Routes of Medication Administration (P 2)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

List of New Drugs Approved in India from 1991 to 2000
LIST OF NEW DRUGS APPROVED IN INDIA FROM 1991 TO 2000 S. No Name of Drug Pharmacological action/ Date of Indication Approval 1 Ciprofloxacin 0.3% w/v Eye Indicated in the treatment of February-1991 Drops/Eye Ointment/Ear Drop external ocular infection of the eye. 2 Diclofenac Sodium 1gm Gel March-1991 3 i)Cefaclor Monohydrate Antibiotic- In respiratory April-1991 250mg/500mg Capsule. infections, ENT infection, UT ii)Cefaclor Monohydrate infections, Skin and skin 125mg/5ml & 250mg/5ml structure infections. Suspension. iii)Cefaclor Monohydrate 100mg/ml Drops. iv)Cefaclor 187mg/5ml Suspension (For paediatric use). 4 Sheep Pox Vaccine (For April-1991 Veterinary) 5 Omeprazole 10mg/20mg Short term treatment of April-1991 Enteric Coated Granules duodenal ulcer, gastric ulcer, Capsule reflux oesophagitis, management of Zollinger- Ellison syndrome. 6 i)Nefopam Hydrochloride Non narcotic analgesic- Acute April-1991 30mg Tablet. and chronic pain, including ii)Nefopam Hydrochloride post-operative pain, dental 20mg/ml Injection. pain, musculo-skeletal pain, acute traumatic pain and cancer pain. 7 Buparvaquone 5% w/v Indicated in the treatment of April-1991 Solution for Injection (For bovine theileriosis. Veterinary) 8 i)Kitotifen Fumerate 1mg Anti asthmatic drug- Indicated May-1991 Tablet in prophylactic treatment of ii)Kitotifen Fumerate Syrup bronchial asthma, symptomatic iii)Ketotifen Fumerate Nasal improvement of allergic Drops conditions including rhinitis and conjunctivitis. 9 i)Pefloxacin Mesylate Antibacterial- In the treatment May-1991 Dihydrate 400mg Film Coated of severe infection in adults Tablet caused by sensitive ii)Pefloxacin Mesylate microorganism (gram -ve Dihydrate 400mg/5ml Injection pathogens and staphylococci). iii)Pefloxacin Mesylate Dihydrate 400mg I.V Bottles of 100ml/200ml 10 Ofloxacin 100mg/50ml & Indicated in RTI, UTI, May-1991 200mg/100ml vial Infusion gynaecological infection, skin/soft lesion infection. -

Formulation and Evaluation of Transdermal Patch and Gel of Nateglinide
Human Journals Research Article September 2015 Vol.:4, Issue:2 © All rights are reserved by C. Aparna et al. Formulation and Evaluation of Transdermal Patch and Gel of Nateglinide Keywords: Nateglinide, transdermal patch and gel, HPMC, ethyl cellulose, carbopol, PVA, PVP ABSTRACT Anusha Gundeti, C. Aparna*, Dr. Prathima Srinivas The objective of the present work was to formulate Transdermal Drug Delivery systems of Nateglinide, an Department of Pharmaceutics, Sri Venkateshwara antidiabetic drug belonging to meglitinide class with a half life of 1.5 hrs. Transdermal patches containing nateglinide were College of Pharmacy, prepared by solvent casting method using the combinations Affiliated to Osmania University, of HPMC:EC, PVA:PVP, HPMC:Eudragit RS 100, Eudragit RL100:RS100 in different proportions and by incorporating Madhapur, Hyderabad, Telangana -500081, India. different permeation enhancers (polyethylene glycol 400, Su bmission: 7 September 2015 DMSO). The transdermal patches were evaluated for their physicochemical properties like thickness, weight variation, Accepted: 11 September 2015 folding endurance, percentage moisture absorption, percentage Published: 25 September 2015 moisture loss, in-vitro diffusion studies & ex-vivo permeation studies. Transdermal Gel was formulated using HPMC, carbopol 934, carbopol 940 and methyl cellulose. Gels were evaluated for homogeneity, pH, viscosity, drug content, in-vitro diffusion studies & ex-vivo permeation studies. By comparing the drug release F5 (HPMC:EC) formulation was selected as optimized formulation as it could sustain the drug release for 12 hrs i.e. 99.2% when compared to gel. Stability studies were www.ijppr.humanjournals.com carried out according to ICH guidelines and the patches maintained integrity and good physicochemical properties during the study period. -
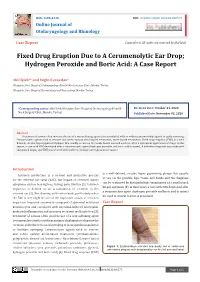
Fixed Drug Eruption Due to a Cerumenolytic Ear Drop; Hydrogen Peroxide and Boric Acid: a Case Report
ISSN: 2688-8238 DOI: 10.33552/OJOR.2020.04.000577 Online Journal of Otolaryngology and Rhinology Case Report Copyright © All rights are reserved by Akif İşlek Fixed Drug Eruption Due to A Cerumenolytic Ear Drop; Hydrogen Peroxide and Boric Acid: A Case Report Akif İşlek1* and Engin Karaaslan2 1Nusaybin State Hospital, Otolaryngology-Head & Neck Surgery Clinic, Mardin, Turkey 2Nusaybin State Hospital, Dermatology and Venereology, Mardin, Turkey *Corresponding author: Received Date: October 24, 2020 Published Date: November 03, 2020 Akif İşlek, Nusaybin State Hospital, Otolaryngology-Head & Neck Surgery Clinic, Mardin, Turkey. Abstract Treatment of earwax often involves the use of a wax softening agent (cerumenolytic) with or without antimicrobial agents to easily removing. Cerumenolytic agents used to remove and soften earwax areoil-based treatments, water-based treatments. Fixed drug eruption (FDE) is a well- defined, circular, hyperpigmented plaque that usually occurs on the trunk, hands mucosal surfaces, after a systemical application of drugs. In this report, a case with FDE developed after a cerumenolytic agent (hydrogen peroxide and boric acid in water). A definitive diagnosis was made with skin punch biopsy and FDE was treated with oral levocetirizine and topical mometasone. Introduction is a well-defined, circular, hyper pigmenting plaque that usually Cerumen production is a normal and protective process occurs on the genitals, lips, trunk, and hands and the diagnosis for the external ear canal (EAC), but impact of cerumen causes can be confirmed by histopathologic examination of a small punch symptoms such as hearing loss, itching, pain, tinnitus [1]. Cerumen biopsy specimen [5]. In this report, a case with FDE developed after impaction is defined as an accumulation of cerumen in the a cerumenolytic agent (hydrogen peroxide and boric acid in water) external ear [2]. -
Inhalation Devices: Various Forms of Administration for Therapeutic Optimization
vv ISSN: 2640-8082 DOI: https://dx.doi.org/10.17352/oja CLINICAL GROUP Renata Cristina de Angelo Calsaverini Leal* Review Article Santa Fé do Sul Foundation of Education and Culture, Brazil Inhalation Devices: Various forms Dates: Received: 31 May, 2017; Accepted: 26 June, of administration for Therapeutic 2017; Published: 27 June, 2017 *Corresponding author: Renata Cristina de Angelo Optimization Calsaverini Leal, Santa Fé do Sul Foundation of Education and Culture, Brazil, Tel: 55 (17) 3272-2769, E-mail: Keywords: Inhalation; Aerosol; Nebulizer Summary https://www.peertechz.com Introduction: Aerosol therapy consists of spraying liquid particles suspended for therapeutic purposes in the respiratory tract. With direct absorption and deposition at the lung level, avoiding side effects and presenting fast response time. Several factors infl uence the drug action, such as size, particle movement, ventilatory fl ow, pulmonary expansion, anatomy, respiratory mechanics and the nebulizer and patient interface. The therapeutic optimization depends on the type of nebulizer differentiating itself by the physical principle that generates the mist. Objectives: Check advantages and disadvantages of different inhalation devices. Methodology. This is a review of the PubMed database using descriptors: ultrasonic and jet nebulizer, aerosol deposition in the lung, metered dose inhaler and dry, inhaler therapy. Results: Different devices are mentioned in the literature: pneumatic and ultrasonic nebulizers (administering solutions), metered pressurized inhalers - pMDI used with or without expander chamber (administering suspensions) and dry powder inhalers - DPI (administering powder). Discussion and Conclusion: The US has advantages: quiet, does not require coordinating abilities, without propellant gases and quick nebulization with small amount of solution. Disadvantages: change in the active principle of thermosensitive drugs, deposition in the oropharynx and VAI of 2% of inhaled particles. -
CS/CS/HB 1373 Persons with Developmental Disabilities
HOUSE OF REPRESENTATIVES STAFF ANALYSIS BILL #: CS/CS/HB 1373 Persons with Developmental Disabilities SPONSOR(S): Health & Human Services Committee; Children, Families & Seniors Subcommittee; Stevenson TIED BILLS: IDEN./SIM. BILLS: CS/SB 1788 REFERENCE ACTION ANALYST STAFF DIRECTOR or BUDGET/POLICY CHIEF 1) Children, Families & Seniors Subcommittee 9 Y, 0 N, As CS Gilani Brazzell 2) Health & Human Services Committee 16 Y, 0 N, As Gilani Calamas CS SUMMARY ANALYSIS The Agency for Persons with Disabilities (APD) is responsible for providing services to persons with developmental disabilities. Persons with developmental disabilities reside in various types of residential settings, including community-based residential facilities licensed and regulated by APD. Medication services are an important element of care for individuals with developmental disabilities in APD facilities and are often provided by unlicensed direct service providers (DSPs). Medication assistance or administration typically involves observation of the client to ensure correct self- administration of medication, or directly giving or applying the medication as prescribed, respectively. Medication administration is generally a nurse’s responsibility; however, a majority of states, including Florida, allows trained unlicensed personnel to perform these tasks to meet the demand. Currently, trained unlicensed personnel can provide or supervise eight routes of medication administration (enteral, inhaled, ophthalmic, oral, otic, rectal, topical, and transdermal). Currently, unlicensed personnel must complete a 4-hour initial training course in medication administration and have their skills assessed and validated by a registered nurse or physician in each route of administration they intend to use. This assessment includes onsite observation of the administration of medication to or supervision of self-administration by a client. -

Inhaled Steroids in Asthma a Patient's Guide
I I v v v v d v v Patient advice and liaison service (PALS) Actions r v If you have a compliment, complaint or It is sensible to ensure you make the r concern please contact our PALS team on following steps now you have a new r 020 7288 5551 or inhaler d [email protected] d d Pick up our guide on inhalers and If you need a large print, audio or spacers to complement this leaflet translated copy of this leaflet please Inhaled Steroids in Agree on a personalised asthma contact us on 020 7288 3182. We will try plan (this is done with your doctor or our best to meet your needs. Asthma nurse and usually written down for future reference) Remember to take your medicines A patient’s guide as advised Should your inhalers fail to relieve your symptoms, go straight to Accident and Emergency Need Help? Whittington Paediatric Asthma Nurse Tel: 020 7288 5527 Whittington Health Community Nurse Magdala Avenue Islington 020 3316 1950 (8am-6pm) London N19 5NF Haringey 020 8887 3301 (9am – 5pm) Phone: 020 7272 3070 www.whittington.nhs.uk Asthma UK 0300 222 5800 Date published: 25/09/2018 www.asthma.org.uk Review date: 25/09/2020 Ref: C&YP/Paed/ISA/03 © Whittington Health Please recycle Tel: 020 7272 3070 Asthma There are many types of preventer Side Effects Asthma is a common condition affecting inhaler. There are simple steroids like Parents worry about children and young the airway. Usually a trigger (such as dust beclomethasone, and then there are also adults taking inhaled steroids because of or pollen) irritates the airways which combined inhalers, called seretide or side effects they’ve heard about. -

Member List 2016
To help make the use of prescription drugs safer and more affordable, our plan is now using a Drug Quantity Management program. That is, for certain medications, you can receive an amount to last you a certain number of days. This gives you the right amount to take the daily dose considered safe and effective, according to the recommendations of the U.S. Food and Drug Administration (FDA). Based on the FDA’s guidelines and other medical information, our plan developed this program together with Express Scripts, the company chosen to manage our prescription drug benefit. The following limits are based on a 30-day supply. If your plan allows for additional days supply, your limits may be higher. For instance, you may be able to get a 90-day supply of your medication through mail order service. Your doctor could also request a prior authorization. If this request is approved, a prior authorization would let you receive more than the recommended quantity. Drug Target Maximum Quantity ABSTRAL 100 MCG TAB SUBLINGUAL 90 units per 30 days ABSTRAL 200 MCG TAB SUBLINGUAL 90 units per 30 days ABSTRAL 300 MCG TAB SUBLINGUAL 90 units per 30 days ABSTRAL 400 MCG TAB SUBLINGUAL 90 units per 30 days ABSTRAL 600 MCG TAB SUBLINGUAL 90 units per 30 days ABSTRAL 800 MCG TAB SUBLINGUAL 90 units per 30 days ACTIQ 1,200 MCG LOZENGE 90 units per 30 days ACTIQ 1,600 MCG LOZENGE 90 units per 30 days ACTIQ 200 MCG LOZENGE 90 units per 30 days ACTIQ 400 MCG LOZENGE 90 units per 30 days ACTIQ 600 MCG LOZENGE 90 units per 30 days ACTIQ 800 MCG LOZENGE 90 units per -

Rectal Suppository & Enema Administration to Administration Unlicensed Assistive Personnel (UAP) Module/Skill Checklist
Delegation of Medication Rectal Suppository & Enema Administration to Administration Unlicensed Assistive Personnel (UAP) Module/Skill Checklist Objective At the completion of this module, the UAP should be able to administer rectal suppository & enema medications. NOTE: 1) The RN or LPN is permitted to delegate ONLY after application of all components of the NCBON Decision Tree for Delegation to UAP and after careful consideration that delegation is appropriate: a) for this client, b) with this acuity level, c) with this individual UAP’s knowledge and experience, and d) now (or in the time period being planned). 2) Successful completion of the “Infection Control” module by the UAP should be documented prior to instruction in medication administration by this or ANY route. Procedure for: SUPPOSITORY 1. Perform skills in General Medication Administration Checklist. 2. Provide privacy. Have client void before procedure. 3. Put on clean gloves. 4. Position the client on their left (preferred) side with the top leg bent slightly. 5. Remove the foil or wrapper from the suppository, if present. 6. Apply a small amount of lubricant to the suppository and your gloved index finger on your dominant hand – the hand holding the suppository. 7. Separate the buttocks with your gloved, non dominant hand. 8. Ask the client to breathe slowly and deeply through the mouth. 9. Place tip of suppository against anus and gently insert the suppository about 4- inches along the rectal wall. Avoid putting the suppository in stool. 10. After removing your finger, squeeze buttocks together for a few minutes to help client hold in the suppository for as long as possible. -

Absorbine Veterinary Liniment for Horses
Doc# 03.287 Ver. 11 SAFETY DATA SHEET ABSORBINE® VETERINARY LINIMENT SECTION 1 - PRODUCT AND COMPANY IDENTIFICATION 1.1 Trade Name (as labeled): Absorbine® Veterinary Liniment Synonyms: N/A CAS No: Mixture 1.2 Product Use: Soothes sore muscles and stiff joints 1.3 Company Name: W.F. Young Company Address: 302 Benton Dr Company Address Cont: East Longmeadow, MA 01028 Business Phone: ( 413) 526-9999 Website: www.wfyoung.com 1.4 Emergency Telephone Number: (413) 526-9999 Date of Current Revision: January 17, 2017 Date of Last Revision: August 7, 2015 SECTION 2 - HAZARD IDENTIFICATION EMERGENCY OVERVIEW: This product is a green thin liquid with an acetone odor. Health Hazards: May cause skin, eye, and respiratory system irritation. Flammabilit Hazards: This product is a flammable liquid with a flash point over 20°F (-6. 7°C). Reactivit Hazards: None. Environmental Hazards: The environmental effectsof this product have not been investigated, however release may cause long term adverse environmental effects. US DOT Symbols: EU and GHS Symbols: Signal Word: Danger! 2.1 CLASSIFICATION OF SUBSTANCE OR MIXTURE IN ACCORDANCE WITH 29 CFR 1200 (OSHA HCSl AND THE EUROPEAN UNION DIRECTIVES: This product does meet the definition of a hazardous substance or preparation as defined by 29 CFR 1910. 1200 or the European Union Council Directives 67 /548/EEC, 1999/45/EC, 1272/2008/EC and subsequent Directives. EU HAZARD CLASSIFICATIONOF INGREDIENTS PER DIRECTIVE 1272/2008/EC: IndexNumber: EC# 201-939-0 This substance is not classified in the AnnexVI of Directive 67/548/EEC EC# 200-662-2 This substance is classified in the AnnexVI of Directive 67/548/EEC Index# 606-001-00-8 Substances not listed either individually or in group entries must be self classified. -

Clinical Practice Statements-Oral Contact Allergy
Clinical Practice Statements-Oral Contact Allergy Subject: Oral Contact Allergy The American Academy of Oral Medicine (AAOM) affirms that oral contact allergy (OCA) is an oral mucosal response that may be associated with materials and substances found in oral hygiene products, common food items, and topically applied agents. The AAOM also affirms that patients with suspected OCA should be referred to the appropriate dental and/or medical health care provider(s) for comprehensive evaluation and management of the condition. Replacement and/or substitution of dental materials should be considered only if (1) a reasonable temporal association has been established between the suspected triggering material and development of clinical signs and/or symptoms, (2) clinical examination supports an association between the suspected triggering material and objective clinical findings, and (3) diagnostic testing (e.g., dermatologic patch testing, skin-prick testing) confirms a hypersensitivity reaction to the suspected offending material. Originators: Dr. Eric T. Stoopler, DMD, FDS RCSEd, FDS RCSEng, Dr. Scott S. De Rossi, DMD. This Clinical Practice Statement was developed as an educational tool based on expert consensus of the American Academy of Oral Medicine (AAOM) leadership. Readers are encouraged to consider the recommendations in the context of their specific clinical situation, and consult, when appropriate, other sources of clinical, scientific, or regulatory information prior to making a treatment decision. Originator: Dr. Eric T. Stoopler, DMD, FDS RCSEd, FDS RCSEng, Dr. Scott S. De Rossi, DMD Review: AAOM Education Committee Approval: AAOM Executive Committee Adopted: October 17, 2015 Updated: February 5, 2016 Purpose The AAOM affirms that oral contact allergy (OCA) is an oral mucosal response that may be associated with materials and substances found in oral hygiene products, common food items, and topically applied agents. -

Consumer Education
CONSUMER EDUCATION Massachusetts General Laws Penalties for Possession or Possession with the Intent to Distribute • Consumers may not sell marijuana to any other individual • Marijuana is a class D controlled substance under the Massachusetts Controlled Substances Act - Mass. Gen. Laws. ch. 94C, § 31 Possession for Personal Use An adult may possess up to one ounce of marijuana; up to 5 grams of marijuana may be marijuana concentrate. Within a primary residence, an adult may possess up to 10 ounces of marijuana and any marijuana produced by marijuana plants cultivated on the premises. An adult who possesses more than one ounce of marijuana or marijuana products must secure the products with a lock. • Mass. Gen. Laws. ch. 94G, § 7 • Mass. Gen. Laws. ch. 94G § 13(b) Possession of more than one ounce of marijuana is punishable by a fine of $500 and/or imprisonment of up to 6 months. However, first offenders of the controlled substances act will be placed on probation and all official records relating to the conviction will be sealed upon successful completion of probation. Subsequent offenses may result in a fine of $2000 and/or imprisonment of up to 2 years. Individuals previously convicted of felonies under the controlled substances act who are arrested with over an ounce of marijuana may be subject to a fine of $2000 and/or up to 2 years of imprisonment. • Mass. Gen. Laws. ch. 94C, § 34 Possession with Intent to Distribute For first offenders, possessing less than 50 pounds of marijuana with the intent to manufacture, distribute, dispense or cultivate is punishable by a fine of $500-$5,000 and/or imprisonment of up to 2 years. -

Inhalation Solution, USP for Oral Inhalation Use What Is Tobramycin
PATIENT INFORMATION TOBRAMYCIN (TOE-BRA-MYE-SIN) Inhalation Solution, USP for oral inhalation use What is Tobramycin Inhalation Solution? Tobramycin inhalation solution is a prescription medicine that is used to treat people with cystic fibrosis who have a bacterial infection called Pseudomonas aeruginosa. Tobramycin inhalation solution contains an antibacterial medicine called tobramycin (an aminoglycoside). It is not known if tobramycin inhalation solution is safe and effective: in children under 6 years of age in people who have an FEV1 less than 25% or greater than 75% predicted in people who are colonized with a bacterium called Burkholderia cepacia Do not take tobramycin inhalation solution if you are allergic to tobramycin, any of the ingredients in tobramycin inhalation solution, or to any other aminoglycoside antibacterial. See the end of this Patient Information for a complete list of ingredients in tobramycin inhalation solution. Before you take tobramycin inhalation solution, tell your healthcare provider about all of your medical conditions, including if you: have or have had hearing problems (including noises in your ears such as ringing or hissing) have dizziness have or have had kidney problems have or have had problems with muscle weakness such as myasthenia gravis or Parkinson’s disease have or have had breathing problems such as wheezing, coughing, or chest tightness are pregnant or plan to become pregnant. Tobramycin inhalation solution is in a class of drugs that can harm your unborn baby. are breastfeeding or plan to breastfeed. It is not known if tobramycin passes into your breast milk. are receiving aminoglycoside therapy by injection or through a vein (intravenous) while taking tobramycin inhalation solution.