District Health Plans 2015/2016
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ethembeni Cultural Heritage
FINAL REPORT PHASE 1 HERITAGE IMPACT ASSESSMENT REPORT: SCOPING AND ENVIRONMENTAL IMPACT ASSESSMENT FOR THE PROPOSED EXPANSION OF PIETERMARITZBURG AIRPORT, MSUNDUZI MUNICIPALITY, KWAZULU-NATAL Prepared for Institute of Natural Resources 67 St Patricks Road, Pietermaritzburg, 3201 Box 100396, Scottsville, 3209 Telephone David Cox 033 3460 796; 082 333 8341 Fax 033 3460 895 [email protected] Prepared by eThembeni Cultural Heritage Len van Schalkwyk Box 20057 Ashburton 3213 Pietermaritzburg Telephone 033 326 1815 / 082 655 9077 Facsimile 086 672 8557 [email protected] 03 January 2017 PHASE 1 HERITAGE IMPACT ASSESSMENT OF EXPANSION OF PIETERMARITZBURG AIRPORT, KWAZULU-NATAL MANAGEMENT SUMMARY eThembeni Cultural Heritage was appointed by the Institute of Natural Resources to undertake a Phase 1 Heritage Impact Assessment of the proposed expansion of Pietermaritzburg Airport, as required by the National Environmental Management Act 107 of 1998 as amended (NEMA), in compliance with Section 38 of the National Heritage Resources Act 25 of 1999 (NHRA). Description and significance assessment of heritage resources Pietermaritzburg Aeroclub Clubhouse The building is older than sixty years and located next to the modern airport terminal buildings. Its continued use for the same purpose over a period of more than sixty years, including its expansions, contribute to give it medium to high heritage significance at community-specific and local levels for its historic, social and cultural values. Its associational value could extend further if it proves that the nearby Italian POW church and the clubhouse were both constructed from Hlatshana shale, and that the construction of the former gave rise to the use of a locally novel material to build the latter. -

30Km from Ballito from 30Km Richard’S Zinkwazi Bay Zinkwazi Beach
CAPPENY ESTATES 30KM FROM BALLITO UMHLALI SHAKASKRAAL STANGER R74 R102 ALBERT LUTHULI MEMORIAL STANGER HOLLA TRAILS SUGARRUSH HOSPITAL PARK DUKUZA MUSEUM PALM TRINITYHOUSE LAKES COLLISHEEN FUNCTION VENUE SCHOOL ESTATE CLUBHOUSE R102 UMHLALI LAP POOL MANOR PREPARATORY ESTATES RETIREMENT VILLAGE SCHOOL NONOTI RICHARD’S ACACIA INDUSTRIAL PARK BAY DRIVING RANGE N2 MVOTI FLAG ANIMAL FARM ZINKWAZI UMHLALI CALEDON IMBONINI INDUSTRIAL PARK TIFFANY’S GOLF SHAKA’S MHALALI ESTATE HEAD SHOPPING CENTRE SO-HIGH SHAKA’S PRE-PRIMARY INDUSTRIAL PARK SCHOOL BROOKLYN SHEFFIELD SHORTENS MANOR ESTATE UMHLALI COUNTRY EDEN VILLAGE CLUB TANGLEWOOD THE LITCHI BLYTHEDALE WESTBROOK ORCHARD COASTAL ESTATE VILLAGE ELALENI KIDZ CURRO BRETTENWOOD WAKENSHAW SCHOOL ZULULAMI MDLOTANE VIRGIN ACTIVE GYM ECO-KIDZ PRE-SCHOOL LIFESTYLE BALLITO DUNKIRK EQUESTRIAN SIMBITHI CENTRE JUNCTION CENTRE COUNTRY MONT CLUB MOUNT SHEFFIELD SIMBITHI RICHMORE CALM ECO ESTATE RETIREMENT VILLAGE BEACH ASHTON GRANTPRINCE’S GOLF COLLEGE NEW SALT BIRDHAVENLOXLEY ESTATE ROCK CITY ESTATE THE WELL SIMBITHI OFFICE PARK IZULU OFFICE PARK HERON ZINKWAZI COMMUNITY CENTRE BEACH NETCARE ALBERLITO SKI BOAT HOSPITAL LAUNCH SALT ROCK CHRISTMAS TINLEY HOTEL BAY BEACH MANOR SHEFFIELD BEACH DOLPHIN COAST PRE-PRIMARY SALT BEACH ROCK GRANNY TIFFANY’S CARAVAN POOLS BALLITO PARK BEACH CARAVAN PARK SALT ROCK PROMENADE BEACH TIDAL POOL THOMPSON’S CLARKE BAY SALMON TIDAL BLYTHEDALE ZINKWAZI BAY WILLARD’S BAY POOL BEACH BALLITO SHAKA’S ROCK SALT ROCK SHEFFIELD TINLEY MANOR. -

Provincial Clinic, CHC and Hospital Distances from Pietermaritzburg
Provincial Clinic, CHC and Hospital Distances from Pietermaritzburg Institution Name Distance (km) Health District Suburb Tel Code Tel Number A.E. Haviland Clinic 120.2 DC23 WEENEN 036 354 1872 Addington Clinic 81.97 Durban DURBAN 031 332 2111 Addington Hospital 81.97 Durban DURBAN 031 327 2000 Altona Clinic 421.29 DC26 PONGOLA 034 413 1707 Amakhabela Clinic 117.93 DC24 KRANSKOP 033 444 0662 Amaoti Clinic 84.17 Durban MOUNT EDGECOMBE 031 519 5967 Amatikulu Chronic Sick Home Hospital 163.93 DC29 AMATIKULU 032 453 0057 Amatimatolo Clinic 90.74 DC24 GREYTOWN 033 445 9319 Appelsbosch Hospital 65.45 DC22 OZWATHINI 032 294 0002 Assisi Clinic 155.58 DC21 PORT SHEPSTONE 039 695 9476 Ballito Clinic 116.72 DC29 BALLITO 032 946 8000 Baniyena Clinic 77.62 DC22 MOBENI 039 974 9004 Baphumile Clinic 153.24 DC21 PORT SHEPSTONE 039 684 7000 Beatrice Street Clinic 79.07 Durban CONGELLA 031 309 6222 Benedictine Hospital 294.83 DC26 NONGOMA 035 831 0314 Bethesda Hospital 369.42 DC27 UBOMBO 035 595 1004 Bhekumthetho Clinic 244.17 DC26 VRYHEID 038 933 0162 Bhekuzulu Clinic 270.39 DC26 VRYHEID 034 981 4892 Bhomela Clinic 189.18 DC21 PORT SHEPSTONE 039 685 0176 Bhoybhoyi Clinic 182.18 DC21 PORT SHEPSTONE 039 687 7831 Boom Street Clinic 3.86 DC22 PIETERMARITZBURG 033 395 1339 Bramhill Building Env. Health 2.83 DC22 PIETERMARITZBURG 033 394 1901 Bruntville CHC 64.42 DC22 MOOI RIVER 033 263 1545 Busingatha Clinic 201.87 DC23 ESTCOURT 036 438 6180 Buxdene Clinic 308.92 DC26 NONGOMA 035 838 0296 Caluza Clinic 11.66 DC22 PIETERMARITZBURG 033 399 3561 Catherine Booth -
Ilembe WC WDM Report
iLembe District Municipality Update on WC/WDM Program– Performance in 2014/15 Financial Year and 2015/16 Financial Year Outlook iLembe District Municipality • Located 65km north of Durban • One of the poorest Districts in KZN, yet one of the fastest growing • Significant tourism and cultural attractions iLembe District Municipality: System Characteristics • Total population - 680 000 • total number of connections – 34 632 • total length of mains - 2 205km • total number of water schemes – 111 • Currently in drought situation NRW Reduction Strategy Executive Summary 2018/19 No Further 2018/19 with 2013/14 Intervention Intervention System Input Volume 63 558 79 228 73 681 (kl/day) Billed Authorised 26 487 42 691 49 366 Consumption (kl/day) Non-Revenue Water 37 071 36 537 24 315 (kl/day) NRW by Volume % 58.3% 46.1% 33.0% 5-year Capex R308 000 000 Requirement (ex VAT) 5-year Opex R91 000 000 Requirement (ex VAT) 5-year Targets: • Infrastructure Leakage Index (ILI) 1,4 • Leakage Performance Category A2 • Inefficiency of Use of Water Resources 12,3 % • Non-Revenue Water by Volume 33,3 % • No Drop Assessment Score 90,0 iLembe District Municipality: Trends iLembe District Municipality: Year-on-Year iLembe District Municipality: Year-on-Year iLembe District Municipality: Year-on-Year iLembe District Municipality: Year-on-Year 2014/15 Financial Year Review • The impact of restrictions was felt, both from a bulk supply and consumer sales perspective • Apart from that, it was a good year – it was the first year that the full benefit of mains replacement and leakage reduction activities were realised 2015/16 Financial Year WC/WDM Activities • Continuation of planned mains replacement programme in KwaDukuza (last FY 45km, this FY 34km) • Continued pressure management in KwaDukuza and Ndwedwe • Aggressive leak detection and repair throughout KwaDukuza and Ndwedwe • Control valve and zone maintenance • Private property leakage reduction in KwaDukuza • Regularisation of reticulation in Mandini • If funds approved, 30% demand reduction in Ndwedwe and Groutville . -

KWADUKUZA LOCAL MUNICIPALITY the KWAZULU-NATAL SCHEME SYSTEM Zoning Companion Document 1
KWADUKUZA LOCAL MUNICIPALITY THE KWAZULU-NATAL SCHEME SYSTEM Zoning Companion Document 1 NOVEMBER 2016 Prepared for: The Municipal Manager KwaDukuza Local Municipality 14 Chief Albert Luthuli Street KwaDukuza 4450 Tel: +27 032 437 5000 E-mail: [email protected] Contents 1.0 DEFINING LAND USE MANAGEMENT? ......................................................................................... 3 2.0 WHY DO WE NEED TO MANAGE LAND? ..................................................................................... 3 3.0 WHAT IS LAND USE PLANNING? ................................................................................................... 4 4.0 WHO IS RESPONSIBLE FOR LAND USE PLANNING? ................................................................ 4 5.0 THE LEGAL FRAMEWORK ............................................................................................................... 5 6.0 MANAGING LAND THROUGH A SUITE OF PLANS .................................................................... 6 7.0 WHAT ARE THE ELEMENTS OF THE LAND USE SCHEME? ................................................. 11 7.1 STATEMENTS OF INTENT (SOI) .............................................................................................. 11 7.2 LAND USE DEFINITIONS............................................................................................................. 12 7.3 ZONES 12 7.4 THE SELECTION OF ZONES AND THE PREPARATION OF A SCHEME MAP ................ 13 8.0 DEVELOPMENT PARAMETERS / SCHEME CONTROLS ....................................................... -

Ilembe District Municipality – Quarterly Economic Indicators and Intelligence Report: 2Nd Quarter 2012
iLembe District Municipality – Quarterly Economic Indicators and Intelligence Report: 2nd Quarter 2012 ILEMBE DISTRICT MUNICIPALITY NOVEMBER 2010 QUARTERLY ECONOMIC INDICATORSNOVEMBER 2010 AND INTELLIGENCE REPORT SECOND QUARTER 2012 APRIL-JUNE Enterprise iLembe Cnr Link Road and Ballito Drive Ballito, KwaZulu-Natal Tel: 032 – 946 1256 Fax: 032 – 946 3515 iLembe District Municipality – Quarterly Economic Indicators and Intelligence Report: 2nd Quarter 2012 FOREWORD This intelligence report comprises of an assessment of key economic indicators for the iLembe District Municipality for the second quarter of 2012, i.e. April to June 2012. This is the 6th edition of the quarterly reports, which are unique to iLembe as we are the only district municipality to publish such a report. The overall objective of this project is to present economic indicators and economic intelligence to assist Enterprise iLembe in driving its mandate, which is to drive economic development and promote trade and investment in the District of iLembe. This quarter sees the inclusion of updated annual data for 2011 which was released by Quantec in the first week of August 2012. The updated data shows that iLembe has grown by 2.9% in 2011, up from 2.7% in 2010, with the tertiary sector showing the most significant growth. Manufacturing has been taken over by ‘finance, insurance, real estate and business services’ as the highest contributor to GDP. The unemployment rate has reduced in 2011 to 21.3%, and iLembe has managed to attract 4% more highly skilled workers than the previous year. See further updated annual stats from page 41 onwards. All the regular quarterly statistics are also included from page 15. -

ACTIVE HERITAGE Cc
Umdloti River Bridge FIRST PHASE HERITAGE IMPACT ASSESSMENT OF THE PROPOSED UMDLOTI RIVER BRIDGE AND REALIGNMENT OF MAIN ROAD P713, NDWEDWE LOCAL MUNICIPALITY ACTIVE HERITAGE cc. For: Kerry Seppings Environmental Consultants Frans Prins MA (Archaeology) P.O. Box 947 Howick 3290 [email protected] [email protected] December 2014 Fax: 086 7636380 Active Heritage cc for KSEMS i Umdloti River Bridge TABLE OF CONTENTS 1 BACKGROUND INFORMATION ON THE PROJECT........................................... 1 1.1. Details of the area surveyed: ........................................................................ 2 2 BACKGROUND INFORMATION OF THE SURVEY ............................................. 5 2.1 Methodology ................................................................................................. 5 2.2 Restrictions encountered during the survey .................................................. 5 2.2.1 Visibility..................................................................................................... 5 2.2.2 Disturbance............................................................................................... 5 2.3 Details of equipment used in the survey........................................................ 5 3 DESCRIPTION OF SITES AND MATERIAL OBSERVED..................................... 5 3.1 Locational data ............................................................................................. 5 3.2 Description of heritage sites identified.......................................................... -
Export This Category As A
South African Government Provincial and Local Government Directory: KwaZulu-Natal Municipalities 2021-09-27 Table of Contents AbaQulusi Local Municipality .............................................................................................................................. 3 Alfred Duma Local Municipality ........................................................................................................................... 3 Amajuba District Municipality .............................................................................................................................. 3 Big 5 Hlabisa Local Municipality (The) ................................................................................................................ 4 City of uMhlathuze Local Municipality ................................................................................................................ 4 Dannhauser Local Municipality ............................................................................................................................ 4 Dr Nkosazana Dlamini Zuma Local Municipality ................................................................................................ 5 eDumbe Local Municipality .................................................................................................................................. 5 Emadlangeni Local Municipality .......................................................................................................................... 6 Endumeni Local Municipality .............................................................................................................................. -

Ilembe District Municipality: Biodiversity Sector Plan
ILembe District Municipality: Biodiversity Sector Plan Version: 1.0 Date: March 2014 i Biodiversity Sector Plan - iLembe District Municipality 2014 Document Details Authored by: Felicity Elliott & Dr Boyd Escott Ezemvelo KZN Wildlife P.O. Box 13053 Cascades, 3202 Document is available from: Ezemvelo KZN Wildlife website, www.kznwildlife.com This guideline should be cited as: Ezemvelo KZN Wildlife (2013), iLembe Biodiversity Sector Plan, V1.0, Unpublished Report by Ezemvelo KZN Wildlife, Biodiversity Conservation Planning Division, Ezemvelo KZN Wildlife, P. O. Box 13053, Cascades, Pietermaritzburg. RECOMMENDED Title Name Signature Date Chairperson: EKZNW, SSOC Chief Executive Officer EKZNW APPROVED Chairperson: KZN Nature Conservation Board - Biodiversity Sector Plan - iLembe District Municipality 2014 Acknowledgements Specialists involved in development, consulting or review during production of the iLembe District Biodiversity Sector Plan include the following key persons. Dr Boyd Escott Manager: Biodiversity Spatial Planning & Information Acting GIS Analysis Terrestrial Felicity Elliott Biodiversity Spatial Planning & Information (Bioregional planning) Heidi Snyman Biodiversity Spatial Planning & Information (cartographer) Ezemvelo KZN Wildlife Bimall Naidoo Biodiversity Spatial Planning & Information (GIS Technician Terrestrial) Shiven Rambarath Biodiversity Spatial Planning & Information (GIS technician – Intern) Vusi Gumede District Conservation Officer Sue George Consultants for the Local Knowledge Balanced Environment Input Process -
•Ar •Ap •Ap •Ap •Ap •Ap •Ap •Ap •Ap •Ap •Ap •Ap
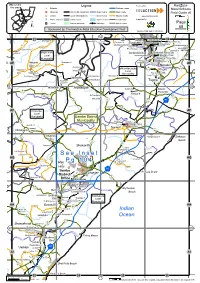
Map covers Legend Produced by: KwaZulu- this area Schools National roads Natal Schools ! Hospitals District Municipalities Major rivers Main roads Field Guide v5 Clinics Local Municipalities Minor rivers District roads www.eduAction.co.za !W Police stations Urban areas Dams / Lakes Local roads Supported by: Towns Nature reserves Railways Minor roads Page 68 Sponsored by: The KwaZulu-Natal Education Development Trust KwaZulu-Natal Dept of Education 58 33 34 35 Udumo H Khayalemfundo Jp 36 Mvumase P Manqindi Jp Siyavikelwa Sp Dendethu P Mandeni P $ Imbewenhle P Ubuhlebesundumbili Jp Ndondakusuka Ss O Thukela S !W Sundumbili P O Iwetane P Khululekani P Siyacothoza P Ethel Mthiyane Lsen Cranburn P Timoni P Maphumulo !!"% !!" Impoqabulungu S Local % Municipality !W 1 North Coast Mandini Pp '!" Nsungwini C Christian Acad Mandini AE AE % O Acad Nyakana P eNdondakusuka 1 Maqumbi P Banguni S 1 #!$ Local Mzobanzi Js Tugela S % O Municipality Lower Tugela P Qondukwazi P Tshelabantu P Ramlakan P &! Shekembula H Mgqwaba- % gqwaba P 1 !W 67 69 Newark P 1 " Hulett P St Christopher P 1 Imbuyiselo S N2 1 1 1 1 1 Nonoti P 1 AF Ndwedwe AF Local Municipality iLembe District Municipality Hulsug P Darnall S 1 Ashville P Lee P % Darnall P Prospect # " Farm P O 1 ()* Bongimfundo P 1 % 1 1 Kearsney P Harry Bodasing P Lethithemba S Ensikeni P See Inset AG O AG New Lubisana P O 1 Pg 104 Guelderland Int Farm ! L Bodasing P O -

Ilembe District Municipality
AGRI-PARK DISTRICT: ILEMBE PROVINCE: KWAZULU-NATAL REPORTING DATE: MARCH 2016 KEY COMMODITIES AGRIPARK COMPONENTS STATUS Sub-tropical fruit (mango, litchi and 4 FPSUs to be located in: Mandeni (2), Maphumulo and DAMC Established avocado) Ndwedwe The final draft of the master plan was submitted on the Vegetables 1 Agri-Hub to be located in KwaDukuza 29/02/2016 Poultry 1 RUMC located within the Agri-Hub site in KwaDukuza KEY CATALYTIC PROJECTS AGRO-PROCESSING BUSINESS OPPORTUNITIES KEY ROLE-PLAYERS Vegetables: investment in the iLembe Mango: sorting; fresh packing; branding; juicing; drying; Public Sector Industry Other Schools Nutrition Programme will assist the preserving into jams, chutney and atchar and processing KZN DARD North East Farmers Co-op Agri-Business market for smallholder primary producers to for medicinal uses DRDLR Emambedwini Farmers Development grow and become more established through Litchi: Sorting; fresh packing; branding; pureeing and iLembe DM Association Agency Enterprise iLembe Nsogweni Farmers AFASA expansion. preserving into sweets, liqueurs and other products; juicing KwaDukuza LM Association KwaDukuza Poultry: two small scale DRDLR projects have Avocado: sorting; fresh packing; branding; pureeing and Mandeni LM KwaMaphumulo Farmers Association been established in Mandeni, however no preserving into guacamole and other dips; oils Maphumulo LM Association GDARD Agri-Hubs KZN EDTEA Groutvillle Farmers Development real processing has occurred within these Vegetables: storage; ripening; washing; sorting; fresh KZN CoGTA Associations Agri-BEE facilities. packing; branding and processing into pastes are all highly Ndwedwe LM Phuhlisani Solutions Sub-Tropical Fruits: No investment has recommended. Pureeing; canning; drying; storing in oil; Ministry of Agriculture KZN Poultry Institute currently been realised, however the Litchi pulverising into powder and preparing for cooking sauces CASP National Regulatory orchard is the most formal environment upon are other possibilities. -

Provincial Road Network
D O L 3 1 9 5 Sabuyaze H Nyamazane 0 D 5 P 1 2 0 Intandoyethu LP 4 P20- 3 1 Nsungwini CP 8 2 7 O D1527 7 6 3 O 5 5 0 6 L 2 Nothweni LP 6 153 0 2 2 P711 1 3 D L 3 1 8 L 4 0 OL 8 Nsongansonga C 4 9 D O 4 2 2 023 1 0 0 L L 2 0 4 7 2 P 2 2 0 3 0 L Siphamandla CP Zephania JS L D O 5 4 2 6 1 7 0 O 7 4 1 1 O 0 0 0 5 L L 6 - 7 1 7 2 5 Vikindlala CP O 1 6 2 0 0 4 O L 3 L 5 3 2 0 9 L 0 5 0 3 5 P415 3 3 O 1 O L D 5 2 L 6 6 1 1 8 L 5 D O Manyonyo LP 1 Dangazela P 2 1 3 D 7 0 0 9 0 Emgaga LP 3 Maqumbi Nyakana CP 4 L 6 3 3 Vukuzenzele LP Umvoti H 6 O 1 2 2 2 4 7 6 4 O Indosi LP 2 3 2 9 O 2 2 0 3 0 L 0 5 1 8 2 6 L 1 L 6 D 0 4 L P 3 3 3 D O 0 0 2 2 O 0 0 O 5 7 L L 6 3 Tugela SS 3 0 O L 0 L 4 7 3 5 1 3 6 5 O 2 9 5 1 Otimati O 1 2 O 4 2 1 0 1 2 1 9 0 0 1 O 4 L 2 L L L !.