2-Muscles Involved in Respiration.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Diapositiva 1
Thoracic Cage and Thoracic Inlet Professor Dr. Mario Edgar Fernández. Parts of the body The Thorax Is the part of the trunk betwen the neck and abdomen. Commonly the term chest is used as a synonym for thorax, but it is incorrect. Consisting of the thoracic cavity, its contents, and the wall that surrounds it. The thoracic cavity is divided into 3 compartments: The central mediastinus. And the right and left pulmonary cavities. Thoracic Cage The thoracic skeleton forms the osteocartilaginous thoracic cage. Anterior view. Thoracic Cage Posterior view. Summary: 1. Bones of thoracic cage: (thoracic vertebrae, ribs, and sternum). 2. Joints of thoracic cage: (intervertebral joints, costovertebral joints, and sternocostal joints) 3. Movements of thoracic wall. 4. Thoracic cage. Thoracic apertures: (superior thoracic aperture or thoracic inlet, and inferior thoracic aperture). Goals of the classes Identify and describe the bones of the thoracic cage. Identify and describe the joints of thoracic cage. Describe de thoracic cage. Describe the thoracic inlet and identify the structures passing through. Vertebral Column or Spine 7 cervical. 12 thoracic. 5 lumbar. 5 sacral 3-4 coccygeal Vertebrae That bones are irregular, 33 in number, and received the names acording to the position which they occupy. The vertebrae in the upper 3 regions of spine are separate throughout the whole of life, but in sacral anda coccygeal regions are in the adult firmly united in 2 differents bones: sacrum and coccyx. Thoracic vertebrae Each vertebrae consist of 2 essential parts: An anterior solid segment: vertebral body. The arch is posterior an formed of 2 pedicles, 2 laminae supporting 7 processes, and surrounding a vertebral foramen. -

Unit 2 Lab 2
Unit 2, Lab 1 PTA/OTA 106 Regional A & P G. Blevins Updated: Fall 2011 SURFACE ANATOMY: VERTEBRAL COLUMN BONES [26] Jugular or suprasternal notch Vertebra (general features) Sternal angle Body Manubrium Neural arch Body of the sternum Pedicles Xiphisternal joint Laminae Costal margin Spinal (or vertebral) foramen Costal arch Transverse processes Anterior median line Spinous process Midclavicular lines Superior articulating processes Intermammary cleft Inferior articulating processes Axillary fossa Intervertebral foramen Anterior axillary line Intervertebral disc Anterior axillary fold Midaxillary line Thoracic vertebrae [12] Posterior axillary line Rib facets or demifacets Posterior median line Scapular lines Lumbar vertebrae [5] Epigastric fossa Lack rib facets and transverse Iliac crest foramina Umbilicus Linea alba Sacrum [1] Rectus abdominis Fused bone consisting of 5 Serratus anterior vertebrae Semilunar line Sacral promontory Sacral foramina (pelvic & dorsal) VERTEBRAL COLUMN- Auricular surface Special Features Coccyx [1] Normal Curves Fused bone consisting of 3-5 Primary: vertebrae Thoracic Sacral THORACIC BONES [25] Secondary: Sternum [1] Cervical Manubrium Lumbar Body (or gladiolus) Abnormal Curves Jugular (or suprasternal) notch Kyphosis Xiphoid process Lordosis Ribs [12 pair] Scoliosis Head Neck Tubercle Body (or shaft) Costal groove Costal cartilages Types of ribs True ribs False ribs Floating ribs PECTORAL (OR SHOULDER) GIRDLE Clavicles [2] Sternal extremity Acromial extremity Conoid tubercle Scapula [2] Borders: Superior -

Epithelia Joitns
NAME LOCATION STRUCTURE FUNCTION MOVEMENT Temporomandibular joint Condylar head of ramus of Synovial Diarthrosis Modified hinge joint mandible and glenoid fossa of Rotation and gliding temporal bone Biaxial Zygapophyseal joint Between articular processes of Synovial Diarthrosis Gliding 2 adjacent vertebrae Non axial Atlanto-Occipital joints Atlas and occipital condyle of Synovial Diarthrosis Ellipsoid occipital bone Biaxial Atlantoaxial joints Atlas and axis Synovial Diarthrosis Pivot Uniaxial Joints of vertebral arches Ligaments Fibrous Amphiarthrosis Syndesmoses Intervertebral symphyseal Intervertebral disk between 2 Cartilaginous Amphiarthrosis joints vertebrae Symphysis Costovertebral Head of ribs and body of Synovial Diarthrosis Gliding thoracic vertebra Non axial Costotrasnverse joints Tubercle of rib and transverse Synovial Diarthrosis Gliding process of thoracic vertebra Non axial Lumbosacral Joint Left and right zygopophyseal Laterally Synovial joint Intervertebral symphyseal joint Symphysis SternoclavicularJoint Clavicular notch articulates Synovial Diarthrosis Gliding with medial ends of clavicle Non Axial Manubriosternal Joint Hyaline cartilage junction Cartilaginous Synarthrosis Sternal Angle between manubrium and body Symphysis Xiphisternal Joint Cartilage between xiphoid Synchondrosis Synarthrosis process and body Synostoses Sternocostal Joint (1st) Costocartilage 1 with sternum Cartilaginous Synchondrosis Synarthrosis NAME Location Section Anterior longitudinal runs down anterior surface of vertebral body Vertebral column ligament Posterior longitudinal in canal, runs down posterior surface of vertebral body ligament Interspinous ligament Connects spinous processes Ligamentum flavum Connects laminae ! Intra-articular Disc Between articulating surface of sternum and clavicle Sternoclavicular Joint Costoclavicular ligament 1st rib to clavicle !. -

1 the Thoracic Wall I
AAA_C01 12/13/05 10:29 Page 8 1 The thoracic wall I Thoracic outlet (inlet) First rib Clavicle Suprasternal notch Manubrium 5 Third rib 1 2 Body of sternum Intercostal 4 space Xiphisternum Scalenus anterior Brachial Cervical Costal cartilage plexus rib Costal margin 3 Subclavian 1 Costochondral joint Floating ribs artery 2 Sternocostal joint Fig.1.3 3 Interchondral joint Bilateral cervical ribs. 4 Xiphisternal joint 5 Manubriosternal joint On the right side the brachial plexus (angle of Louis) is shown arching over the rib and stretching its lowest trunk Fig.1.1 The thoracic cage. The outlet (inlet) of the thorax is outlined Transverse process with facet for rib tubercle Demifacet for head of rib Head Neck Costovertebral T5 joint T6 Facet for Tubercle vertebral body Costotransverse joint Sternocostal joint Shaft 6th Angle rib Costochondral Subcostal groove joint Fig.1.2 Fig.1.4 A typical rib Joints of the thoracic cage 8 The thorax The thoracic wall I AAA_C01 12/13/05 10:29 Page 9 The thoracic cage Costal cartilages The thoracic cage is formed by the sternum and costal cartilages These are bars of hyaline cartilage which connect the upper in front, the vertebral column behind and the ribs and intercostal seven ribs directly to the sternum and the 8th, 9th and 10th ribs spaces laterally. to the cartilage immediately above. It is separated from the abdominal cavity by the diaphragm and communicates superiorly with the root of the neck through Joints of the thoracic cage (Figs 1.1 and 1.4) the thoracic inlet (Fig. -

Pictorial Essay
EDUCATIONAL REVIEW ER_024 Pictorial essay. ZATTAR-RAMOS, L.C.1* LEÃO, R.V. 1 CAVALCANTI, C.F.A.1 BORDALO-RODRIGUES, M.1 1 LEITE, C.C. HOSPITAL SÍRIO-LIBANÊS, 1 São Paulo – SP, Brazil. CERRI, G.G. *[email protected] 1Department of Radiology ▶ DISCLOSURE PARAGRAPHS: - The authors of this educational review declare no relationships with any companies, whose products or services may be related to the subject matter of the article. - The authors state that this work has not received any funding. ▶ INTRODUCTION: - Sternal abnormalities are commonly seen in clinical practice. - In addition to the numerous anatomical variations and congenital anomalies, the sternum and sternoclavicular joints can be affected by various pathological conditions such as trauma, infection, tumors, degenerative and inflammatory changes. - This study aims to demonstrate and illustrate such conditions, as the knowledge of its characteristics and imaging findings are essential for correct diagnosis and patient management. ▶ DISCUSSION: - Sternum injuries are common and should be properly recognized and characterized; using different imaging methods we will illustrate the variations of normality, congenital abnormalities and characteristic radiographic findings of sternal lesions highlighting: psoriatic arthritis, inflammatory osteitis, SAPHO syndrome, neoplastic, traumatic and degenerative lesions. ▶ ANATOMY: STERNUM: Flat bone, with 3 parts: *MANUBRIUM: superior central (jugular) notch and 2 lateral fossae that articulate with the MANUBRIUM clavicles. Also articulates with the 1o and 2o ribs and the body of the sternum. - Atachments: sternohyoideus, sternothyroideus, subclavius, pectoralis major, transversus thoracis and sternocleidomastoideus muscles. BODY OF *BODY OF THE STERNUM: articulates with the THE manubrium, xiphoid process and with the 2o STERNUM through 7o ribs. -

Muscles Involved in Respiration
Prof. Ahmed Fathalla Ibrahim Professor of Anatomy College of Medicine King Saud University E-mail: [email protected] OBJECTIVES At the end of the lecture, students should: ▪ Describe the components of the thoracic cage and their articulations. ▪ Describe in brief the respiratory movements. ▪ List the muscles involved in inspiration and in expiration. ▪ Describe the attachments of each muscle to the thoracic cage and its nerve supply. ▪ Describe the origin, insertion, nerve supply of diaphragm. THORACIC CAGE Vertebra Rib THORACIC CAGE ❑Conical in shape ❑Has 2 apertures (openings): 1. Superior (thoracic outlet): narrow, open, continuous with neck 2. Inferior: wide, closed by diaphragm ❑ Formed of: 1. Sternum & costal cartilages: anteriorly 2. Twelve pairs of ribs: laterally 3. Twelve thoracic vertebrae: posteriorly ARTICULATIONS Costovertebral Manubriosternal Intervertebral disc Costochondral Sternocostal Xiphisternal ARTICULATIONS Costovertebral Sternocostal Costochondral Interchondral ARTICULATIONS • Secondary cartilaginous: Manubriosternal joint, Xiphisternal joint and Intervertebral discs. • Primary cartilaginous: 1st Sternocostal joint, Costochondral joints and Interchondral joints. • Plane synovial joints: Costovertebral joints and the rest of Sternocostal joints. RESPIRATORY MOVEMENTS A- MOVEMENTS OF DIAPHRAGM Inspiration Contraction (descent) of diaphragm Increase of vertical diameter of thoracic cavity Relaxation (ascent) of diaphragm) Expiration RESPIRATORY MOVEMENTS B- MOVEMENTS OF RIBS PUMP HANDLE MOVEMENT BUCKET HANDLE -
Intervertebral Foramina - Wikipedia Visited on 06/06/2017
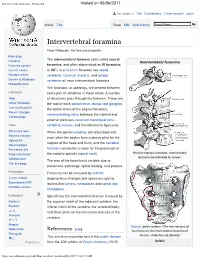
Intervertebral foramina - Wikipedia Visited on 06/06/2017 Not logged in Talk Contributions Create account Log in Article Talk Read Edit View history Intervertebral foramina From Wikipedia, the free encyclopedia Main page The intervertebral foramen (also called neural Contents Intervertebral foramina Featured content foramina, and often abbreviated as IV foramina Current events or IVF), is a foramen between two spinal Random article vertebrae. Cervical, thoracic, and lumbar Donate to Wikipedia vertebrae all have intervertebral foramina. Wikipedia store The foramina, or openings, are present between Interaction every pair of vertebrae in these areas. A number Help of structures pass through the foramen. These are About Wikipedia the root of each spinal nerve, dorsal root ganglion, Community portal the spinal artery of the segmental artery, Recent changes communicating veins between the internal and Contact page external plexuses, recurrent meningeal (sinu- Tools vertebral) nerves, and transforaminal ligaments. What links here When the spinal vertebrae are articulated with Related changes each other the bodies form a strong pillar for the Upload file support of the head and trunk, and the vertebral Special pages Permanent link foramen constitutes a canal for the protection of Page information the medulla spinalis (spinal cord). Peculiar thoracic vertebrae. Intervertebral foramina are indicated by arrows. Wikidata item The size of the foramina is variable due to Cite this page placement, pathology, spinal loading, and posture. Print/export Foramina can be occluded by arthritic Create a book degenerative changes and space-occupying Download as PDF lesions like tumors, metastases and spinal disc Printable version herniations. Languages Specifically the intervertebral foramen is bound by Deutsch the superior notch of the adjacent vertebra, the Español inferior notch of the vertebra, the vertebral body, and facet joints on the transverse process of the فارسی Français vertebra. -

Bones, Part 1: the Axial Skeleton
PowerPoint® Lecture Slides The Skeleton prepared by Leslie Hendon University of Alabama, Birmingham • Consists of: • Bones, cartilage, joints, and ligaments Composed of 206 named bones grouped into C H A P T E R • 7 two divisions Part 1 • Axial skeleton (80 bones) Bones, Part 1: • Appendicular skeleton (126 bones) The Axial Skeleton Copyright © 2011 Pearson Education, Inc. Copyright © 2011 Pearson Education, Inc. The Axial Skeleton(in green) The Axial Skeleton Cranium Skull Cranium Facial bones Bones of Clavicle pectoral Clavicle girdle • Formed from 80 Thoracic cage Scapula (ribs and Scapula Sternum sternum) Upper named bones Rib limb Humerus Rib Humerus Vertebra • Consists of skull, Vertebral Vertebra Radius column Radius Ulna Ulna vertebral column, Sacrum Carpals Bones of and bony thorax pelvic girdle Carpals Phalanges Phalanges Metacarpals Metacarpals Femur Femur Patella Lower Tibia limb Tibia Fibula Fibula Tarsals Metatarsals (a) Anterior view Phalanges (b) Posterior view Copyright © 2011 Pearson Education, Inc. Figure 7.1a Copyright © 2011 Pearson Education, Inc. Figure 7.1b The Skull The Cranium • Formed by cranial and facial bones • Is the body’s most complex bony structure Frontal bone Parietal bone Glabella • Formed by cranial and facial bones Squamous part Frontonasal suture of frontal bone Supraorbital foramen Nasal bone (notch) • The cranium Sphenoid bone Supraorbital margin (greater wing) Superior orbital fissure • Encloses and protects brain Temporal bone Optic canal Ethmoid bone Inferior orbital fissure Lacrimal bone • Provides attachment for head and neck Zygomatic bone Middle nasal concha muscles Infraorbital foramen Ethmoid Perpendicular plate bone Maxilla Inferior nasal concha Vomer Mandible Mental foramen Mental protuberance (a) Anterior view of skull Copyright © 2011 Pearson Education, Inc. -

Bone Scintigraphy and the Manubrio-Sternal Joint Laurie Renelle Margolies Yale University
Yale University EliScholar – A Digital Platform for Scholarly Publishing at Yale Yale Medicine Thesis Digital Library School of Medicine 1983 Bone scintigraphy and the manubrio-sternal joint Laurie Renelle Margolies Yale University Follow this and additional works at: http://elischolar.library.yale.edu/ymtdl Recommended Citation Margolies, Laurie Renelle, "Bone scintigraphy and the manubrio-sternal joint" (1983). Yale Medicine Thesis Digital Library. 2900. http://elischolar.library.yale.edu/ymtdl/2900 This Open Access Thesis is brought to you for free and open access by the School of Medicine at EliScholar – A Digital Platform for Scholarly Publishing at Yale. It has been accepted for inclusion in Yale Medicine Thesis Digital Library by an authorized administrator of EliScholar – A Digital Platform for Scholarly Publishing at Yale. For more information, please contact [email protected]. Permission for photocopying or microfilming of " __ 'S.c/aji / Ci iCft-Prfy Aajd ~tr/f (title of thesis) ijgin- 5;rr R.(Lifrt \ c)\ tO'*■” for the purpose of individual scholarly consultation or refer¬ ence is hereby granted by the author. This permission is not to be interpreted as affecting publication of this work, or otherwise placing it in the public domain, and the author re¬ serves all rights of ownership guaranteed under common law (Printed name) (Date) Digitized by the Internet Archive in 2017 with funding from The National Endowment for the Humanities and the Arcadia Fund https://archive.org/details/bonescintigraphyOOmarg BONE SCINTIGRAPHY AND THE MANUBRIO-STERNAL JOINT BY LAURIE RENELLE MARGOLIES A Thesis Submitted to the Yale University School of Medicine in Partial Fulfillment of the Requirements for the Degree of Doctor of Medicine May, 1983 TABLE OF CONTENTS Page I. -

A Reappraisal of Adult Thoracic and Abdominal Surface Anatomy Via CT Scan in Chinese Population
Clinical Anatomy 29:165–174 (2016) ORIGINAL COMMUNICATION A Reappraisal of Adult Thoracic and Abdominal Surface Anatomy via CT Scan in Chinese Population XIN-HUA SHEN,1† BAI-YAN SU,2† JING-JUAN LIU,2 GU-MUYANG ZHANG,2 2 2 3 1 HUA-DAN XUE, ZHENG-YU JIN, S. ALI MIRJALILI, AND CHAO MA * 1Department of Anatomy, Histology and Embryology, Institute of Basic Medical Sciences Chinese Academy of Medical Sciences, School of Basic Medicine Peking Union Medical College, Beijing, China 2Department of Radiology, Peking Union Medical College Hospital, Beijing, China 3Department of Anatomy with Radiology, Faculty of Medical and Health Sciences, University of Auckland, Auckland, New Zealand Accurate surface anatomy is essential for safe clinical practice. There are numer- ous inconsistencies in clinically important surface markings among and within contemporary anatomical reference texts. The aim of this study was to investi- gate key thoracic and abdominal surface anatomy landmarks in living Chinese adults using computed tomography (CT). A total of 100 thoracic and 100 abdom- inal CT scans were examined. Our results indicated that the following key surface landmarks differed from current commonly–accepted descriptions: the positions of the tracheal bifurcation, azygos vein termination, and pulmonary trunk bifur- cation (all below the plane of the sternal angle at vertebral level T5–T6 in most individuals); the superior vena cava formation and junction with the right atrium (most often behind the 1st and 4th intercostal spaces, respectively); and the level at which the inferior vena cava and esophagus traverse the diaphragm (T10 and T11, respectively). The renal arteries were most commonly at L1; the mid- point of the renal hila was most frequently at L2; the 11th rib was posterior to the left kidney in only 29% of scans; and the spleen was most frequently located between the 10th and 12th ribs. -
Disorders of the Thoracic Cage and Abdomen
Disorders of the thoracic cage and abdomen CHAPTER CONTENTS Heart (Fig. 1) Referred pain e185 Pain referred from visceral structures . e185 Ischaemic heart disease Pain referred from musculoskeletal structures not The innervation of the heart is derived from the C8–T4 seg- belonging to the thoracic cage . e191 ments. Pain is therefore not only felt in the chest but can also Disorders of the thoracic cage and abdomen e191 be referred to the ulnar side of both upper limbs, though more commonly to the left. Disorders of the inert structures . e191 It is traditionally accepted that pain felt in the chest radiat- Disorders of the contractile structures . e193 ing into the left arm is indicative of myocardial ischaemia, especially when the patient reports it as pressure, constriction, squeezing or tightness. However, none of these descriptions, which are usually regarded as characteristic of ischaemia, is of Pain in the thorax or abdomen can be the result of a local definitive aid in the differential diagnosis from other non- problem of either the thoracic wall or the abdominal muscles cardiogenic problems in the thorax. Even relief of pain after but it is more often referred from a visceral structure or the intake of glyceryl trinitrate does not offer absolute confir- from another musculoskeletal source, most frequently a disc mation of coronary ischaemia. For clinical diagnosis, a combina- protrusion. Therefore, it is wise to remember the only safe tion of several elements must be present, of which the most approach in this area is to achieve a diagnosis by both positive important is pain spreading to both arms and shoulders initi- confirmation of the lesion and exclusion of other possible ated by walking, especially after heavy meals or on cold days.1 disorders. -
Structure of the Thoracic Wall
human anatomy 2016 lecture eleven Dr meethak ali ahmed neurosurgeon opening of the thorax The thoracic cavity communicates with the root of the neck through an opening called the thoracic inlet ; is bounded post. by first thoracic vertebra, laterally by the medial border of the first ribs & their costal cartilage , & ant. by the superior border of the manubrium sterni. the opening is obliquely placed facing upward & forward . Through this small opening pass the esophagus &trachea and many vessels & nerve . because of the obliquely of the opening ,the apices of the lung and pleurae project upward into the neck. The thoracic cavity communicates with abdomen through a large opening called the thoracic outlet . The opening is bounded post. by the twelfth thoracic vertebrae , laterally by the curving costal margin ,& ant. by xiphisternal joint . Through this large opening , which is closed by the diaphragm ,pass the esophagus & many large vessels & nerve ,all which pierce the diaphragm. structure of the thoracic wall The thoracic wall is coverd on the outside by skin & by muscles attaching the shoulder girdle to the trunk. lined with parietal pleura . thoracic part of the vertebral column is concave forward & is made up of twelve vertebrae , together with their intervertebral disc. sternum the sternum is flat bone that may be divided into three parts reference, snell clinical anatomy human anatomy 2016 lecture eleven Dr meethak ali ahmed neurosurgeon manubrium; is the upper part of the sternum ,& it articulates with the clavical & the first & upper part of the second costal cartilages on each side . it opposite the third and fourth thoracic vertebrae.