Cesarean Section by Larry C
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Moms Æ FLIP OVER for Atlanta Parent!
atlanta BABYFROM ATLANTA PARENT MAGAZINE Delivery Decisions Words of Wisdom for New Moms æ FLIP OVER for Atlanta Parent! Mom- Approved Obstetricians Feeding Help for Parents. Powered by Experts. Strong4Life.com By the age of 3, your baby will develop eating habits that can last a lifetime, so you’re smart to get a jump on your baby’s nutrition. It’s easy with Strong4Life.com—a unique parenting website from the experts you trust at Children’s Healthcare of Atlanta. At Strong4Life.com, you can: Ask an expert Sign up for Browse for who is a our monthly tips by age parent too e-newsletter ©2018 Children’s Healthcare of Atlanta Inc. All rights reserved. The Doctor’s Office to your Doorstep Moms-to-be: We Come to You! Are you tired of ... OB2me alleviates all of these and provides l fighting Atlanta traffic to get the luxury and convenience of bringing to the doctor’s office? quality prenatal care to your doorstep while l having to take time off from still delivering your baby at the hospital! work or finding childcare? l extended, unpredictable OB2me.com waiting room times? l minimal face to face time with your provider? l inconvenient appointment times? OB2me is a Division of 2me Healthcare, LLC atlanta BABYFROM ATLANTA PARENT MAGAZINE Guide for New and Expectant Parents 7 / Advice for New Moms 20 / Where Will You While many “words of wisdom” new mothers Have Your Baby? receive may sound clichéd, here are a few Use Atlanta truths that help with life in general, and Parent’s easy- parenthood in particular. -
November 28, 2018 – December 4, 2018 Requests for Extended Implementation/Performance Period
Use the links below for easy navigation Letters of Intent Letters of Intent - Expired Letters of Intent – Fall Batching New CON Applications CON Applications/Projects Withdrawn Pending/Complete Applications Pending Review/Incomplete CON Applications Office of Health Planning Recently Approved CON Applications Recently Denied CON Applications Appealed CON Projects Letters of Determination Requests for Miscellaneous Letters of Determination Appealed Determinations DET Review LNR Conversion CERTIFICATE OF NEED Requests for LNR for Diagnostic or Therapeutic Equipment Requests for LNR for Establishment of Physician-Owned Ambulatory Surgery Facilities Appealed LNRs November 28, 2018 – December 4, 2018 Requests for Extended Implementation/Performance Period Batching Notifications - Fall Need Projection Analyses Georgia Department of Community Health New Batching Review Office of Health Planning Summer Cycle Fall Cycle 2 Peachtree Street 5th Floor Non-Filed or Incomplete Surveys Atlanta, Georgia 30303-3159 Indigent-Charity Shortfalls (404) 656-0409 (404) 656-0442 Fax CON Filing Requirements (effective July 18, 2017) www.dch.georgia.gov Contact Information Verification of Lawful Presence within U.S. Periodic Reporting Requirements CON Thresholds Open Record Request Form Web Links Certificate of Need Appeal Panel www.GaMap2Care.info Letters of Intent LOI2018083 Doctors Hospital of Augusta Acquire a Fixed-Based MRI to Replace Existing Mobile MRI Received: 11/15/2018 Application must be submitted on: 12/17/2018 Site: 3651 Wheeler Road, Augusta, GA -

March 6, 2019 – March 12, 2019 Need Projection Analyses
Use the links below for easy navigation Letters of Intent Letters of Intent - Expired New CON Applications Pending/Complete Applications Pending Review/Incomplete CON Applications Office of Health Planning Recently Approved CON Applications Recently Denied CON Applications Appealed CON Projects Letters of Determination Requests for Miscellaneous Letters of Determination Appealed Determinations DET Review LNR Conversion Requests for LNR for Diagnostic or Therapeutic Equipment Requests for LNR for Establishment CERTIFICATE OF NEED of Physician-Owned Ambulatory Surgery Facilities Appealed LNRs Requests for Extended Implementation/Performance Period Batching Notifications - Fall March 6, 2019 – March 12, 2019 Need Projection Analyses New Batching Review Winter Cycle Fall Cycle Non-Filed or Incomplete Surveys Georgia Department of Community Health Office of Health Planning Indigent-Charity Shortfalls 2 Peachtree Street 5th Floor CON Filing Requirements (effective July 18, 2017) Atlanta, Georgia 30303-3159 Contact Information (404) 656-0409 (404) 656-0442 Fax Verification of Lawful Presence within U.S. www.dch.georgia.gov Periodic Reporting Requirements CON Thresholds Open Record Request Form Web Links Certificate of Need Appeal Panel www.GaMap2Care.info Letters of Intent LOI2019010 Tanner Imaging Center, Inc. Development of Freestanding Imaging Center on Tanner Medical Center-Carrollton Campus Received: 2/15/2019 Application must be submitted on: 3/18/2019 Site: 706 Dixie Street, Carrollton, GA 30117 (Carroll County) Estimated Cost: $2,200,000 -

Eugene H. Hirsh, M.D., F.A.C.P., F.A.C.G., A.G.A.F
Eugene H. Hirsh, M.D., F.A.C.P., F.A.C.G., A.G.A.F. Gastroenterology Consultants, PC Georgia Endoscopy 5669 Peachtree-Dunwoody Rd., Suite 270 Center, LLC Atlanta, Georgia 30342 3330 Preston Ridge Rd. (404) 255-1000 Fax: (404) 847-0416 Alpharetta, GA 30005 Endoscopy Consultants, LLC Suite 290 (770) 821-6800 (678) 399-2050 EDUCATION: Specialty Training: 1978-1980 Emory University Affiliated Hospitals, Division of Digestive Diseases John T. Galambos, M.D., Director, Theodore Hersh, M.D., Co-Director Training in Gastroenterology with inpatient and outpatient responsibilities at Emory University Hospital, Grady Memorial Hospital, and the Atlanta Veterans Administration Hospital Internship and Residency: 1975-1978 Emory University Affiliated Hospitals, 69 Butler Street, Atlanta, Georgia 30303 J. Willis Hurst, M.D., Chairman, Department of Medicine Medical School: 1971-1975 State University of New York at Buffalo, School of Medicine, Buffalo, New York Postgraduate: 1968-1971 - Teacher of Mathematics, New York City Board of Education Chairman, Faculty Council 1969-1971 College: 1964-1968, Cornell University, Ithaca, New York Bachelor of Science, Member, Cornell Society of Engineers American Society of Materials Engineers PROFESSIONAL EXPERIENCE: Medical Practice: Private practice – Gastroenterology Consultants, PC – 1980 to present. Teaching Appointments: Clinical Associate Professor of Medicine (Digestive Diseases) Emory University School of Medicine, 1983-present Board of Directors, Saint Joseph’s Hospital of Atlanta, 1999 – 2011 Board of Directors, St. Joseph’s Translational Research Institute with Georgia Tech University, 2008-present Fellow, American Gastroenterological Association, May 2007 Fellow, American College of Gastroenterology, 10/88 Fellow, American College of Physicians, 3/84 Diplomate, American Board of Internal Medicine, 1978 Board Certified in Gastroenterology 1981. -

HB 789 Surprise Bill Transparency Act Information
HB 789 Surprise Bill Transparency Act Information As part of the HB 789 Surprise Bill Transparency Act, Ambetter from Peach State Health Plan is providing consumers with the surprise bill rating for in-network hospital specialty groups. If a surprise bill rating is less than four checkmarks, each insurer advertising a hospital as in-network shall describe which qualified hospital based specialty group types are not contracted with the insurer. Please use the legend below to determine the rating for in-hospital specialty groups. Key Service Provided by In-Network Provider Service Provided by Out of Network Provider Service not offered at Facility Specialty Network Participation in Review To view a full listing of our in-network provider’s visit: https://guide.ambetterhealth.com/ NOTE: The information in this document was accurate when published. Since then, changes may have occurred that affect the information. Please call Member Services at 1-877-687-1180 or TTY/TDD 1-877-941-9231 for the most current provider information. 10/2020 This document is current as of the date listed below. A provider’s listing in the directory does not guarantee that the provider is still in the network or accepting new members. Ambetter from Peach State Health Plan 10/2020 TABLE OF CONTENTS / TABLA DE CONTENIDOS Page / Página Hospitals / Hospitales .......................................................................... 2 Index / Índice ........................................................................................ 6 Peach State Health Plan November/2020 -

Health-Careers-Manual-2016.Pdf
30417 Health Career Booklet Cvr_r1.indd 1 3/15/16 12:42 PM Table of Contents Acknowledgments Foothills Area Health Education Center (AHEC) is pleased to present the 10th edition of Health Careers in Georgia. This publication is produced through the partnership of the Georgia Statewide AHEC Network consisting of six centers with support from the Georgia legislature and the US Department of Title Page ........................................................................3 Health and Human Services Health Resources and Services Administration. Many community and academic partners contributed time, expertise, and resources in producing this resource for the current and future healthcare workforce. Some content, photos, and/or layout ideas were provided by Pam What is AHEC? ....................................................................4 Reynolds and SOWEGA AHEC, staff from other Georgia AHECs, Jeremy Whigham Design, the Georgia Department of Labor, Phyllis Johnson with the Georgia Department of Education, Ralph Morrison and the Georgia Health Information & Management Association Board of Directors, the American AHEC Spotlight ....................................................................5 Society for Cytotechnology, Sheri Porter with American Academy of Family Physicians News, and Dru Nadler Photography. We appreciate all of the Healthcare Trends ...............................................................6-7 expert readers listed below for reviewing and editing the content of each career page thereby enabling us to produce -

2019 Ambetter and Bluecross Hospital List.Xlsx
Ambetter and BlueCross Hospital List Most doctors that practice at an in‐network hospital will also be in‐network. One exception we know is Piedmont Atlanta Hospital. Piedmont Hospital is in the Ambetter netwok, but very few Piedmont Doctors are. It's always best to check with the insurance company's Search Tool or with the Provider directly. Hospital Name City Zip Ambetter BlueCross Emory University Hospital Atlanta 30322 X Emory University Hospital Midtown Atlanta 30308 X Emory Saint Joseph Atlanta 30342 X Emory Johns Creek Duluth 30097 X Emory Wesley Woods Hospital Atlanta 30329 X Northside Hospital Atlanta 30342 X Northside Hospital Cherokee Canton 30115 X Northside Hospital Forsyth Cumming 30041 X WellStar Atlanta Medical Center Atlanta 30312 X X WellStar Windy Hill Marietta 30067 X X WellStar Cobb Austell 30106 X X WellStar North Fulton Hospital Roswell 30076 X X WellStar Douglas Douglasville 30134 X Wellstar Kennestone Hospital Marietta 30060 X X WellStar Paulding Hiram 30141 X X WellStar Spalding Griffin 30224 X X WellStar Sylvan Grove Jackson 30233 X X WellStar Atlanta Medical Center South East Point 30344 X X Wellstar West Georgia Medical Center Lagrange 30240 X X DeKalb Medical Center Decatur 30033 X X Dekalb Medical Center at Hillendale Lithonia 30058 X X Shepherd Center Atlanta 30305 X X Gwinnett Medical Center Duluth Lawrenceville 30096 X X Gwinnett Medical Center Lawrenceville 30046 X X Childrens Healthcare of Atlanta Scottish Rite Atlanta 30342 X X Children Healthcare of Atl Hughes Spaulding Atlanta 30303 X X Childrens -

Relocation Guide to Atlanta, Georgia Home Abroad
EuRA: Atlanta City Guide Updated: 8/24/2016 Helping you feel at Relocation guide to Atlanta, Georgia home abroad. February 8, 2018 Relocation Guide to Atlanta, Georgia www.iorworld.com IOR makes every effort to ensure that the information contained in this guide is as current as possible. If you notice errors, or information which is no longer accurate, please contact us immediately so that we may correct the issue. i IOR Global Services • All Rights Reserved Worldwide TABLE OF CONTENTS WELCOME & OVERVIEW ................................................................................................................. 1 EMERGENCY AND HOSPITALS ......................................................................................................... 4 HOUSING ......................................................................................................................................... 7 US EDUCATION SYSTEM ................................................................................................................ 14 SCHOOLS IN THE AREA .................................................................................................................. 22 BANKING ....................................................................................................................................... 25 PUBLIC TRANSPORTATION/DRIVING ............................................................................................ 27 LOCAL REGISTRATIONS- SOCIAL SECURITY AND DRIVER’S LICENSE ............................................. 28 -
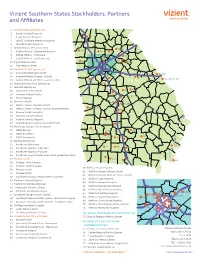
2018 Vizient Southern States Membership Map-Apr
Vizient Southern States Stockholders, Partners and Affiliates 1 Archbold Medical Center, Inc. 2 Brooks County Hospital 18 3 Grady General Hospital 19 16 4 John D. Archbold Memorial Hospital 5 Mitchell County Hospital 6 DeKalb Regional Health System 27, 28 28, 31 10 7 DeKalb Medical - Downtown Decatur 3433 35 30 8 DeKalb Medical - Hillandale 14, 63 33 30 9 DeKalb Medical - North Decatur 11 29 7 10 Floyd Medical Center 66 43 11 Polk Medical Center 12 Gwinnett Health System, Inc. 51, 52, 53 13 Glancy Rehabilitation Center 54, 56 69 14 Gwinnett Medical Center - Duluth 58 15 Gwinnett Medical Center - Lawrenceville 53, 55, 57, 59 70 GEORGIA 16 Hamilton Health Care System, Inc. 68 17 Houston Healthcare 25, 26 25 18 Houston Heart Institute 26 19 Houston Medical Center 24 24, 64 21, 22, 27 20 Perry Hospital 21 Navicent Health 23 17, 18, 19 22 Medical Center, Navicent Health 20, 21, 22 44, 45, 46 23 Medical Center of Peach County, Navicent Health 20 69 24 Monroe County Hospital 73 8, 9, 11, 61 25 Navicent Health Baldwin 23 26 Putnam General Hospital 40 68, 70 10 27 Rehabilitation Hospital, Navicent Health 75 28 Northeast Georgia Health System 29 NGMC Barrow 42 39 62 76 30 NGMC Braselton 66 31 NGMC Gainesville 37, 38 41 50, 52 6774 32 Northside Hospital 36 33 Northside Alpharetta 65 5 72 47, 48 34 Northside Hospital - Cherokee 51 41 34 35 50 35 Northside Hospital - Forsyth 40, 42, 43, 44 36 Northside Hospital Outpatient Center @ Meridian Mark 3 37 Phoebe Health 1, 4 3 260 49 38 Phoebe – Main Campus 6 48 46 39 Phoebe – North Campus 60 WellStar Health -

Facility Name Address City State Zip Emergency Radiology Pathology
The Surprise Bill Rating System provides a list of in-network hospitals and indicates whether the hospital has contracted hospital-based physicians (anesthesiologists, pathologists, radiologists, and emergency medicine physicians). The rating system displays checkmarks and X-marks between zero and four that an in-network hospital has earned based upon the number of in-network hospital-based specialty group types. Each checkmark indicates the presence of an in-network particular type of qualified hospital-based specialty group. An X-mark indicates the absence of an in-network particular type of qualified hospital-based specialty group. If a hospital does not provide one of the qualified hospital-based specialties, the absence of that specialty shall be designated by a green N/A mark. You should contact the hospital to determine if they might provide a physician that is not contracted with your plan. Facility Name Address City State Zip Emergency Radiology Pathology Anesthesiology AdventHealth Gordon 1035 Red Bud Rd NE Calhoun GA 30701 ✓ ✓ ✓ ✓ AdventHealth Murray 707 Old Dalton Ellijay Rd Chatsworth GA 30705 ✓ ✓ ✓ ✓ Appling Hospital 163 E Tollison St Baxley GA 31513 ✓ ✓ ✓ ✓ Bacon County Hospital 302 S Wayne St Alma GA 31510 ✓ ✓ ✓ Berrien County Hospital 1221 E McPherson Ave Nashville GA 31639 ✓ Bleckley Memorial Hospital 145 E Peacock St Cochran GA 31014 ✓ ✓ Burke Medical Center Health Clinic 351 S Liberty St Waynesboro GA 30830 ✓ ✓ ✓ Candler County Hospital 400 Cedar St Metter GA 30439 ✓ ✓ Candler General Hospital 5353 Reynolds -

Certificate of Need Tracking and Appeals Report
OFFICE OF GENERAL COUNSEL Georgia Department of Community Health CERTIFICATE OF NEED g TRACKING and APPEALS REPORT May 31, 2004 Health Plannin f Division o Georgia Department of Community Health Office of General Counsel 2 Peachtree Street 40th Floor Atlanta, Georgia 30303-3159 (404) 656-0456 (404) 656-0442 Fax www.communityhealth.state.ga.us Certificate of Need Tracking and Appeals Report New Applications Appealed Projects and Determinations Pending Review/Incomplete Applications Requests for LNR-MRI Units Pending Review/Complete Applications Requests for LNR-Physician Owned Amb Surg Facilities Recently Approved Applications Requests for miscellaneous Letters of Determination Applications withdrawn by Applicant Requests for Extended Implementation Period 2 New Applications 2004-043 Northside Hospital - Forsyth Construction of Women's Center/New Maternity and Newborn Services Filed: 5/25/2004 Site: 1200 Northside Forsyth Drive, Cumming, GA 30041 (Forsyth County) Contact: Brian J Toporek 404-851-6821 Estimated Cost: $34,957,824 2004-044 Rockdale Medical Center Addition of 2nd CT Scanner Filed: 5/28/2004 Site: 1412 Milstead Avenue, NE, Conyers, GA 30012 (Rockdale County) Contact: Joy L Davis 770-918-3914 Estimated Cost: $1,931,379 2004-045 Fayette Community Hospital New Perinatal Service Filed: 5/28/2004 Site: 1255 Highway 54 West, Fayetteville, GA 30214 (Fayette County) Contact: Michael Burnett 770-719-7000 Estimated Cost: $1,228,300 Pending Review/Incomplete Applications 2004-032 Ashley Glen Addition of 5 Beds and Renovation of Facility -

HS&R Q3 Report, 2017
SFY 2018: GEORGIA DEPARTMENT OF COMMUNITY HEALTH GEORGIA FAMILIES MEDICAID CARE MANAGEMENT ORGANIZATIONS ACT COMPLIANCE MONITORING ANALYSES OF HOSPITAL STATISTICAL AND REIMBURSEMENT (HS&R) REPORT SUBMISSIONS QUARTER 3: JULY 2017 THROUGH SEPTEMBER 2017 March 21, 2018 www.mslc.com page 1 TABLE OF CONTENTS Project Background .................................................................................................... 3 Objective ..................................................................................................................... 4 Methodology ............................................................................................................... 5 Assumptions and Limitations ...................................................................................... 6 Analytical Findings ..................................................................................................... 7 Findings Summary ..................................................................................................... 8 Recommendations .................................................................................................. 10 Exhibits .................................................................................................................... 11 www.mslc.com page 2 PROJECT BACKGROUND The Medicaid Care Management Organizations Act (the “Act”) requires the Care Management Organizations (CMOs) to provide a Hospital Statistical and Reimbursement (HS&R) report within 30 (thirty) days upon request of a provider. Specifically,