PATH Intl. Standards for Certification and Accreditation 2018
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Frecker's Saddlery
Frecker’s Saddlery Frecker’s 13654 N 115 E Idaho Falls, Idaho 83401 addlery (208) 538-7393 S [email protected] Kent and Dave’s Price List SADDLES FULL TOOLED Base Price 3850.00 5X 2100.00 Padded Seat 350.00 7X 3800.00 Swelled Forks 100.00 9X 5000.00 Crupper Ring 30.00 Dyed Background add 40% to tooling cost Breeching Rings 20.00 Rawhide Braided Hobble Ring 60.00 PARTIAL TOOLED Leather Braided Hobble Ring 50.00 3 Panel 600.00 5 Panel 950.00 7 Panel 1600.00 STIRRUPS Galvanized Plain 75.00 PARTIAL TOOLED/BASKET Heavy Monel Plain 175.00 3 Panel 500.00 Heavy Brass Plain 185.00 5 Panel 700.00 Leather Lined add 55.00 7 Panel 800.00 Heel Blocks add 15.00 Plain Half Cap add 75.00 FULL BASKET STAMP Stamped Half Cap add 95.00 #7 Stamp 1850.00 Tooled Half Cap add 165.00 #12 Stamp 1200.00 Bulldog Tapadero Plain 290.00 Bulldog Tapadero Stamped 350.00 PARTIAL BASKET STAMP Bulldog Tapadero Tooled 550.00 3 Panel #7 550.00 Parade Tapadero Plain 450.00 5 Panel #7 700.00 Parade Tapadero Stamped (outside) 500.00 7 Panel #7 950.00 Parade Tapadero Tooled (outside) 950.00 3 Panel #12 300.00 Eagle Beak Tapaderos Tooled (outside) 1300.00 5 Panel #12 350.00 7 Panel #12 550.00 BREAST COLLARS FULL BASKET/TOOLED Brannaman Martingale Plain 125.00 #7 Basket/Floral Pattern 2300.00 Brannaman Martingale Stamped 155.00 #12 Basket/Floral 1500.00 Brannaman Martingale Basket/Tooled 195.00 Brannaman Martingale Tooled 325.00 BORDER STAMPS 3 Piece Martingale Plain 135.00 Bead 150.00 3 Piece Martingale Stamped 160.00 ½” Wide 250.00 3 Piece Martingale Basket/Tooled 265.00 -

Press Notice
1 July 2008 Top to Toe: Fashion for Kids New exhibition at V&A Museum of Childhood relives 300 years of fashion for children 4 October 2008 - 19 April 2009 This autumn, the V&A Museum of Childhood will present a major exhibition exploring the history of children’s fashion, reliving iconic and defining moments from the past 300 years of children's clothing, vintage fashions, rare objects and photography. Top to Toe: Fashion for Kids will profile the changing attitudes, themes and fads of one of fashion’s most intriguing and enduring demographics, and promises to provide nostalgic moments for all generations. Visitors may recall evocative brands like Ladybird and Clothkits, or encounter classic memories from their own wardrobes such as parkas, knitted woollen swimsuits, leg warmers and ponchos. The Museum holds one of the most significant collections of children’s clothing in the world with over 6,000 outstanding items ranging from the 1700s to the present day, over 100 of which will be featured in the exhibition. Other objects, including a group of paintings depicting historical outfits from the V&A’s main collections, will complement the clothing on display. The exhibition will demonstrate how children’s clothing has changed over time, covering four broad themes: Milestones, Changing Fashions, Fashion Drivers and Practical Fashions. It will consider how materials, colours, shapes and styles have developed but will also show how many classic garments have remained unchanged or have been revived, due to practical design or enduring appeal. -
Historic Costuming Presented by Jill Harrison
Historic Southern Indiana Interpretation Workshop, March 2-4, 1998 Historic Costuming Presented By Jill Harrison IMPRESSIONS Each of us makes an impression before ever saying a word. We size up visitors all the time, anticipating behavior from their age, clothing, and demeanor. What do they think of interpreters, disguised as we are in the threads of another time? While stressing the importance of historically accurate costuming (outfits) and accoutrements for first- person interpreters, there are many reasons compromises are made - perhaps a tight budget or lack of skilled construction personnel. Items such as shoes and eyeglasses are usually a sticking point when assembling a truly accurate outfit. It has been suggested that when visitors spot inaccurate details, interpreter credibility is downgraded and visitors launch into a frame of mind to find other inaccuracies. This may be true of visitors who are historical reenactors, buffs, or other interpreters. Most visitors, though, lack the heightened awareness to recognize the difference between authentic period detailing and the less-than-perfect substitutions. But everyone will notice a wristwatch, sunglasses, or tennis shoes. We have a responsibility to the public not to misrepresent the past; otherwise we are not preserving history but instead creating our own fiction and calling it the truth. Realistically, the appearance of the interpreter, our information base, our techniques, and our environment all affect the first-person experience. Historically accurate costuming perfection is laudable and reinforces academic credence. The minute details can be a springboard to important educational concepts; but the outfit is not the linchpin on which successful interpretation hangs. -

High Adventure Awards
HIGH ADVENTURE AWARDS FOR SCOUTS AND VENTURERS 2016 HIGH ADVENTURE AWARDS SCOUTS & VENTURES BOY SCOUTS OF AMERICA - WESTERN REGION APRIL 2016 CHAPTER 1 ORANGE COUNTY AWARD/PROGRAM ACTIVITY AREA AWARD PAGE 3 SAINTS AWARD ANY APPROVED WILDERNESS AREA PATCH 1-15 BACKCOUNTRY LEADERSHIP ANY APPROVED WILDERNESS AREA PATCH 1-3 BOY SCOUT TRAIL BOY SCOUT TRAIL PATCH 1-9 BRON DRAGANOV HONOR AWARD ANYWHERE PATCH 1-1 BSA ROCKETEER SANCTIONED CLUB LAUNCH PATCH 1-11 CHANNEL ISLANDS ADVENTURER CHANNEL ISLANDS PATCH 1-14 CHRISTMAS CONSERVATION CORP ANYWHERE PATCH 1-12 DEATH VALLEY CYCLING 50 MILER DEATH VALLEY PATCH 1-10 EAGLE SCOUT LEADERSHIP SERVICE ANYWHERE PATCH 1-2 EAGLE SCOUT PEAK EAGLE SCOUT PEAK PATCH 1-6 EAGLE SCOUT PEAK POCKET PATCH EAGLE SCOUT PEAK PATCH 1-6 EASTER BREAK SCIENCE TREK ANYWHERE PATCH 1-13 HAT OUTSTANDING SERVICE AWARD SPECIAL PATCH 1-24 HIGH LOW AWARD MT. WHITNEY/DEATH VALLEY PATCH 1-1 JOHN MUIR TRAIL THROUGH TREK JOHN MUIR TRAIL MEDAL 1-4 MARINE AREA EAGLE PROJECT MARINE PROTECTED AREA PATCH 1-14 MT WHITNEY DAY TREK MOUNT WHITNEY PATCH 1-5 MT WHITNEY FISH HATCHERY FISH HATCHERY PATCH 1-11 NOTHING PEAKBAGGER AWARD ANYWHERE PATCH 1-8 SEVEN LEAGUE BOOT ANYWHERE PATCH 1-2 MILES SEGMENTS ANYWHERE SEGMENT 1-2 TELESCOPE PEAK DAY TREK TELESCOPE PEAK PATCH 1-9 TRAIL BUILDING HONOR AWARD ANY APPROVED WILDERNESS AREA PATCH 1-1 WHITE MOUNTAIN WHITE MOUNTAIN PATCH 1-5 WILDERNESS SLOT CANYONEERING SLOT CANYON SEGMENTS PATCH 1-7 ESCALANTE CANYONEERING ANYWHERE SEGMENT 1-7 PARIA CANYONEERING ANYWHERE SEGMENT 1-7 ZION CANYONEERING ANYWHERE SEGMENT -
Pocket Packing Guide You Will Find the Following Information
ABOUT LLAMAS Llamas Colorado LLC Llamas are superior pack animals. They are quiet, courteous, curious, intelligent, strong and agile. POCKET Llamas have soft pads on the bottom of their foot like a dog. This PACKING is optimal in helping to reduce environ- mental impact. They have two toes that GUIDE operate independ- ently, which makes This little guidebook should serve as a quick them very surefooted and easy to pack on reference - just in case you can't remember rough terrain. They are also very clean. every detail learned at orientation. They tend to go to the bathroom in the same spots if they John & Devin have been there before. We are so pleased that you have chosen us to help make your trip enjoyable, stress-free, and environmentally harmonious. We want you to enjoy our llamas as much as we do, and that involves knowing how to handle them on and off the trail. In this Pocket Packing Guide you will find the following information: Introduction . .1 About Llamas . .3 Preparing for your pack trip . .6 General Handling . .6 Loading the Panniers . .7 At the Trailhead . .7 Saddling . .8 On the Trail . .10 Trail Circumstances . .12 Meetings on the Trail . .14 Difficulties on the Trail . .14 Camp Time . .16 Llama on the Loose . .18 First Aid Kit for Llamas . .19 Do's & Don'ts quick reference list . .19 Knots . 21 Frequently asked questions . 23 Hello! Welcome Many thanks to Al & Sonora Ellis, Cindy Campbell, Elisabeth Myers, MJ Myers, Denise Newberry, and Katy to Thach for help with this booklet. -

Read Book Through England on a Side-Saddle Ebook, Epub
THROUGH ENGLAND ON A SIDE-SADDLE PDF, EPUB, EBOOK Celia Fiennes | 96 pages | 02 Apr 2009 | Penguin Books Ltd | 9780141191072 | English | London, United Kingdom Sidesaddle - Wikipedia Ninth century depictions show a small footrest, or planchette added to the pillion. In Europe , the sidesaddle developed in part because of cultural norms which considered it unbecoming for a woman to straddle a horse while riding. This was initially conceived as a way to protect the hymen of aristocratic girls, and thus the appearance of their being virgins. However, women did ride horses and needed to be able to control their own horses, so there was a need for a saddle designed to allow control of the horse and modesty for the rider. The earliest functional "sidesaddle" was credited to Anne of Bohemia — The design made it difficult for a woman to both stay on and use the reins to control the horse, so the animal was usually led by another rider, sitting astride. The insecure design of the early sidesaddle also contributed to the popularity of the Palfrey , a smaller horse with smooth ambling gaits, as a suitable mount for women. A more practical design, developed in the 16th century, has been attributed to Catherine de' Medici. In her design, the rider sat facing forward, hooking her right leg around the pommel of the saddle with a horn added to the near side of the saddle to secure the rider's right knee. The footrest was replaced with a "slipper stirrup ", a leather-covered stirrup iron into which the rider's left foot was placed. -

253 AMERICAN MINIATURE HORSE REGISTRY Driving Performance
AMERICAN MINIATURE HORSE REGISTRY Driving Performance Division Rules 5.1 Miniature Horse Driving Division – General Rules A. Guidance: The driving division was founded for the purpose of developing and furthering the art and sport of driving for pleasure. A working knowledge of and compliance with the rules are essential. B. The only person to handle the reins, under penalty of elimination, is the driver. No change of driver is per- mitted during any class. C. Dress Code: Headers, Drivers and their passengers should be dressed appropriately. Dress in the show ring is to complement the overall appearance of the unit, not take away from the appearance. 1. Hats for gentlemen are optional, except when in formal attire. 2. Formal wear should not be worn before 5 p.m. un- less stake classes are held in an afternoon perfor- mance session. 3. No strapless dresses in any driving class. Miniature Horse 4. No sandals or open toed shoes to be worn by driver or header. 5. No T-shirts or shorts. 6. No farm, individual, or animal names may be dis- played. Exception: Draft harness classes. D. Horses must be serviceably sound. E. Horses may be shown with a full mane or mane with bridle path clipped and full tail. F. Driving whips, if used, must be of suitable style, and the tip of the lash must not reach past the shoulder of the horse. Section XI - Driving Division Rules 253 G. Cross Entering: 1. Pleasure horses cannot cross-enter into Country Pleasure, Western Pleasure or Park Divisions at the same show. -

Mastering Equine - Advanced Horsemanship Mastering Horses
4-H Equine Series Mastering Equine - Advanced Horsemanship Mastering Horses The purpose of the Mastering Horses project is to help you to further develop skills in all areas of equine management. By setting goals to become a responsible horse owner and a good rider, you will become strong in the areas of self-discipline, patience, responsibility, respect Table of Contents and pride in your accomplishments. Introduction 1 As you progress through the Mastering Equine manual, remember that Skill Builder 1: 3 time is not limited. Follow the 4-H motto and “Learn to do by doing”. Ground work and Although you may finish the activities in the manual quite quickly and Psychology easily, you may wish to spend more time in this unit to improve your Skill Builder 2: Grooming 19 horsemanship skills. Be sure to Dream It! record what you wish to complete this club year. Then Do It! After your lessons and at your Skill Builder 3: Identification 30 Achievement you can Dig It! and Conformation Horsemanship is an art of riding in a manner that makes it look easy. Skill Builder 4: Safety and 55 To do this, you and your horse must be a happy team and this takes Stable Management time and patience. Skill Builder 5: Health 64 The riding skills you develop in this project will prepare you for Skill Builder 6: Riding 97 advancement. Whether you are interested in specialized riding Showcase Challenge 138 disciplines or horse training, you will need to learn more about aids and equipment. Portfolio Page 140 No matter what kind of goals you set for yourself in Mastering - Revised 2019 - Horsemanship, the satisfaction you experience will come from the results of your own hard work. -
Pennsylvania 4-H Horse Show Rule Book
Pennsylvania 4-H Horse Show Rule Book Revised 2018 Prepared by Bethany Bickel, Tammy Clark, Andrea Kocher, Amy Snover, Joe Stanco, Lew Trumble, Donna Zang, and with approval by The Pennsylvania 4-H Horse Program Development Committee and the State 4-H Office. This publication is made possible through Pennsylvania 4-H program fees. Penn State College of Agricultural Sciences research and extension programs are funded in part by Pennsylvania counties, the Commonwealth of Pennsylvania, and the U.S. Department of Agriculture. Where trade names appear, no discrimination is intended, and no endorsement by Penn State Extension is implied. Penn State encourages persons with disabilities to participate in its programs and activities. If you anticipate needing any type of accommodation or have questions about the physical access provided, please contact your local extension office in advance of your participation or visit. This publication is available in alternative media on request. The University is committed to equal access to programs, facilities, admission, and employment for all persons. It is the policy of the University to maintain an environment free of harassment and free of discrimination against any person because of age, race, color, ancestry, national origin, religion, creed, service in the uniformed services (as defined in state and federal law), veteran status, sex, sexual orientation, marital or family status, pregnancy, pregnancy-related conditions, physical or mental disability, gender, perceived gender, gender identity, genetic information or political ideas. Discriminatory conduct and harassment, as well as sexual misconduct and relationship violence, violates the dignity of individuals, impedes the realization of the University’s educational mission, and will not be tolerated. -

Joseph Smith Period Clothing 145
Carma de Jong Anderson: Joseph Smith Period Clothing 145 Joseph Smith Period Clothing: The 2005 Brigham Young University Exhibit Carma de Jong Anderson Early in 2005, administrators in Religious Education at Brigham Young University gave the green light to install an exhibit (hopefully my last) in the display case adjacent to the auditorium in the Joseph Smith Building. The display would showcase the clothing styles of the life span of the Prophet Joseph Smith and the people around him (1805–1844). There were eleven mannequins and clothing I had constructed carefully over many years, mingled with some of my former students’ items made as class projects. Those pieces came from my teaching the class, “Early Mormon Clothing 1800–1850,” at BYU several years ago. There were also a few original pieces from the Joseph Smith period. During the August 2005 BYU Education Week, thousands viewed these things, even though I rushed the ten grueling days of installation for something less than perfect.1 There was a constant flow of university students passing by and stopping to read extensive signage on all the contents shown. Mary Jane Woodger, associate professor of Church History and Doctrine, reported more young people and faculty paid attention to it than any other exhibit they have ever had. Sincere thanks were extend- ed from the members of Religious Education and the committee plan- ning the annual Sydney B. Sperry October symposium. My scheduled lectures to fifteen to fifty people, two or three times a week, day or night for six months (forty stints of two hours each), were listened to by many of the thirty thousand viewers who, in thank-you letters, were surprised at how much information could be gleaned from one exhibit. -

Product Catalogue 1
Leading Brand in Harness & Accessories Product Catalogue 1 www.idealequestrian.com Ideal Equestrian Quality and reassurance Since 1994 Ideal Equestrian has been developing and producing a wide range of driving harness and accessories. The standard of our harness is our no.1 priority and together with successful national and international drivers, we are constantly improving in the design and technology of our products. Our harness ranges from a luxury traditional leather presentation 2 harness with full collar, to a marathon or high-tech synthetic EuroTech harness. Ideal has it all! This catalogue is just a selection of our products. Visit our website and view our full range, and discover what Ideal Equestrian has to offer you. www.idealequestrian.com LEADING BRAND IN HARNESS & ACCESSORIES Index HARNESS Luxe 4 Marathon 6 LeatherTech Combi 8 EuroTech Classic 12 3 EuroTech Combi 14 WebTech Combi 16 Ideal Friesian 18 Ideal Heavy horse 18 Harness Parts 19 Driving Accessories 20 Luxe • Traditional Classic Harness • High Quality Leather • Elegant appearance Sizes available: Full / Cob / Pony / Shetland / Mini Shetland 4 Leather LeatherLeather Leather Black Black/ London Australian Nut Luxe Options – Single: - Breast collar with continuous traces This traditionally made quality harness is perfect for all disciplines of carriage driving, durable enough (adjustment at carriage end) for tough conditions yet attractive for presentation. Nylon webbing is stitched between the leather where extra strength is needed. The saddle pad has foam filled cushions, holes are oval to prevent - Traces with Rollerbolt or Crew hole tearing and all buckles have stainless steel tongues. Nose band is fully adjustable and headpiece is - Leather Reins tapered in the middle to create more freedom around the ears. -
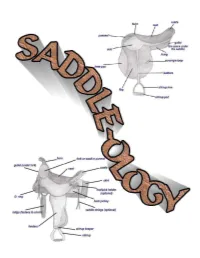
Saddleology (PDF)
This manual is intended for 4-H use and created for Maine 4-H members, leaders, extension agents and staff. COVER CREATED BY CATHY THOMAS PHOTOS OF SADDLES COURSTESY OF: www.horsesaddleshop.com & www.western-saddle-guide.com & www.libbys-tack.com & www.statelinetack.com & www.wikipedia.com & Cathy Thomas & Terry Swazey (permission given to alter photo for teaching purposes) REFERENCE LIST: Western Saddle Guide Dictionary of Equine Terms Verlane Desgrange Created by Cathy Thomas © Cathy Thomas 2008 TABLE OF CONTENTS Introduction.................................................................................4 Saddle Parts - Western..................................................................5-7 Saddle Parts - English...................................................................8-9 Fitting a saddle........................................................................10-15 Fitting the rider...........................................................................15 Other considerations.....................................................................16 Saddle Types & Functions - Western...............................................17-20 Saddle Types & Functions - English.................................................21-23 Latigo Straps...............................................................................24 Latigo Knots................................................................................25 Cinch Buckle...............................................................................26 Buying the right size