The Relationship Between Chitotriosidase Activity and Tuberculosis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Analysis on the Spatial Form of Traditional Kiln Houses in Hongjiang Ancient Commercial City in Xiangxi
Analysis on the Spatial Form of Traditional Kiln Houses in Hongjiang Ancient Commercial City in Xiangxi Chenglin He*, Jie Zhang School of Art Design and Media, East China University of Science and Technology, Shanghai 200237, China Email: [email protected] Abstract: The ancient commercial city in Hongjiang, Huaihua has a long history and a strong national cultural atmo- sphere. It is famous for collecting and dispersing Hong oil, wood, and white vinegar. It has the reputation of "Little Nan- jing" and "Southwest Metropolis". As an important part of Hongjiang's ancient architecture, the kiln house building carries the regional culture of the ancient commercial city. This article focuses on the main body of the kiln house, and analyzes the characteristics of the scale, form, material, etc. through the spatial form of the streets and lanes of the building, the ap- pearance form of the building, the building structure and the detailed decoration characteristics. The kiln house constructs the unique style of the architecture in Xiangxi, combining practical functions with artistic aesthetics. This article focuses on the research of the kiln house, aiming to provide some reference for the future research and protection of traditional an- cient villages. Keywords: Hongjiang ancient commercial city, kiln house, spatial form, architectural decoration 1. Overview of the ancient commercial city Hongjiang ancient commercial city is located in Huaihua City, Hunan Province, at the junction of southXiangxi Province, Guizhou Province and Chongqing City, and is located in the Xuefeng Mountain area in the east of the Yunnan- Guizhou Plateau. According to historical records, the ancient city covers an area of approximately 300,000 square kilometers, bordering Qianyang County in the east and Huitong County in the south. -

Social Assessment Report
IPP574 v2 World Bank Loan Public Disclosure Authorized Hunan Forest Restoration and Development Project (HFRDP) Social Assessment Report Public Disclosure Authorized Public Disclosure Authorized Hunan Provincial Forest Foreign Fund Project Management Office Public Disclosure Authorized Social Assessment Team of HFRDP March, 2012 Social Assessment Report for Hunan Forest Restoration and Development Project Abbreviations CFB: County Forestry Bureau FC: Forest Cooperative HFRDP: Hunan Forest Restoration and Development Project HH: household HN: Hunan Province PCP: Participatory consultation and planning PFD: Provincial Forestry Department PPMO: Provincial Project Management Office PRA: Participatory Rural Appraisal SA: Social Assessment TFS: Township Forestry Station Social Assessment Report for Hunan Forest Restoration and Development Project ABSTRACT ................................................................................................................... 1 1. PROJECT BACKGROUND.................................................................................... 10 1.1 Project Background ........................................................................................ 10 1.2 Project Objectives .......................................................................................... 10 1.3 Project Components ....................................................................................... 10 2. PROCESS AND METHODS OF SA ...................................................................... 11 2.1 Process .......................................................................................................... -

Supplemental Information
Supplemental information Table S1 Sample information for the 36 Bactrocera minax populations and 8 Bactrocera tsuneonis populations used in this study Species Collection site Code Latitude Longitude Accession number B. minax Shimen County, Changde SM 29.6536°N 111.0646°E MK121987 - City, Hunan Province MK122016 Hongjiang County, HJ 27.2104°N 109.7884°E MK122052 - Huaihua City, Hunan MK122111 Province 27.2208°N 109.7694°E MK122112 - MK122144 Jingzhou Miao and Dong JZ 26.6774°N 109.7341°E MK122145 - Autonomous County, MK122174 Huaihua City, Hunan Province Mayang Miao MY 27.8036°N 109.8247°E MK122175 - Autonomous County, MK122204 Huaihua City, Hunan Province Luodian county, Qiannan LD 25.3426°N 106.6638°E MK124218 - Buyi and Miao MK124245 Autonomous Prefecture, Guizhou Province Dongkou County, DK 27.0806°N 110.7209°E MK122205 - Shaoyang City, Hunan MK122234 Province Shaodong County, SD 27.2478°N 111.8964°E MK122235 - Shaoyang City, Hunan MK122264 Province 27.2056°N 111.8245°E MK122265 - MK122284 Xinning County, XN 26.4652°N 110.7256°E MK122022 - Shaoyang City,Hunan MK122051 Province 26.5387°N 110.7586°E MK122285 - MK122298 Baojing County, Xiangxi BJ 28.6154°N 109.4081°E MK122299 - Tujia and Miao MK122328 Autonomous Prefecture, Hunan Province 28.2802°N 109.4581°E MK122329 - MK122358 Guzhang County, GZ 28.6171°N 109.9508°E MK122359 - Xiangxi Tujia and Miao MK122388 Autonomous Prefecture, Hunan Province Luxi County, Xiangxi LX 28.2341°N 110.0571°E MK122389 - Tujia and Miao MK122407 Autonomous Prefecture, Hunan Province Yongshun County, YS 29.0023°N -

Hunan Lingjintan Hydropower Project (Loan 1318-PRC) in the People’S Republic of China
Performance Evaluation Report PPE: PRC 26198 Hunan Lingjintan Hydropower Project (Loan 1318-PRC) in the People’s Republic of China December 2005 Operations Evaluation Department Asian Development Bank CURRENCY EQUIVALENTS Currency Unit – yuan (CNY) At Appraisal At Project Completion At Operations Evaluation (September 1994) (August 2003) (September 2005) CNY1.00 = $0.1149 = $0.1205 = $0.1238 $1.00 = CNY8.70 = CNY8.30 = CNY8.08 ABBREVIATIONS ADB – Asian Development Bank ADTA – advisory technical assistance BOO – build-operate-own BOT – build-operate-transfer EA – Executing Agency EIRR – economic internal rate of return FIRR – financial internal rate of return GWh – gigawatt-hour HEPC – Hunan Electric Power Company HPEPB – Hunan Province Electric Power Bureau IA – Implementing Agency MW – megawatt OED – Operations Evaluation Department, Asian Development Bank OEM – operations evaluation mission PCR – project completion report PPA – power purchase agreement PPTA – project preparatory technical assistance PRC – People’s Republic of China SES – special evaluation study SSTA – small-scale technical assistance TA – technical assistance WACC – weighted and average cost of capital WPC – Wuling Power Corporation NOTES (i) The fiscal year (FY) of the Government ends on 31 December. “FY” before a calendar year denotes the year in which the fiscal year ends. (ii) In this report, “$” refers to US dollars. Director D. Edwards, Operations Evaluation Division 2, OED Team Leader R. Schenck, Evaluation Specialist, Operations Evaluation Division 2, OED Team Members B. Palacios, Senior Evaluation Officer, Operations Evaluation Division 2, OED A. SIlverio, Operations Evaluation Assistant, Operations Evaluation Division 2,OED Operations Evaluation Department, PE-677 CONTENTS Page BASIC DATA iii EXECUTIVE SUMMARY iv MAP vii I. -

MIAMI UNIVERSITY the Graduate School Certification for Approving
MIAMI UNIVERSITY The Graduate School Certification for Approving the Dissertation We hereby approve the Dissertation of Stephen Hess Candidate for the Degree: Doctor of Philosophy ____________________________________ Director (Dr. Venelin Ganev) ____________________________________ Reader (Dr. Gulnaz Sharafutdinova) ____________________________________ Reader (Dr. Adeed Dawisha) ____________________________________ Graduate School Representative (Dr. Stanley Toops) ABSTRACT AUTHORITARIAN LANDSCAPES: STATE DECENTRALIZATION, POPULAR MOBILIZATION, AND THE INSTITUTIONAL SOURCES OF RESILIENCE IN NONDEMOCRACIES by Stephen Hess Beginning with the insight that highly-centralized state structures have historically provided a unifying target and fulcrum for the mobilization of contentious nationwide social movements, this dissertation investigates the hypothesis that decentralized state structures in authoritarian regimes impede the development of forms of popular contention sustained and coordinated on a national scale. As defined in this work, in a decentralized state, local officials assume greater discretionary control over public expenditures, authority over the implementation of government policies, and latitude in managing outbreaks of social unrest within their jurisdictions. As a result, they become the direct targets of most protests aimed at the state and the primary mediators of actions directed at third-party, non-state actors. A decentralized state therefore presents not one but a multitude of loci for protests, diminishing claimants‘ ability to use the central state as a unifying target and fulcrum for organizing national contentious movements. For this reason, decentralized autocracies are expected to face more fragmented popular oppositions and exhibit higher levels of durability than their more centralized counterparts. To examine this claim, I conduct four comparative case studies, organized into pairs of autocracies that share a common regime type but vary in terms of state decentralization. -
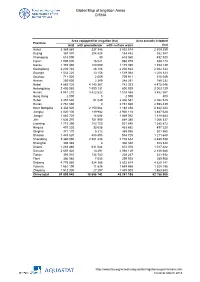
Global Map of Irrigation Areas CHINA
Global Map of Irrigation Areas CHINA Area equipped for irrigation (ha) Area actually irrigated Province total with groundwater with surface water (ha) Anhui 3 369 860 337 346 3 032 514 2 309 259 Beijing 367 870 204 428 163 442 352 387 Chongqing 618 090 30 618 060 432 520 Fujian 1 005 000 16 021 988 979 938 174 Gansu 1 355 480 180 090 1 175 390 1 153 139 Guangdong 2 230 740 28 106 2 202 634 2 042 344 Guangxi 1 532 220 13 156 1 519 064 1 208 323 Guizhou 711 920 2 009 709 911 515 049 Hainan 250 600 2 349 248 251 189 232 Hebei 4 885 720 4 143 367 742 353 4 475 046 Heilongjiang 2 400 060 1 599 131 800 929 2 003 129 Henan 4 941 210 3 422 622 1 518 588 3 862 567 Hong Kong 2 000 0 2 000 800 Hubei 2 457 630 51 049 2 406 581 2 082 525 Hunan 2 761 660 0 2 761 660 2 598 439 Inner Mongolia 3 332 520 2 150 064 1 182 456 2 842 223 Jiangsu 4 020 100 119 982 3 900 118 3 487 628 Jiangxi 1 883 720 14 688 1 869 032 1 818 684 Jilin 1 636 370 751 990 884 380 1 066 337 Liaoning 1 715 390 783 750 931 640 1 385 872 Ningxia 497 220 33 538 463 682 497 220 Qinghai 371 170 5 212 365 958 301 560 Shaanxi 1 443 620 488 895 954 725 1 211 648 Shandong 5 360 090 2 581 448 2 778 642 4 485 538 Shanghai 308 340 0 308 340 308 340 Shanxi 1 283 460 611 084 672 376 1 017 422 Sichuan 2 607 420 13 291 2 594 129 2 140 680 Tianjin 393 010 134 743 258 267 321 932 Tibet 306 980 7 055 299 925 289 908 Xinjiang 4 776 980 924 366 3 852 614 4 629 141 Yunnan 1 561 190 11 635 1 549 555 1 328 186 Zhejiang 1 512 300 27 297 1 485 003 1 463 653 China total 61 899 940 18 658 742 43 241 198 52 -

48443-002: Hunan Xiangjiang River
Resettlement Plan May 2018 People’s Republic of China: Hunan Xiangjiang River Watershed Existing Solid Waste Comprehensive Treatment Project --- Changning Subproject Prepared by The People’s Government of Changning for the Asian Development Bank. CURRENCY EQUIVALENTS (as of 30 April 2018) Currency unit – yuan (CNY) CNY1.00 = $0.15 8 $1.00 = CNY6.334 ABBREVIATIONS AAOV – average annual output value ADB – Asian Development Bank DI – design institute EA – executing agency FSR – feasibility study report HD – House demolition HPG – Hunan Provincial Government IA – implementing agency LA – land acquisition LAR – land acquisition and resettlement LRB – Land and Resources Administration Bureau RP – resettlement plan SES – social and economic survey SPS – ADB’s Safeguard Policy Statement (2009) WEIGHTS AND MEASURES m2 – square meter mu – 1 mu is equal to 666.7 m 2 km – kilometer NOTE In this report, "$" refers to United States dollars. This resettlement plan is a document of the borrower. The views expressed herein do not necessarily represent those of ADB's Board of Directors, Management, or staff, and may be preliminary in nature. Your attention is directed to the “terms of use” section of this website. In preparing any country program or strategy, financing any project, or by making any designation of or reference to a particular territory or geographic area in this document, the Asian Development Bank does not intend to make any judgments as to the legal or other status of any territory or area. Table of Contents EXECUTIVE SUMMARY ....................................................................................................................... -

Respiratory Healthcare Resource Allocation in Rural Hospitals in Hunan, China: a Cross-Sectional Survey
11 Original Article Page 1 of 10 Respiratory healthcare resource allocation in rural hospitals in Hunan, China: a cross-sectional survey Juan Jiang1, Ruoxi He1, Huiming Yin2, Shizhong Li3, Yuanyuan Li1, Yali Liu2, Fei Qiu2, Chengping Hu1 1Department of Respiratory Medicine, National Key Clinical Specialty, Xiangya Hospital, Central South University, Changsha 410008, China; 2Department of Respiratory and Critical Care Medicine, First Affiliated Hospital of Hunan University of Medicine, Huaihua 418099, China; 3Health Policy and Management Office of Health Commission in Hunan Province, Changsha 410008, China Contributions: (I) Conception and design: C Hu; (II) Administrative support: C Hu, H Yin, S Li; (III) Provision of study materials or patients: C Hu, J Jiang; (IV) Collection and assembly of data: J Jiang, R He, Y Li, Y Liu, F Qiu; (V) Data analysis and interpretation: C Hu, J Jiang; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Chengping Hu, MD, PhD. #87 Xiangya Road, Kaifu District, Changsha 410008, China. Email: [email protected]. Background: Rural hospitals in China provide respiratory health services for about 600 million people, but the current situation of respiratory healthcare resource allocation in rural hospitals has never been reported. Methods: In the present study, we designed a survey questionnaire, and collected information from 48 rural hospitals in Hunan Province, focusing on their respiratory medicine specialty (RMS), basic facilities and equipment, clinical staffing and available medical techniques. Results: The results showed that 58.3% of rural hospitals established an independent department of respiratory medicine, 50% provided specialized outpatient service, and 12.5% had an independent respiratory intensive care unit (RICU). -

Resettlement Plan: Zixing Subproject
Resettlement Plan May 2018 People’s Republic of China: Hunan Xiangjiang River Watershed Existing Solid Waste Comprehensive Treatment Project --- Zixing Subproject Prepared by the People’s Government of Zixing City for the Asian Development Bank. CURRENCY EQUIVALENTS (as of 30 April 2018) Currency unit – yuan (CNY) CNY1.00 = $0.15 8 $1.00 = CNY6.334 ABBREVIATIONS AAOV – average annual output value ADB – Asian Development Bank DI – design institute EA – executing agency FS R – feasibility study report HD – House demolition IA – implementing agency LA – land acquisition LAR – land acquisition and resettlement LRB – Land and Resources Admi nistration Bureau NDRC – National Development and Reform Commission RP – resettlement plan SES – social and economic survey SPS – ADB’s Safeguard Policy Statement (2009) WEIGHTS AND MEASURES m2 – square meter mu – equal to 666.7 m 2 km – kilometer NOTE In this report, "$" refers to United States dollars. This resettlement plan is a document of the borrower. The views expressed herein do not necessarily represent those of ADB's Board of Directors, Management, or staff, and may be preliminary in nature. Your attention is directed to the “terms of use” section of this website. In preparing any country program or strategy, financing any project, or by making any designation of or reference to a particular territory or geographic area in this document, the Asian Development Bank does not intend to make any judgments as to the legal or other status of any territory or area. Table of Contents EXECUTIVE SUMMARY ............................................................................................. I 1. PROJECT OVERVIEW .................................................................................... 1 1.1. PROJECT BACKGROUND ............................................................................. 1 1.2 PROJECT IMPACT SCOPE AND LOCATION ............................................... -

Chinese Bankers Survey 2016
www.pwchk.com Chinese Bankers Survey 2016 Executive summary February 2017 Preface We are pleased to present the Chinese Bankers Most bankers in the survey believe that the top Survey 2016 report, prepared jointly by the China priority in addressing risk is "to improve cash Banking Association (CBA) and PwC. Now in its collection, accelerate write-offs and disposal of eighth year, the report keeps track of developments collaterals". While increasing NPL disposal efforts in China’s banking sector from the perspective of a through conventional means such as write-offs, group of bankers. collections and transfers, Chinese banks are also actively exploring a diversified range of alternatives, This year’s survey dug deep into the core issues including NPL securitisation, cooperating with the while maintaining a broad scope. Dr. BA Shusong, big four asset management companies (AMCs), and the project leader, together with the project team, transfer of income beneficial rights. There is a interviewed 15 senior bankers to get their insights section in this report summarising bankers’ views into the sector. Seven of the 15 bankers are at C- on the major challenges regarding disposal of NPLs. suite level (director, vice president or above). These interviews complemented the online survey With China’s economic structural reform at a critical covering 31 provinces in mainland China (excluding juncture, Chinese banks are expected to play a more Hong Kong, Macau and Taiwan). With a total of active role in fulfilling social responsibilities by 1,794 valid responses collected, the survey sampling serving the real economy. With regard to economic process has taken into account participants’ restructuring, most bankers believe that “upgrading geographical regions, grades, types of financial and transforming manufacturing sector, and institution, and if the institution is listed on stock exploration of new markets" brings many exchange(s) or privately held. -

Congressional-Executive Commission on China Annual Report 2012
CONGRESSIONAL-EXECUTIVE COMMISSION ON CHINA ANNUAL REPORT 2012 ONE HUNDRED TWELFTH CONGRESS SECOND SESSION OCTOBER 10, 2012 Printed for the use of the Congressional-Executive Commission on China ( Available via the World Wide Web: http://www.cecc.gov 2012 ANNUAL REPORT CONGRESSIONAL-EXECUTIVE COMMISSION ON CHINA ANNUAL REPORT 2012 ONE HUNDRED TWELFTH CONGRESS SECOND SESSION OCTOBER 10, 2012 Printed for the use of the Congressional-Executive Commission on China ( Available via the World Wide Web: http://www.cecc.gov U.S. GOVERNMENT PRINTING OFFICE 76–190 PDF WASHINGTON : 2012 For sale by the Superintendent of Documents, U.S. Government Printing Office Internet: bookstore.gpo.gov Phone: toll free (866) 512–1800; DC area (202) 512–1800 Fax: (202) 512–2104 Mail: Stop IDCC, Washington, DC 20402–0001 CONGRESSIONAL-EXECUTIVE COMMISSION ON CHINA LEGISLATIVE BRANCH COMMISSIONERS House Senate CHRISTOPHER H. SMITH, New Jersey, SHERROD BROWN, Ohio, Cochairman Chairman MAX BAUCUS, Montana FRANK WOLF, Virginia CARL LEVIN, Michigan DONALD A. MANZULLO, Illinois DIANNE FEINSTEIN, California EDWARD R. ROYCE, California JEFF MERKLEY, Oregon TIMOTHY J. WALZ, Minnesota SUSAN COLLINS, Maine MARCY KAPTUR, Ohio JAMES RISCH, Idaho MICHAEL M. HONDA, California EXECUTIVE BRANCH COMMISSIONERS SETH D. HARRIS, Department of Labor MARIA OTERO, Department of State FRANCISCO J. SANCHEZ, Department of Commerce KURT M. CAMPBELL, Department of State NISHA DESAI BISWAL, U.S. Agency for International Development PAUL B. PROTIC, Staff Director LAWRENCE T. LIU, Deputy Staff -

Resource-Based City Type and Reforming Strategy Discussion and Research
2016 4th International Conference on Advances in Social Science, Humanities, and Management (ASSHM 2016) ISBN: 978-1-60595-412-7 Resource-based City Type and Reforming Strategy Discussion and Research Junwei Xing1 Abstract The resource-based city can divides according to the Israeli resource type and development phase two big standards. The resource-based city economic transformation strategy first should from the macroscopic level, seek for the regional economic development the new superiority, next should act according to the new regional development favorable condition that establishes the pattern of industrial transformation from the microscopic level. Keywords. Resource-based City; Type; Reforming Strategy. 1. INTRODUCTION The resource-based city is our country important foundation energy and raw material supplying place, development display excessively significant role to our country national economy. But as a result of the non-renewability of finiteness and resources of resource, the resource-based city sooner or later must face the issue of economic transformation, otherwise possibly enters the winter. At present, a considerable number of resource-based cities in China have been facing a series of economic and social problems such as resource depletion, economic recession, environmental degradation, unemployment and the increase of the poor population. These resource-based cities have become the problem areas in which regional contradictions are concentrated. Therefore, how to guide these cities to successfully transform and achieve sustainable development has become an important topic of concern for both academia and government. 2. Classification of Resource-based Cities Resource based cities are mainly built up by the development of resources. Although the overall pattern of urban growth and development is similar, because of the differences of the economic development factors such as natural resources, geographical conditions and other economic development factors, the difference between different resource cities is very large.