Death Is Coming and the Clot Thickens, As Pyroptosis Feeds the Fire
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Gasdermin D: the Long-Awaited Executioner of Pyroptosis Cell Research (2015) 25:1183-1184
Cell Research (2015) 25:1183-1184. npg © 2015 IBCB, SIBS, CAS All rights reserved 1001-0602/15 $ 32.00 RESEARCH HIGHLIGHT www.nature.com/cr Gasdermin D: the long-awaited executioner of pyroptosis Cell Research (2015) 25:1183-1184. doi:10.1038/cr.2015.124; published online 20 October 2015 Inflammatory caspases drive a screen for mutations that would impair cell membrane that mediates release of lytic form of cell death called pyropto- activation of the caspase-11-dependent matured IL-1β from the cell. sis in response to microbial infection pathway. Through this screen, the au- To further dissect how gasdermin and endogenous damage-associated thors found that peritoneal macrophages D might contribute to the caspase- signals. Two studies now demonstrate harvested from a mouse strain harboring 11-dependent pathway, both groups that cleavage of the substrate gas- a mutation in the gene encoding gasder- performed a series of biochemical as- dermin D by inflammatory caspases min D, called GsdmdI105N/I105N (owing to says to demonstrate that recombinant necessitates eventual pyroptotic de- an isoleucine-to-asparagine substitu- caspase-11 cleaved gasdermin D be- mise of a cell. tion mutation at position 105), did not tween the Asp276 and Gly277 residues Inflammatory caspases, including undergo pyroptosis and release IL-1β of mouse gasdermin D, generating an N- caspase-1, -4, -5 and -11, are crucial in response to LPS transfection. On the terminal (30-31-kDa) and a C-terminal mediators of inflammation and cell other hand, Shao and colleagues utilized fragment (22-kDa). Caspase-4 or -5 also death. -

Mechanisms and Therapeutic Regulation of Pyroptosis in Inflammatory Diseases and Cancer
International Journal of Molecular Sciences Review Mechanisms and Therapeutic Regulation of Pyroptosis in Inflammatory Diseases and Cancer Zhaodi Zheng and Guorong Li * Shandong Provincial Key Laboratory of Animal Resistant, School of Life Sciences, Shandong Normal University, Jinan 250014, China; [email protected] * Correspondence: [email protected]; Tel.: +86-531-8618-2690 Received: 24 January 2020; Accepted: 17 February 2020; Published: 20 February 2020 Abstract: Programmed Cell Death (PCD) is considered to be a pathological form of cell death when mediated by an intracellular program and it balances cell death with survival of normal cells. Pyroptosis, a type of PCD, is induced by the inflammatory caspase cleavage of gasdermin D (GSDMD) and apoptotic caspase cleavage of gasdermin E (GSDME). This review aims to summarize the latest molecular mechanisms about pyroptosis mediated by pore-forming GSDMD and GSDME proteins that permeabilize plasma and mitochondrial membrane activating pyroptosis and apoptosis. We also discuss the potentiality of pyroptosis as a therapeutic target in human diseases. Blockade of pyroptosis by compounds can treat inflammatory disease and pyroptosis activation contributes to cancer therapy. Keywords: pyroptosis; GSDMD; GSDME; inflammatory disease; cancer therapy 1. Introduction Many disease states are cross-linked with cell death. The Nomenclature Committee on Cell Death make a series of recommendations to systematically classify cell death [1,2]. Programmed Cell Death (PCD) is mediated by specific cellular mechanisms and some signaling pathways are activated in these processes [3]. Apoptosis, autophagy and programmed necrosis are the three main types of PCD [4], and they may jointly determine the fate of malignant tumor cells. -

SENP7 Knockdown Inhibited Pyroptosis and NF-Κb/NLRP3
www.nature.com/scientificreports OPEN SENP7 knockdown inhibited pyroptosis and NF‑κB/NLRP3 infammasome pathway activation in Raw 264.7 cells Xun Li1, Fangzhou Jiao1, Jia Hong2, Fan Yang1, Luwen Wang1 & Zuojiong Gong 1* Pyroptosis is a kind of necrotic and infammatory programmed cell death induced by infammatory caspases. SENP7 is a SUMO‑specifc protease, which mainly acts on deconjugation of SUMOs from substrate proteins. We evaluated the efect of SENP7 knockdown on pyroptosis, NF‑κB signaling pathway, and NLRP3 infammasome in Raw 264.7 cells. The results showed that the GSDMD protein mainly expressed in the cytoplasm nearby nuclei of Raw 264.7 cells. It migrated to cytomembrane with the numbers of Raw 264.7 cell decreased when LPS + ATP were administrated. Which was inhibited by SENP7 knockdown. In addition, not only the pyroptosis of Raw 264.7 cells was inhibited, the activation of NF‑κB signaling pathway and NLRP3 infammasome were also attenuated by SENP7 knockdown. The mechanism may be associated with the over SUMOylation of proteins induced by SENP7 knockdown. Pyroptosis is a form of regulated cell death (RCD) with specifc morphological features including cell swelling and a specifc form of chromatin condensation, culminating with plasma membrane permeabilization 1,2. In contrast to apoptosis, pyroptosis is a kind of necrotic and infammatory programmed cell death induced by infammatory caspases3. It is regulated by caspase-1 dependent or caspase-1 independent mechanisms. In caspase-1-dependent manner, also known as canonical infammasome activation, Caspase-1 is activated by an infammasome initiation sensor that recognizes either cause-associated or risk-associated molecular patterns 3. -

Pyroptosis Versus Necroptosis: Similarities, Differences, and Crosstalk
Cell Death & Differentiation (2019) 26:99–114 https://doi.org/10.1038/s41418-018-0212-6 REVIEW ARTICLE Pyroptosis versus necroptosis: similarities, differences, and crosstalk 1,2 1,2 Daniel Frank ● James E. Vince Received: 9 June 2018 / Revised: 17 August 2018 / Accepted: 20 September 2018 / Published online: 19 October 2018 © ADMC Associazione Differenziamento e Morte Cellulare 2018 Pyroptosis and necroptosis represent two pathways of genetically encoded necrotic cell death. Although these cell death programmes can protect the host against microbial pathogens, their dysregulation has been implicated in a variety of autoimmune and auto-inflammatory conditions. The disease-promoting potential of necroptosis and pyroptosis is likely a consequence of their ability to induce a lytic cell death. This cell suicide mechanism, distinct from apoptosis, allows the release of immunogenic cellular content, including damage-associated molecular patterns (DAMPs), and inflammatory cytokines such as interleukin-1β (IL-1β), to trigger inflammation. In this Review, we discuss recent discoveries that have advanced our understanding on the primary functions of pyroptosis and necroptosis, including evidence for the specific cytokines and DAMPs responsible for driving inflammation. We compare the similar and unique aspects of pyroptotic- and necroptotic-induced membrane damage, and explore how these may functionally impact distinct intracellular organelles and signalling pathways. We also examine studies highlighting the crosstalk that can occur between necroptosis and pyroptosis 1234567890();,: 1234567890();,: signalling, and evidence supporting the physiological significance of this convergence. Ultimately, a better understanding of the similarities, unique aspects and crosstalk of pyroptosis and necroptosis will inform as to how these cell death pathways might be manipulated for therapeutic benefit. -

Priming Is Dispensable for Nlrp3 Inflammasome Activation in Human Monocytes
bioRxiv preprint doi: https://doi.org/10.1101/2020.01.30.925248; this version posted January 30, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. PRIMING IS DISPENSABLE FOR NLRP3 INFLAMMASOME ACTIVATION IN HUMAN MONOCYTES Anna Gritsenko1,2, Shi Yu1, Fatima Martin-Sanchez2, Ines Diaz del Olmo2, Eva-Maria Nichols3, Daniel M. Davis2, David Brough1, Gloria Lopez-Castejon2. 1. Lydia Becker Institute of Immunology and Inflammation, Division of Neuroscience and Experimental Psychology, Faculty of Biology, Medicine and Health, University of Manchester, Manchester Academic Health Science Centre, Manchester, UK 2. Lydia Becker Institute of Immunology and Inflammation, Manchester Collaborative Centre for Inflammation Research (MCCIR), Division of Infection, Immunity and Respiratory Medicine, Faculty of Biology, Medicine and Health, University of Manchester, Manchester Academic Health Science Centre, Manchester, UK 3. GSK Medicines Research Centre, Stevenage, UK ABSTRACT Interleukin (IL)-1 family of cytokines modulate immune responses during infection and inflammation. IL-18 and IL-1β are members of the IL-1 family, which contribute to inflammatory conditions such as rheumatoid arthritis and Alzheimer’s disease. IL-18 and IL-1β are produced as inactive precursors that are activated by large macromolecular complexes called inflammasomes upon sensing damage or pathogenic signals. Canonical NLRP3 inflammasome activation is regarded to require a priming step that causes NLRP3 and IL-1β gene upregulation, and also NLRP3 post- translational licencing. A subsequent activation step leads to the assembly of the inflammasome and the cleavage of pro-IL-18 and pro-IL-1β by caspase-1 into their mature forms, allowing their release. -

Pyroptosis: Physiological Roles in Viral Infection
1 Pyroptosis: Physiological roles in viral infection Nelson Durán1,2 and Wagner J. Fávaro1 ¹Laboratory of Urogenital Carcinogenesis and Immunotherapy, Department of Structural and Functional Biology, University of Campinas, Campinas, SP, Brazil, 2Nanomedicine Research Unit (Nanomed), Federal University of ABC (UFABC), Santo André, SP, Brazil. *Correspondence: Prof. Nelson Durán (E-mail: [email protected]) and Prof. Wagner J. Fávaro (E-mail: [email protected]). Abstract The current review focuses on important aspects of pyroptosis, such as morphological features of inflammasomes, as well as on knowledge about coronavirus infection mechanisms and the association between SARS-CoV-2 infection and cell pyroptosis. The application of immunomodulation therapies to Covid-19 patients is the most promising treatment under investigation nowadays. The possibilities of assistance to help protecting patients from infections are also addressed in the present study. Keywords: Pyroptosis, virus, Covid-19, SARS-CoV-2, inflammasomes, cytokines Highlights • Inflammatory caspases play an important role in innate immunity. • Pyroptosis eliminates the reproduction site of intracellular pathogens. • SARS-CoV proteins triggers NLRP3 inflammasome induction. • SARS-CoV-2 infection and cell pyroptosis. • Immunomodulation therapies to Covid-19 patients is the most promising treatment. 2 1. Introduction It is well known that inflammatory caspases play an important role in innate immunity by responding to cytosolic signals and by inducing a twofold response (Jorgensen and Miao, 2015). First, caspase-1 induces the activation and release of pro-inflammatory cytokines, such as interleukin-18 (IL-18) and IL-1β. Second, caspase-11 or caspase-1 can trigger a lytic, programmed cell death known as pyroptosis. Pyroptosis eliminates the reproduction site of intracellular pathogens, such as bacteria or virus, which makes them susceptible to phagocytosis and to be destroyed by secondary phagocytes. -

Critical Interactions Between Immunogenic Cancer Cell Death
Th eJournal of Brief Reviews Immunology Critical Interactions between Immunogenic Cancer Cell Death, Oncolytic Viruses, and the Immune System Define the Rational Design of Combination Immunotherapies ,1 †,‡,x,1 Jacob P. van Vloten,* x Samuel T. Workenhe, Sarah K. Wootton,* Karen L. Mossman,†,‡, ,2 and Byram W. Bridle*,2 Oncolytic viruses (OVs) are multimodal cancer thera- emphasis of cancer research is therapies that overcome im- peutics, with one of their dominant mechanisms munosuppression and tolerance to reawaken the immune being in situ vaccination. There is a growing consensus system to kill cancer cells. Immunogenic cell death (ICD) that optimal cancer therapies should generate robust engages multiple conserved cell death pathways, triggering tumor-specific immune responses. Immunogenic cell an immune response against tumor Ags and culminating in death (ICD) is a paradigm of cellular demise culminat- antitumor immunity (4). ing in the spatiotemporal release of danger-associated The engagement of overlapping, phylogenetically conserved molecular patterns that induce potent anticancer cell death pathways in ICD results in the spatiotemporal release immunity. Alongside traditional ICD inducers like of danger-associated molecular patterns (DAMPs) from dying anthracycline chemotherapeutics and radiation, OVs cells (5) (Fig. 1A). Critical DAMPs initiate responses by have emerged as novel members of this class of thera- attracting innate cells, particularly dendritic cells (DCs), to the tumor. DAMPs mature Ag-carrying DCs, endowing them peutics. OVs replicate in cancers and release tumor with the ability to activate tumor-specific T cells. Thus, ICD Ags, which are perceived as dangerous because of simul- is tied to the danger hypothesis (6), wherein factors produced taneous expression of pathogen-associated molecular by stressed and dying cells alert the immune system without patterns that activate APCs. -

Toll-Like Receptors
Toll-like Receptors TLR2/TLR6 TLR1/TLR2 TLR5 TLR4 TLR10 CD14 CD14 CD36 CD14 TIRAP TIRAP MD-2 MyD88 TIRAP MyD88 MyD88 TRAM MyD88 MyD88 TRIF Endosome TLR7 RIP1 IRAK4 IRAK1/2 TLR8 TLR9 TLR3 TRAF-6 TAB1/2 TAK1 TRAF-6 MyD88 MyD88 TRIF MyD88 TRAF-3 TRAF-3 TANK IKK IRF7 MKK RIP1 TBK1 Proteasome IKKε TAB1/2 IRF7 Homodimer TAK1 TRAF-6 TRAF-3 IκB Proteasome TANK IKK IκB IRF3 NFκB JNK IκB MKK p38 TBK1 IKKε IκB NFκB p38 JNK IRF7 IRF3 Homodimer IRF3 IRF7 Homodimer IRF3 Homodimer Toll-like Receptors Toll-like receptors are a family of type I transmembrane pattern recognition receptors (PRRs) that sense invading pathogens or endogenous damage signals and initiate the innate and adaptive immune response. There are ten functional TLRs in human (TLR1–10) and twelve in mice (TLR1−9, 11−13). Various combinations of TLRs are expressed by different subsets of immune and non-immune cell types such as monocytes, macrophages, dendritic cells, neutrophils, B cells, T cells, fibroblasts, endothelial cells, and epithelial cells. Of the human TLRs, TLR1, 2, 4, 5, 6, and 10 are expressed on the cell surface and primarily recognize microbial membrane and/or cell wall components, while TLR3, 7, 8, and 9 are expressed in the membranes of endolysosomal compartments and recognize nucleic acids. TLRs have a variable number of ligand- sensing, leucine-rich repeats (LRR) at their N-terminal ends and a cytoplasmic Toll/IL-1 R (TIR) domain. The TIR domain mediates interactions between TLRs and adaptor proteins involved in regulating TLR signaling including MyD88, TRIF, TRAM, and TIRAP/MAL. -
Apoptosis Vs Necrosis Cell Death
Apoptosis, Necrosis, Necroptosis & Pyroptosis By Sally Hed Dahlquist, President, BS, MBA October 20, 2020 © ImmunoChemistry Technologies LLC 2020 Agenda • Cell death is vital for life • Cells die differently • Accidental vs progammed cell death • Classification of cell death • Morphology • Caspases • TNFR1 death receptor • Key regulatory rolecules • Oncosis to necrosis • Necrosis • Necroptosis • Apoptosis • Pyroptosis • Detection Kits from ICT Sally Hed Dahlquist, President BS Genetics & Cell Biology, MBA Cell death is vital for life Good Bad Controlled Uncontrolled Cells die differently Pathways of cell death Necrosis & Oncosis Necroptosis Others: Anoikis Entosis Ferroptosis Methuosis Apoptosis Paraptosis Mitoptosis Parthanatos NETosis And more… Pyroptosis Programmed Regulated Cell Death (PCD or RCD) such as Apoptosis, etc; Good or Bad Not Programmed Accidental Cell Death (ACD) Necrosis & Oncosis; Bad; Uncontrolled Van Cruchten, S., & Van den Broeck, W. (2002). Morphological and Biochemical Aspects of Apoptosis, Oncosis and Necrosis. Anatomia, Histologia, Embryologia: Journal Of Veterinary Medicine Series C, 31(4), 214-223. doi:10.1046/j.1439-0264.2002.00398.x Classification Accidental Non- programmed Necrosis Not (Oncosis) regulated Programmed Cell death Apoptotic cell death Figure 1 from Yan, G., Elbadawi, M., & Efferth, T. (2020). Multiple cell death modalities and their key features (Review). World Academy of Sciences Journal, 2, 39-48. https://doi.org/10.3892/wasj.2020.40 Figure 2 from: Yan, G., Elbadawi, M., & Efferth, T. (2020). Multiple cell death modalities and their key features (Review). World Academy of Morphology Sciences Journal, 2, 39-48. https://doi.org/10.3892/wasj.2020.40 Non-programmed Programmed Necrosis (oncosis) Apoptosis Programmed Non-Apoptotic Cell Death Immune: Pyroptosis NETosis Programmed Non-Apoptotic Cell Death Vacuole: Autophagy Entosis Methuosis Paraptosis Mitochondria: Mitoptosis Parthanatos Iron: Ferroptosis Other: Necroptosis Control Adapted from Figure 1 of Xin Chen et al. -
The Role of Pyroptosis in Cancer: Pro-Cancer Or Pro-“Host”? Xiaojing Xia 1,Xinwang2, Zhe Cheng1,Wanhaiqin3, Liancheng Lei4,Jinqingjiang1 and Jianhe Hu1
Xia et al. Cell Death and Disease (2019) 10:650 https://doi.org/10.1038/s41419-019-1883-8 Cell Death & Disease REVIEW ARTICLE Open Access The role of pyroptosis in cancer: pro-cancer or pro-“host”? Xiaojing Xia 1,XinWang2, Zhe Cheng1,WanhaiQin3, Liancheng Lei4,JinqingJiang1 and Jianhe Hu1 Abstract Programmed cell death (PCD) refers to the way in which cells die depending on specific genes encoding signals or activities. Apoptosis, autophagy, and pyroptosis are all mechanisms of PCD. Among these mechanisms, pyroptosis is mediated by the gasdermin family, accompanied by inflammatory and immune responses. The relationship between pyroptosis and cancer is complex, and the effects of pyroptosis on cancer vary in different tissues and genetic backgrounds. On one hand, pyroptosis can inhibit the occurrence and development of tumors; on the other hand, as a type of proinflammatory death, pyroptosis can form a suitable microenvironment for tumor cell growth and thus promote tumor growth. In addition, the induction of tumor pyroptosis is also considered a potential cancer treatment strategy. Studies have shown that DFNA5 (nonsyndromic hearing impairment protein 5)/GSDME (Gasdermin-E) mRNA methylation results in lower expression levels of DFNA5/GSDME in most tumor cells than in normal cells, making it difficult to activate the pyroptosis in most tumor cells. During the treatment of malignant tumors, appropriate chemotherapeutic drugs can be selected according to the expression levels of DFNA5/GSDME, which can be upregulated in tumor cells, thereby increasing the sensitivity to chemotherapeutic drugs and reducing drug resistance. Therefore, induced pyroptosis may play a predominant role in the treatment of cancer. -
Pyroptosis - an Inflammatory Form of Regulated Cell Death Review
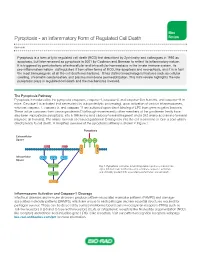
Mini Pyroptosis - an Inflammatory Form of Regulated Cell Death Review Overview Pyroptosis is a form of lytic regulated cell death (RCD) first described by Zychlinsky and colleagues in 1992 as apoptosis, but later renamed as pyroptosis in 2001 by Cookson and Brennan to reflect its inflammatory nature. It is triggered by perturbations of extracellular and intracellular homeostasis in the innate immune system. Its pro-inflammatory nature distinguishes it from other forms of RCD, like apoptosis and necroptosis, and it is in fact the most immunogenic of all the cell death mechanisms. It has distinct morphological features such as cellular swelling, chromatin condensation, and plasma membrane permeabilization. This mini-review highlights the role pyroptosis plays in regulated cell death and the mechanisms involved. The Pyroptosis Pathway Pyroptosis is mediated by the pyroptotic caspases, caspase-1, caspase-4, and caspase-5 in humans, and caspase-11 in mice. Caspase-1 is activated (not necessarily by autoproteolytic processing), upon activation of various inflammasomes, whereas caspase-4, caspase-5, and caspase-11 are activated upon direct binding of LPS from gram negative bacteria. These active caspases then cleave gasdermin D (although more recently other members of the gasdermin family have also been implicated in pyroptosis), into a 199 amino acid carboxy-terminal fragment and a 242 amino acid amino-terminal fragment (in humans). The amino-terminal of cleaved gasdermin D integrates into the cell membrane to form a pore which directly leads to cell death. A simplified overview of the pyroptosis pathway is shown in Figure 1. PyroptosisPyroptosis ExtracellularExtracellular Space Space + IL-1ß Na H20 Nigericin PAMPS D min D sdermin sder Ga Ga Intracellular NLPR3 NLRC4 AIM2 Space Intracellular Space Pro-Caspase-1 Fig. -

Pyroptosis and Neurological Diseases
Review Article Pyroptosis and neurological diseases Zhen Xie1,2, Gang Zhao1 1Department of Neurology, Xijing Hospital, Forth Military Medical University, Xi’an 710032, Shaanxi, China 2Department of Neurology, Shaanxi Provincial People’s Hospital, Xi’an 710068, Shaanxi, China ABSTRACT Pyroptosis is a new process of programmed cell death, which has been discovered and confirmed in recent years. Its cardinal features include activation of caspase‑1 and a massive release of inflammatory cytokines (interleukin (IL)‑1β, IL‑18), etc. The morphological characteristics, occurrence and regulatory mechanisms of the pyroptosis greatly, differ from other cell death mechanisms such as apoptosis and necrosis. It has already been proven that pyroptosis participates and plays an important role in a wide range of neuronal diseases. Here, we review the current understanding of the pyroptosis and its roles in neurological diseases. Key words: Caspase-1, inflammasome, interleukin-1β, interleukin‑18, neurological diseases, pyroptosis INTRODUCTION Pyroptosis was first observed in 1992 when Zychlinsky et al. described that Shigella flexneri can induce Cell death is a critical and inevitable phase common programmed cell death in macrophage, but this process to all cell types. A deeper understanding of cell death was mediated by a caspase-1, and the iconic molecule in its form and nature is critical to shed new light in apoptosis, caspase-3, was not apparently involved. on the emergence, development and treatment of This observation suggested that such programmed diseases. Many different types of cell death patterns cell death was different from apoptosis.[1] Subsequent have been discovered in the last years; among that studies confirmed that in S.