 3 The Mechanisms of Electromagnetic Emissions Objectives: Upon completion of this chapter, you will be able to describe the difference between thermal and non-thermal radiation and give some examples of each. You will be able to distinguish between thermal and non-thermal radiation curves. You will be able to describe the significance of the 21-cm hydrogen line in radio astronomy. If the material in this chapter is unfamiliar to you, do not be discouraged if you don’t understand everything the first time through. Some of these concepts are a little complicated and few non- scientists have much awareness of them. However, having some familiarity with them will make your radio astronomy activities much more interesting and meaningful. What causes electromagnetic radiation to be emitted at different frequencies? Fortunately for us, these frequency differences, along with a few other properties we can observe, give us a lot of information about the source of the radiation, as well as the media through which it has traveled. Electromagnetic radiation is produced by either thermal mechanisms or non-thermal mechanisms. Examples of thermal radiation include • Continuous spectrum emissions related to the temperature of the object or material. • Specific frequency emissions from neutral hydrogen and other atoms and mol- ecules. Examples of non-thermal mechanisms include • Emissions due to synchrotron radiation. • Amplified emissions due to astrophysical masers. Thermal Radiation Did you know that any object that contains any heat energy at all emits radiation? When you’re camping, if you put a large rock in your campfire for a while, then pull it out, the rock will emit the energy it has absorbed as radiation, which you can feel as heat if you hold your hand a few inches away. -

Personal Preparedness Guide Radiological: Nuclear Explosion
PERSONAL PREPAREDNESS GUIDE RADIOLOGICAL: NUCLEAR EXPLOSION What It Is: Nuclear explosions occur when two subcritical masses of highly processed radioactive material are thrust together suddenly, triggering a violent chain reaction and release of energy. Nuclear weapons are designed to cause catastrophic damage to people, buildings and the environment. Special highly guarded materials and expertise are required to construct and detonate a nuclear weapon. Damage from nuclear weapons fall into several categories. The explosion itself can demolish buildings and structures over a large area. The extent of the damage depends on the power of the bomb. Once the bomb explodes, it releases a fireball. This form of radiation can melt and burn some objects and skin, but clothing and opaque objects can provide some protection. However, the heat from thermal radiation is also the source of most of the post-blast fires. The intense heat of the fire causes an updraft, pulling oxygen in, making it difficult to breathe in the surrounding area. One of the unique effects of a nuclear blast is the electromagnetic pulse, which also emanates from the center of the blast. It disables all electrical devices in its path, rendering anything with a computer chip essentially dead. This poses an escape problem; newer cars with chips would not be able to start. Perhaps the most widely known effect of a nuclear attack is the fallout. When the bomb or missile explodes near the earth's surface, it pulls soil and water into a mushroom cloud, contaminating it with radiation. This matter settles back to the ground generally within a day and can be spread over a wider area by wind. -

Advanced Waste Heat Recovery Technology by Thermo-Rradiative
Nuclear and Emerging Technologies for Space Knoxville, TN, April 6 – April 9, 2020, available online at https://nets2020.ornl.gov ADVANCED WASTE HEAT RECOVERY TECHNOLOGY BY THERMO-RADIATIVE CELL FOR NUCLEAR SPACE POWER APPLICATIONS Jianjian Wang1*, Chien-Hua Chen1, Richard Bonner1, and William G. Anderson1 1Advanced Cooling Technologies, Inc., Lancaster, PA 17603 *[email protected] 717-490-2387 In order to satisfy the long-lasting and high However, the bulk production of Pu-238 in the US energy/power density requirements for NASA deep space was stopped in 1988. Although DOE is expected to be exploration missions, Pu-238 has been identified as one able to produce 1.5 kg Pu-238 per year by 2026 for of the most suitable radioisotope fuels for GPHS modules NASA, there are still many uncertainties, and DOE is since the 1960s. The availability of Pu-238 is currently facing many challenges to meet this production goal. In extremely limited. The limited availability suggests that addition, due to the highly technical nature of the Pu-238 efficiently using the heat generated by the GPHS is very production process and the long time required (~2 years) important and critical for NASA space applications. for technical staff training, the unit price of Pu-238 is very However, the efficiency of the most widely used high, ~$8 million per kilogram [2,3]. NASA’s budget can radioisotope thermoelectric generators is only about 6- only support one radioisotope power system (RPS) 8%, which means that a significant amount of energy is mission every 4 years [3]. -

Nuclear and Space Radiation Effects on Materials
RIV000151 Date Submitted: June 9, 2015 CASE FILE NASA coe.x NASA SP -8053 SPACE VEHICLE United States Nuclear Regulatory Commission Official Hearing Exhibit In the Matter of: Entergy Nuclear Operations, Inc. (Indian Point Nuclear Generating Units 2 and 3) DESIGN CRITERIA ASLBP #: 07-858-03-LR-BD01 Docket #: 05000247 | 05000286 Exhibit #: RIV000151-00-BD01 Identified: 11/5/2015 (STRUCTURES) Admitted: 11/5/2015 Withdrawn: Rejected: Stricken: Other: NUCLEAR AND SPACE RADIATION EFFECTS ON MATERIALS JUNE 1970 NATIONAL AERONAUTICS AND SPACE ADMINISTRATION FOREWORD NASA experience has indicated a need for uniform criteria for the design of space vehicles. Accordingly, criteria are being developed in the following areas of technology: Environment Structures Guidance and Con trol Chemical Propulsion Individual components of this work will be issued as separate monographs as soon as they are completed. A list of all previously issued monographs in this series can be found at the end of this document. These monographs are to be regarded as guides to design and not as NASA requirements, except as may be specified in formal project specifications. It is expected, however, that the criteria sections of these documents, revised as experience may indicate to be desirable, eventually will become uniform design requirements for NASA space vehicles. This monograph was prepared under the cognizance of the Langley Research Center. The Task Manager was T. L. Coleman. The authors were H. Shulman of Teledyne Isotopes and W. S. Ginell of McDonnell Douglas Corporation. A number of other individuals assisted in developing the material and reviewing the drafts. In particular, the significant contributions made by J. -

Spatio-Temporal Radiation Biology: New Insights and Biomedical Perspectives
Citation: Cell Death and Disease (2010) 1, e4; doi:10.1038/cddis.2009.5 & 2010 Macmillan Publishers Limited All rights reserved 1350-9047/10 $32.00 www.nature.com/cdd Meeting Report Spatio-temporal radiation biology: new insights and biomedical perspectives Cell Death and Disease (2010) 1, e4; doi:10.1038/cddis.2009.5; published online 14 January 2010 Subject Category: Experimental Medicine The ESF-EMBO Symposium Spatio-Temporal Radiation Biology: Transdisciplinary Advances for Biomedical Applications, 16–21 May 2009 Sant Feliu de Guixols, Spanish Costa Brava This is an open-access article distributed under the terms of the Creative CommonsAttribution License, which permits distribution and reproduction in any medium, provided the original author and source are credited. This license does not permit commercial exploitation without specific permission. The ESF-EMBO Symposium Spatio-Temporal Radiation pathways. Two models, including the budding yeast Biology: Transdisciplinary Advances for Biomedical Applica- Saccharomyces cerevisiae and DT40 chicken B-lymphocytic tions, 16–21 May 2009 was held in Sant Feliu de Guixols, cells, show how the DDR is crucial for each cell and allow the 120 km from Barcelona, the capital city of Catalunya, Spanish dissection of the involvement of each protein that participates Costa Brava. This 4-day conference created a timely forum for in similar functions in such distant species. Marie-Pierre multidisciplinary discussions of recent researches on ionizing Gaigeot (Evry University, Evry, France) discussed semi- radiation effects in living organisms, from molecular to tissue quantum simulations of primary radiation effects, considering scales. The symposium brought together 95 participants from the direct DNA damage dynamics and indirect effects 21 countries worldwide, such as physicists, chemists, with water molecules. -

Thermal Radio Emission
AN EFFECT OF STIMULATED EADIATION PROCESSES ON RADIO EMISSION FROM EXTENDED SOURCES Fedor V.Prigara Institute of Microelectronics and Informatics, Russian Academy of Sciences, 21 Universitetskaya, 150007 Yaroslavl, Russia; [email protected] ABSTRACT Both the standard theory of thermal radio emission and the synchrotron theory encounter some difficulties. The most crucial for the former one is nonpossibility to explain the radio spectrum of Venus in the decimeter range (Ksanfomality 1985). The radio spectra of planetary nebulae at high frequencies also are not comfortably consistent with the standard theory (Siodmiak & Tylenda 2001). Here we show that the account for an induced character of radiation processes sufficiently improves the predictions of the standard theory. Moreover, the developed here theory of radio emission from non-uniform gas gives the radio spectra of extended sources, such as supernova remnants and radio galaxies, which are normally attributed to the synchrotron emission. It is important, in this aspect, that the synchrotron self-absorption produces a change in the polarization position angle across the spectral peak. No such a change was detected in gigahertz-peaked spectrum sources (Mutoh et al. 2002). Besides, the flat or slightly inverted radio spectra of low-luminosity active galactic nuclei are not easily consistent with the synchrotron radiation mechanism (Nagar, Wilson & Falcke 2001, Ulvestad & Ho 2001). Thermal radiation in a magnetic field is polarized (see, e.g., Lang 1978). This is also true for radiation considered in the present paper, which can be described as incoherent induced radiation (Prigara 2001b). Subject headings: radiation mechanisms: thermal - radio continuum: general 1. INTRODUCTION In this paper the thermal radio emission from non-uniform gas is considered. -

Radiological Injuries
Radiological Injuries Chapter 30 Radiological Injuries The reader is strongly advised to supplement material in this chapter with the following two references: 1. Medical Management of Radiological Casualties Handbook, 2003, Armed Forces Radiobiology Research Institute, Bethesda, MD. 2. Medical Management of the Acute Radiation Syndrome: Recommendations of the Strategic National Stockpile. Radiation Working Group, Strategic National Stockpile (Annals of Internal Medicine, 15 June 2004). Introduction Radiological casualties on the battlefield may occur with improvised or conventional nuclear devices or radiological dispersal devices (“dirty bombs”) (Table 30-1). Conventional nuclear weapons. ο The relative casualty-causing potential depends primarily on four factors: ♦ Yield of the weapon. ♦ Height of burst. ♦ Environmental conditions in which the detonation occurs. ♦ Distribution and shielding of troops in the target area. ο A nuclear detonation generally causes injuries with the following distribution: ♦ Blast injury: 50%. ♦ Thermal injury: 35%. ♦ Ionizing radiation injury. ◊ Initial: 5%. ◊ Residual: 10%. 30.1 Emergency War Surgery A radiological dispersal device (RDD) is any device, including any weapon or equipment, other than a nuclear explosive device, specifically designed to spread radiation. ο RDDs contaminate conventional casualties with radionuc- lides, complicating medical evacuation. ο RDDs are ideal weapons for terrorism and are used to intimidate and deny access to an area by spreading radioactive material. Table 30-1. Radiological casualties. Weapon Effect Weapon Yield (Kiloton)/Distance (Meters) 1 kt 10 kt 100 kt 1,000 kt Blast (50% casualties) 140 m 360 m 860 m 3,100 m Thermal radiation 370 m 1,100 m 3,190 m 8,020 m (50% deep burns) Ionizing radiation 600 m 950 m 1,400 m 2,900 m (50% immediate transient ineffectiveness) Ionizing radiation 800 m 1,100 m 1,600 m 3,200 m (50% lethality) Triage Different from conventionally injured patients, because survivable radiation injury is not manifested until days to weeks after exposure. -

Effect of Thermal Radiation on the Laminar Free Convection from a Heated Vertical Plate
ht. J. Hear Muss Tramfer. Vol. I I, pp. 871481. Pergamon Press 1968. Priinted in Great Britain EFFECT OF THERMAL RADIATION ON THE LAMINAR FREE CONVECTION FROM A HEATED VERTICAL PLATE VEDAT S. ARPACI University of Michigan, Ann Arbor, Michigan 48104, U.S.A. (Received 3 1 August 1967 and in revised form 15 November 1967) Abstract-An analytical attempt is made to understand the non-equilibrium interaction between thermal radiation and laminar free convection in terms of a heated vertical plate in a stagnant radiating gas. The effect of radiation is taken into account in the integral formulation of the problem as a one-dimensional heat flux, evaluated by including the absorption in thin gas approximation and the wall elfect in thick gas approximation. The local Nusselt numbers thus obtained help to interpret the gas domains from transparent to opaque and from cold to hot. The present thick gas model approximates the radiant flux as qR=-E[- (I-?)exp(-$aygT’$ whose limit for large a and small but non-zero y is the Rosseland gas, qgs = - (16a/3a) T3(cW/ay), and that for y = 0 and large but finite a is 4”, = - c,(8a/3a) T$W/ay),. NOMENCLATURE coefficient of thermal expansion ; thermal diffusivity, k/pep; local dimensionless number, B../(G,/ Bouguer number, a6 ; 4Y ; local Bouguer number, ax ; boundary-layer thickness ; specific heat at constant pressure ; diffuse emissivity of plate wall ; integro-exponential function of order dimensionless variable, 1 - l; n; dimensionless variable, cry ; gravitational acceleration ; temperature ratio, (T, - TJT, ; local Grashof number, gj3p2(Tw - T,) viscosity ; x3/$; kinematic viscosity ; heat-transfer coefficient ; dimensionless variable, q/B; thermal conductivity ; density ; local Nusselt number, hx/k ; diffuse reflectivity of plate wall ; Prandtl number, V/U= ,uc,/k ; Stefan-Boltzmann constant ; ambient Planck number, akT,/4a-. -
Radiological Injuries
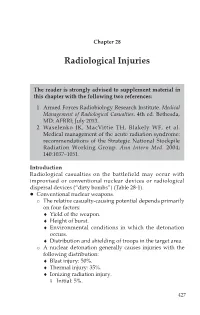
Radiological Injuries Chapter 28 Radiological Injuries The reader is strongly advised to supplement material in this chapter with the following two references: 1. Armed Forces Radiobiology Research Institute. Medical Management of Radiological Casualties. 4th ed. Bethesda, MD: AFRRI; July 2013. 2. Waselenko JK, MacVittie TH, Blakely WF, et al. Medical management of the acute radiation syndrome: recommendations of the Strategic National Stockpile Radiation Working Group. Ann Intern Med. 2004; 140:1037–1051. Introduction Radiological casualties on the battlefield may occur with improvised or conventional nuclear devices or radiological dispersal devices (“dirty bombs”) (Table 28-1). Conventional nuclear weapons. o The relative casualty-causing potential depends primarily on four factors: ♦ Yield of the weapon. ♦ Height of burst. ♦ Environmental conditions in which the detonation occurs. ♦ Distribution and shielding of troops in the target area. o A nuclear detonation generally causes injuries with the following distribution: ♦ Blast injury: 50%. ♦ Thermal injury: 35%. ♦ Ionizing radiation injury. ◊ Initial: 5%. 427 Emergency War Surgery ◊ Residual: 10%. A radiological dispersal device (RDD) is any device— including any weapon or equipment—other than a nuclear explosive device, specifically designed to spread radiation. o RDDs contaminate conventional casualties with radionuclides, complicating medical evacuation. o RDDs are ideal weapons for terrorism, and are used to intimidate and deny access to an area by spreading radioactive material. Table 28-1. Radiological Casualties Weapon Effect Weapon Yield (kt)/Distance (m) 1 kt 10 kt 100 kt 1,000 kt Blast 140 m 360 m 860 m 3,100 m (50% casualties) Thermal radiation 370 m 1,100 m 3,190 m 8,020 m (50% deep burns) Ionizing radiation 600 m 950 m 1,400 m 2,900 m (50% immediate transient ineffectiveness) Ionizing radiation 800 m 1,100 m 1,600 m 3,200 m (50% lethality) kt: kiloton; m: meter. -

Radiation Spectrum (Ionizing and Non-Ionizing)
RADIATION SPECTRUM The electromagnetic spectrum is the range of frequencies (the spectrum) of electromagnetic radiation and their respective wavelengths and photon energies. The electromagnetic spectrum covers electromagnetic waves with frequencies ranging from below one hertz to above 1025 hertz, corresponding to wavelengths from thousands of kilometers down to a fraction of the size of an atomic nucleus. This frequency range is divided into separate bands, and the electromagnetic waves within each frequency band are called by different names; beginning at the low frequency (long wavelength) end of the spectrum these are: radio waves, microwaves, infrared, visible light, ultraviolet, X-rays, and gamma rays at the high-frequency (short wavelength) end. The electromagnetic waves in each of these bands have different characteristics, such as how they are produced, how they interact with matter, and their practical applications. The limit for long wavelengths is the size of the universe itself, while it is thought that the short wavelength limit is in the vicinity of the Planck length. Gamma rays, X- rays, and high ultraviolet are classified as ionizing radiation as their photons have enough energy to ionize atoms, causing chemical reactions. Exposure to these rays can be a health hazard, causing radiation sickness, DNA damage and cancer. Radiation of visible light wavelengths and lower are called nonionizing radiation as they cannot cause these effects. In most of the frequency bands above, a technique called spectroscopy can be used to physically separate waves of different frequencies, producing a spectrum showing the constituent frequencies. Spectroscopy is used to study the interactions of electromagnetic waves with matter. -
Radiological Emergency Management Glossary
Glossary RADIOLOGICAL EMERGENCY MANAGEMENT GLOSSARY Acute Exposure: Radiation exposure of short duration. ALARA: Acronym for keeping radiation exposure "As Low As Reasonably Achievable." Radioactive material users apply this concept in minimizing occupational and public exposure. Alpha Particle: A positively charged particle ejected spontaneously from the nuclei of some radioactive elements. It is equal in mass and charge to a helium nucleus and has low penetrating power and short range. The most energetic alpha particle from radioactive decay will generally fail to penetrate the skin. Alphas are hazardous when an alpha-emitting nuclide is introduced into the body. Atom: The smallest particle of an element that cannot be divided or broken up by chemical means. It consists of a central core called the nucleus which contains protons and neutrons. Electrons revolve in orbits in the region surrounding the nucleus. Becquerel (Bq): The radioactivity unit of the international system of units. One becquerel equals one nuclear disintegration per second. Beta Particle: A charged particle emitted from a nucleus during radioactive decay. The beta particle, with a mass equal to 1/1837 that of a proton, is similar to an electron. Large amounts of beta radiation may cause skin burns, and beta emitters are harmful if they enter the body. Beta particles from radioactive decay are easily stopped by a thin sheet of metal or plastic. Blast Effect: A pulse of air in which the pressure increases sharply at the front, accompanied by winds, propagated from an explosion. Boiling Water Reactor (BWR): A type of reactor system which allows water to boil directly in the reactor core to produce steam for the turbine generator.