Identification of Compound Heterozygous Variants in The
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Coding RNA Genes
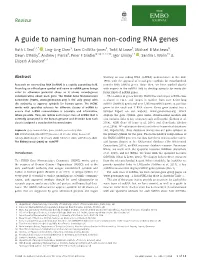
Review A guide to naming human non-coding RNA genes Ruth L Seal1,2,* , Ling-Ling Chen3, Sam Griffiths-Jones4, Todd M Lowe5, Michael B Mathews6, Dawn O’Reilly7, Andrew J Pierce8, Peter F Stadler9,10,11,12,13, Igor Ulitsky14 , Sandra L Wolin15 & Elspeth A Bruford1,2 Abstract working on non-coding RNA (ncRNA) nomenclature in the mid- 1980s with the approval of initial gene symbols for mitochondrial Research on non-coding RNA (ncRNA) is a rapidly expanding field. transfer RNA (tRNA) genes. Since then, we have worked closely Providing an official gene symbol and name to ncRNA genes brings with experts in the ncRNA field to develop symbols for many dif- order to otherwise potential chaos as it allows unambiguous ferent kinds of ncRNA genes. communication about each gene. The HUGO Gene Nomenclature The number of genes that the HGNC has named per ncRNA class Committee (HGNC, www.genenames.org) is the only group with is shown in Fig 1, and ranges in number from over 4,500 long the authority to approve symbols for human genes. The HGNC ncRNA (lncRNA) genes and over 1,900 microRNA genes, to just four works with specialist advisors for different classes of ncRNA to genes in the vault and Y RNA classes. Every gene symbol has a ensure that ncRNA nomenclature is accurate and informative, Symbol Report on our website, www.genenames.org, which where possible. Here, we review each major class of ncRNA that is displays the gene symbol, gene name, chromosomal location and currently annotated in the human genome and describe how each also includes links to key resources such as Ensembl (Zerbino et al, class is assigned a standardised nomenclature. -

Diagnostic Interpretation of Genetic Studies in Patients with Primary
AAAAI Work Group Report Diagnostic interpretation of genetic studies in patients with primary immunodeficiency diseases: A working group report of the Primary Immunodeficiency Diseases Committee of the American Academy of Allergy, Asthma & Immunology Ivan K. Chinn, MD,a,b Alice Y. Chan, MD, PhD,c Karin Chen, MD,d Janet Chou, MD,e,f Morna J. Dorsey, MD, MMSc,c Joud Hajjar, MD, MS,a,b Artemio M. Jongco III, MPH, MD, PhD,g,h,i Michael D. Keller, MD,j Lisa J. Kobrynski, MD, MPH,k Attila Kumanovics, MD,l Monica G. Lawrence, MD,m Jennifer W. Leiding, MD,n,o,p Patricia L. Lugar, MD,q Jordan S. Orange, MD, PhD,r,s Kiran Patel, MD,k Craig D. Platt, MD, PhD,e,f Jennifer M. Puck, MD,c Nikita Raje, MD,t,u Neil Romberg, MD,v,w Maria A. Slack, MD,x,y Kathleen E. Sullivan, MD, PhD,v,w Teresa K. Tarrant, MD,z Troy R. Torgerson, MD, PhD,aa,bb and Jolan E. Walter, MD, PhDn,o,cc Houston, Tex; San Francisco, Calif; Salt Lake City, Utah; Boston, Mass; Great Neck and Rochester, NY; Washington, DC; Atlanta, Ga; Rochester, Minn; Charlottesville, Va; St Petersburg, Fla; Durham, NC; Kansas City, Mo; Philadelphia, Pa; and Seattle, Wash AAAAI Position Statements,Work Group Reports, and Systematic Reviews are not to be considered to reflect current AAAAI standards or policy after five years from the date of publication. The statement below is not to be construed as dictating an exclusive course of action nor is it intended to replace the medical judgment of healthcare professionals. -

University of Groningen Unravelling the Genetic Basis of Hereditary
University of Groningen Unravelling the genetic basis of hereditary disorders by high-throughput exome sequencing strategies Jazayeri, Omid IMPORTANT NOTE: You are advised to consult the publisher's version (publisher's PDF) if you wish to cite from it. Please check the document version below. Document Version Publisher's PDF, also known as Version of record Publication date: 2016 Link to publication in University of Groningen/UMCG research database Citation for published version (APA): Jazayeri, O. (2016). Unravelling the genetic basis of hereditary disorders by high-throughput exome sequencing strategies. University of Groningen. Copyright Other than for strictly personal use, it is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s), unless the work is under an open content license (like Creative Commons). The publication may also be distributed here under the terms of Article 25fa of the Dutch Copyright Act, indicated by the “Taverne” license. More information can be found on the University of Groningen website: https://www.rug.nl/library/open-access/self-archiving-pure/taverne- amendment. Take-down policy If you believe that this document breaches copyright please contact us providing details, and we will remove access to the work immediately and investigate your claim. Downloaded from the University of Groningen/UMCG research database (Pure): http://www.rug.nl/research/portal. For technical reasons the number of authors shown on this cover page is limited to 10 maximum. Download date: 07-10-2021 Unravelling the genetic basis of hereditary disorders by high-throughput exome sequencing strategies Omid Jazayeri | Omid Jazayeri Unravelling the genetic basis of hereditary disorders by high-throughput exome sequencing strategies The research presented in this thesis was performed at the Department of Genetics, Uiversity Medical Center Groningen, University of Groningen, Groningen, The Netherlands. -
Methods for Determining the Genetic Causes of Rare Diseases
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Apollo Methods for Determining the Genetic Causes of Rare Diseases Daniel Greene MRC Biostatistics Unit University of Cambridge This dissertation is submitted for the degree of Doctor of Philosophy Clare College January 2018 Methods for Determining the Genetic Causes of Rare Diseases Daniel Greene Thanks to the affordability of DNA sequencing, hundreds of thousands of individuals with rare disorders are undergoing whole-genome sequencing in an effort to reveal novel disease aetiologies, increase our understanding of biological processes and improve patient care. However, the power to discover the genetic causes of many unexplained rare diseases is hindered by a paucity of cases with a shared molecular aetiology. This thesis presents research into statistical and computational methods for determining the genetic causes of rare diseases. Methods described herein treat important aspects of the nature of rare diseases, including genetic and phenotypic heterogeneity, phenotypes involving multiple organ systems, Mendelian modes of inheritance and the incorporation of complex prior information such as model organism phenotypes and evolutionary conservation. The complex nature of rare disease phenotypes and the need to aggregate patient data across many centres has led to the adoption of the Human Phenotype Ontology (HPO) as a means of coding patient phenotypes. The HPO provides a standardised vocabulary and captures relationships between disease features. The use of such ontologically encoded data is widespread in bioinformatics, with ontologies defining relationships between concepts in hundreds of subfields. However, there has been a dearth of tools for manipulating and analysing ontological data. -

Compound Heterozygous Mutations in the Noncoding RNU4ATAC Cause Roifman Syndrome by Disrupting Minor Intron Splicing
ARTICLE Received 2 Feb 2015 | Accepted 25 Sep 2015 | Published 2 Nov 2015 DOI: 10.1038/ncomms9718 OPEN Compound heterozygous mutations in the noncoding RNU4ATAC cause Roifman Syndrome by disrupting minor intron splicing Daniele Merico1,*, Maian Roifman2,3,4,*, Ulrich Braunschweig5,RyanK.C.Yuen1, Roumiana Alexandrova1, Andrea Bates6, Brenda Reid6, Thomas Nalpathamkalam1,ZhuozhiWang1, Bhooma Thiruvahindrapuram1, Paul Gray7, Alyson Kakakios8, Jane Peake9,10, Stephanie Hogarth9,10,DavidManson11, Raymond Buncic12, Sergio L. Pereira1, Jo-Anne Herbrick1,BenjaminJ.Blencowe5,13,ChaimM.Roifman4,6 &StephenW.Scherer1,13,14,15 Roifman Syndrome is a rare congenital disorder characterized by growth retardation, cognitive delay, spondyloepiphyseal dysplasia and antibody deficiency. Here we utilize whole-genome sequencing of Roifman Syndrome patients to reveal compound heterozygous rare variants that disrupt highly conserved positions of the RNU4ATAC small nuclear RNA gene, a minor spliceosome component that is essential for minor intron splicing. Targeted sequencing confirms allele segregation in six cases from four unrelated families. RNU4ATAC rare variants have been recently reported to cause microcephalic osteodysplastic primordial dwarfism, type I (MOPD1), whose phenotype is distinct from Roifman Syndrome. Strikingly, all six of the Roifman Syndrome cases have one variant that overlaps MOPD1-implicated structural elements, while the other variant overlaps a highly conserved structural element not previously implicated in disease. RNA-seq analysis confirms extensive and specific defects of minor intron splicing. Available allele frequency data suggest that recessive genetic disorders caused by RNU4ATAC rare variants may be more prevalent than previously reported. 1 The Centre for Applied Genomics (TCAG), Program in Genetics and Genome Biology, The Hospital for Sick Children, Toronto, Ontario, Canada M5G 0A4. -
Minor Class Splicing Shapes the Zebrafish Transcriptome During Development
Minor class splicing shapes the zebrafish transcriptome during development Sebastian Markmillera,b,1, Nicole Cloonanc,2,3, Rea M. Lardellia,2,4, Karen Doggettd,e, Maria-Cristina Keightleyf, Yeliz Bogleva, Andrew J. Trottera, Annie Y. Nga,5, Simon J. Wilkinsc, Heather Verkadea,g, Elke A. Oberg,6, Holly A. Fieldg, Sean M. Grimmondc, Graham J. Lieschkef, Didier Y. R. Stainierg,7, and Joan K. Heatha,b,d,e,8 aLudwig Institute for Cancer Research, Melbourne-Parkville Branch, Parkville, VIC 3050, Australia; bDepartment of Surgery, Royal Melbourne Hospital, University of Melbourne, Parkville, VIC 3050, Australia; cQueensland Centre for Medical Genomics, Institute for Molecular Bioscience, University of Queensland, St. Lucia, QLD 4072, Australia; dWalter and Eliza Hall Institute of Medical Research, Parkville, VIC 3052, Australia; eDepartment of Medical Biology, University of Melbourne, Parkville, VIC 3052, Australia; fAustralian Regenerative Medicine Institute, Monash University, Clayton, VIC 3800, Australia; and gDepartment of Biochemistry and Biophysics, University of California, San Francisco, CA 94158 Edited* by Joan A. Steitz, Howard Hughes Medical Institute, New Haven, CT, and approved January 16, 2014 (received for review March 31, 2013) Minor class or U12-type splicing is a highly conserved process splicing pathway has been an intriguing aspect of gene ex- required to remove a minute fraction of introns from human pre- pression. Interestingly, U12-type introns are nonrandomly dis- mRNAs. Defects in this splicing pathway have recently been linked to tributed across the genome (11) and their removal is thought to human disease, including a severe developmental disorder encom- be rate-limiting in the generation of mature mRNAs (12–14). -

A Homozygous Mutation in the Stem II Domain of RNU4ATAC Causes Typical Roifman Syndrome
www.nature.com/npjgenmed CASE REPORT OPEN A homozygous mutation in the stem II domain of RNU4ATAC causes typical Roifman syndrome Yael Dinur Schejter1,2, Adi Ovadia1,2, Roumiana Alexandrova3, Bhooma Thiruvahindrapuram3, Sergio L. Pereira3, David E. Manson4, Ajoy Vincent5, Daniele Merico3,6 and Chaim M. Roifman1,2 Roifman syndrome (OMIM# 616651) is a complex syndrome encompassing skeletal dysplasia, immunodeficiency, retinal dystrophy and developmental delay, and is caused by compound heterozygous mutations involving the Stem II region and one of the other domains of the RNU4ATAC gene. This small nuclear RNA gene is essential for minor intron splicing. The Canadian Centre for Primary Immunodeficiency Registry and Repository were used to derive patient information as well as tissues. Utilising RNA sequencing methodologies, we analysed samples from patients with Roifman syndrome and assessed intron retention. We demonstrate that a homozygous mutation in Stem II is sufficient to cause the full spectrum of features associated with typical Roifman syndrome. Further, we demonstrate the same pattern of aberration in minor intron retention as found in cases with compound heterozygous mutations. npj Genomic Medicine (2017) 2:23 ; doi:10.1038/s41525-017-0024-5 INTRODUCTION from Roifman syndrome, typically presenting early in life with a Roifman syndrome (OMIM# 616651) was first identified as a novel high pre-natal and post-natal lethality, major structural brain association of immunodeficiency, spondyloepiphyseal dysplasia, malformations, neuroendocrine dysfunction, very short and developmental delay, retinal dystrophy and unique facial dys- bowed limbs as well as dysmorphic features including proptotic morphic features.1, 2 Additional features, such as autoimmune eyes, prominent nose and micrognathia. -

And Super Elongation Complex (Sec) As Regulators of Tdp-43-Associated Neurodegeneration
University of Pennsylvania ScholarlyCommons Publicly Accessible Penn Dissertations 2018 Little Elongation Complex (lec) And Super Elongation Complex (sec) As Regulators Of Tdp-43-Associated Neurodegeneration Chia-Yu Chung University of Pennsylvania, [email protected] Follow this and additional works at: https://repository.upenn.edu/edissertations Part of the Biology Commons, Cell Biology Commons, and the Neuroscience and Neurobiology Commons Recommended Citation Chung, Chia-Yu, "Little Elongation Complex (lec) And Super Elongation Complex (sec) As Regulators Of Tdp-43-Associated Neurodegeneration" (2018). Publicly Accessible Penn Dissertations. 3102. https://repository.upenn.edu/edissertations/3102 This paper is posted at ScholarlyCommons. https://repository.upenn.edu/edissertations/3102 For more information, please contact [email protected]. Little Elongation Complex (lec) And Super Elongation Complex (sec) As Regulators Of Tdp-43-Associated Neurodegeneration Abstract TDP-43 aggregation is the pathological hallmark of amyotrophic lateral sclerosis (ALS) and frontotemporal lobar degeneration with ubiquitinated inclusions (FTLD-TDP). To define pathways important in TDP-43 proteinopathy, a genetic screen for modifiers of TDP-43-mediated ye e degeneration was conducted in the fruit fly (Drosophila melanogaster). This approach and the following studies in the fly identified anscriptionaltr elongation factor Ell as a potent dose-dependent modifier. Ell is a shared component of little elongation complex (LEC) and super elongation complex (SEC). Our studies show that downregulation of additional components in LEC or SEC partially but consistently ameliorates TDP-43-associated eye degeneration, implicating both Ell-associated complexes in TDP-43 toxicity. LEC regulates transcription of RNA Polymerase II (Pol II)-transcribed small nuclear RNAs (snRNAs), while SEC mainly regulates transcription of select inducible genes harboring paused Pol II including stress-induced loci. -

International Growth List
! Preface Causes of Disrupons in Children’s Growth Scienfic Evidence Advancements in technology, clinical research, and high speed informa'on sharing have collec'vely facilitated the discovery of an unprecedented amount of informa'on pertaining to the gene'c causes of children’s growth failure, overgrowth or other growth irregulari'es. For decades, scien'sts have been mapping out the millions of human gene'c details in discovery. During this process they iden'fied diseases/syndromes which are apparent in a child who displays all of the characteris'cs (“classic” form) of that syndrome. Other children may have the same syndrome but in a “par'al” form. There are typically mul'ple varie'es of the par'al forms. It is a complicated discovery and cataloguing process which con'nues to this day. The varia'on of characteris'cs within each syndrome means that growth irregulari'es may be the result of a variety of mechanisms. As you will note in the categories within this document, some children have issues which are (non-syndromic) and do not yet have a “name” but have a list of characteris'cs of which growth is listed as a condi'on. Therefore, those “un-named” syndromes are listed in the Alphabe'cal list contained herein. What does this increase in knowledge do for families and growth affected children? Poten'ally, gene'c explana'ons can afford physicians an opportunity to iden'fy causes for growth failure or overgrowth at a much younger age. If treatments are available for the iden'fied medical cause, ini'a'ng therapies as soon as possible could change the child’s future and health for his/her en're life'me.