Amyand Hernia Repair with Mesh and Appendectomy Katelin Holmes1* and Joseph E
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Utility of the Digital Rectal Examination in the Emergency Department: a Review
The Journal of Emergency Medicine, Vol. 43, No. 6, pp. 1196–1204, 2012 Published by Elsevier Inc. Printed in the USA 0736-4679/$ - see front matter http://dx.doi.org/10.1016/j.jemermed.2012.06.015 Clinical Reviews UTILITY OF THE DIGITAL RECTAL EXAMINATION IN THE EMERGENCY DEPARTMENT: A REVIEW Chad Kessler, MD, MHPE*† and Stephen J. Bauer, MD† *Department of Emergency Medicine, Jesse Brown VA Medical Center and †University of Illinois-Chicago College of Medicine, Chicago, Illinois Reprint Address: Chad Kessler, MD, MHPE, Department of Emergency Medicine, Jesse Brown Veterans Hospital, 820 S Damen Ave., M/C 111, Chicago, IL 60612 , Abstract—Background: The digital rectal examination abdominal pain and acute appendicitis. Stool obtained by (DRE) has been reflexively performed to evaluate common DRE doesn’t seem to increase the false-positive rate of chief complaints in the Emergency Department without FOBTs, and the DRE correlated moderately well with anal knowing its true utility in diagnosis. Objective: Medical lit- manometric measurements in determining anal sphincter erature databases were searched for the most relevant arti- tone. Published by Elsevier Inc. cles pertaining to: the utility of the DRE in evaluating abdominal pain and acute appendicitis, the false-positive , Keywords—digital rectal; utility; review; Emergency rate of fecal occult blood tests (FOBT) from stool obtained Department; evidence-based medicine by DRE or spontaneous passage, and the correlation be- tween DRE and anal manometry in determining anal tone. Discussion: Sixteen articles met our inclusion criteria; there INTRODUCTION were two for abdominal pain, five for appendicitis, six for anal tone, and three for fecal occult blood. -

The Differences Between ICD-9 and ICD-10
Preparing for the ICD-10 Code Set: Fact Sheet 2 October 1, 2015 Compliance Date Get the Facts to be Compliant Alert: The new ICD-10 compliance date is October 1, 2015. The Differences Between ICD-9 and ICD-10 This is the second fact sheet in a series and is focused on the differences between the ICD-9 and ICD-10 code sets. Collectively, the fact sheets will provide information, guidance, and checklists to assist you with understanding what you need to do to implement the ICD-10 code set. The ICD-10 code sets are not a simple update of the ICD-9 code set. The ICD-10 code sets have fundamental changes in structure and concepts that make them very different from ICD-9. Because of these differences, it is important to develop a preliminary understanding of the changes from ICD-9 to ICD-10. This basic understanding of the differences will then identify more detailed training that will be needed to appropriately use the ICD-10 code sets. In addition, seeing the differences between the code sets will raise awareness of the complexities of converting to the ICD-10 codes. Overall Comparisons of ICD-9 to ICD-10 Issues today with the ICD-9 diagnosis and procedure code sets are addressed in ICD-10. One concern today with ICD-9 is the lack of specificity of the information conveyed in the codes. For example, if a patient is seen for treatment of a burn on the right arm, the ICD-9 diagnosis code does not distinguish that the burn is on the right arm. -
Appendectomy: Simple Appendicitis
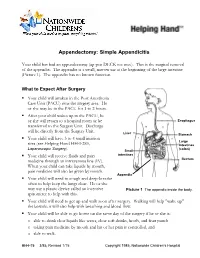
Appendectomy: Simple Appendicitis Your child has had an appendectomy (ap pen DECK toe mee). This is the surgical removal of the appendix. The appendix is a small, narrow sac at the beginning of the large intestine (Picture 1). The appendix has no known function. What to Expect After Surgery . Your child will awaken in the Post Anesthesia Care Unit (PACU) near the surgery area. He or she may be in the PACU for 1 to 2 hours. After your child wakes up in the PACU, he or she will return to a hospital room or be Esophagus transferred to the Surgery Unit. Discharge will be directly from the Surgery Unit. Liver Stomach . Your child will have 3 to 4 small incision Large sites (see Helping Hand HH-I-283, Intestines Laparoscopic Surgery (colon) ). Small . Your child will receive fluids and pain intestines medicine through an intravenous line (IV). Rectum When your child can take liquids by mouth, pain medicine will also be given by mouth. Appendix . Your child will need to cough and deep-breathe often to help keep the lungs clear. He or she may use a plastic device called an incentive Picture 1 The appendix inside the body. spirometer to help with this. Your child will need to get up and walk soon after surgery. Walking will help "wake up" the bowels; it will also help with breathing and blood flow. Your child will be able to go home on the same day of the surgery if he or she is: o able to drink clear liquids like water, clear soft drinks, broth, and fruit punch o taking pain medicine by mouth and his or her pain is controlled, and o able to walk. -

Laparoscopy in Emergency Hernia Repair
Review Article Page 1 of 11 Laparoscopy in emergency hernia repair George P.C. Yang Department of Surgery, Hong Kong Adventist Hospital, Hong Kong, China Correspondence to: George Pei Cheung Yang, FRACS. Department of Surgery, Hong Kong Adventist Hospital, 40 Stubbs Road, Hong Kong, China. Email: [email protected]. Abstract: Minimal access surgery (MAS) or laparoscopic surgery has revolutionized our surgical world since its introduction in the 1980s. Its benefits of faster recovery, lesser wound pain which in turn reduced respiratory complications, allows earlier mobilization, minimize deep vein thrombosis, minimize wound infection rate are well reported and accepted. It also has significant long-term benefits which are often neglected by many, such as reduced risk of incisional hernia and lesser risk of intestinal obstruction from post-operative bowel adhesion. The continuous development and improvement in laparoscopic equipment and instruments, together with the better understanding of laparoscopic anatomy and refinement of laparoscopic surgical techniques, has enable laparoscopic surgery to evolve further. The evolution allows its application to include not only elective conditions, but also emergency surgical conditions. Performing laparoscopy and laparoscopic procedure under surgical emergencies require extra cautions. These procedures should be performed by expert in these fields together with experienced supporting staffs and the availability of appropriate equipment and instruments. Laparoscopic management for emergency groin hernia conditions has been reported by centers expert in laparoscopic hernia surgery. However, laparoscopy in emergency hernia repair includes a wide variety of meanings. Often in the different reports series one will see different meanings for laparoscopic repair and open conversion when reading in details. -
Laparoscopic Totally Extraperitoneal Inguinal Hernia Repair: Lessons Learned from 3,100 Hernia Repairs Over 15 Years
Surg Endosc (2009) 23:482–486 DOI 10.1007/s00464-008-0118-3 Laparoscopic totally extraperitoneal inguinal hernia repair: lessons learned from 3,100 hernia repairs over 15 years Jean-Louis Dulucq Æ Pascal Wintringer Æ Ahmad Mahajna Received: 30 November 2007 / Accepted: 14 July 2008 / Published online: 23 September 2008 Ó Springer Science+Business Media, LLC 2008 Abstract Mean operative time was 17 min in unilateral hernia and Background Two revolutions in inguinal hernia repair 24 min in bilateral hernia. There were 36 hernias (1.2%) surgery have occurred during the last two decades. The first that required conversion: 12 hernias were converted to was the introduction of tension-free hernia repair by open anterior Liechtenstein and 24 to laparoscopic TAPP Liechtenstein in 1989 and the second was the application of technique. The incidence of intraoperative complications laparoscopic surgery to the treatment of inguinal hernia in was low. Most of the patients were discharged at the sec- the early 1990s. The purposes of this study were to assess ond day of the surgery. The overall postoperative morbidity the safety and effectiveness of laparoscopic totally extra- rate was 2.2%. The incidence of recurrence rate was peritoneal (TEP) repair and to discuss the technical changes 0.35%. The recurrence rate for the first 200 repairs was that we faced on the basis of our accumulative experience. 2.5%, but it decreased to 0.47% for the subsequent 1,254 Methods Patients who underwent an elective inguinal hernia repairs hernia repair at the Department of Abdominal Surgery at Conclusion According to our experience, in the hands of the Institute of Laparoscopic Surgery (ILS), Bordeaux, experienced laparoscopic surgeons, laparoscopic hernia between June 1990 and May 2005 were enrolled retro- repair seems to be the favored approach for most types of spectively in this study. -

Ventral Hernia Repair
AMERICAN COLLEGE OF SURGEONS • DIVISION OF EDUCATION Ventral Hernia Repair Benefits and Risks of Your Operation Patient Education B e n e fi t s — An operation is the only This educational information is way to repair a hernia. You can return to help you be better informed to your normal activities and, in most about your operation and cases, will not have further discomfort. empower you with the skills and Risks of not having an operation— knowledge needed to actively The size of your hernia and the pain it participate in your care. causes can increase. If your intestine becomes trapped in the hernia pouch, you will have sudden pain and vomiting Keeping You Common Sites for Ventral Hernia and require an immediate operation. Informed If you decide to have the operation, Information that will help you possible risks include return of the further understand your operation The Condition hernia; infection; injury to the bladder, and your role in healing. A ventral hernia is a bulge through blood vessels, or intestines; and an opening in the muscles on the continued pain at the hernia site. Education is provided on: abdomen. The hernia can occur at a Hernia Repair Overview .................1 past incision site (incisional), above the navel (epigastric), or other weak Condition, Symptoms, Tests .........2 Expectations muscle sites (primary abdominal). Treatment Options….. ....................3 Before your operation—Evaluation may include blood work, urinalysis, Risks and Common Symptoms Possible Complications ..................4 ultrasound, or a CT scan. Your surgeon ● Visible bulge on the abdomen, and anesthesia provider will review Preparation especially with coughing or straining your health history, home medications, and Expectations .............................5 ● Pain or pressure at the hernia site and pain control options. -
RELATIVE VALUE UNITS (RVUS) and RELATED INFORMATION—Continued
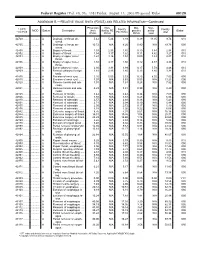
Federal Register / Vol. 68, No. 158 / Friday, August 15, 2003 / Proposed Rules 49129 ADDENDUM B.—RELATIVE VALUE UNITS (RVUS) AND RELATED INFORMATION—Continued Physician Non- Mal- Non- 1 CPT/ Facility Facility 2 MOD Status Description work facility PE practice acility Global HCPCS RVUs RVUs PE RVUs RVUs total total 42720 ....... ........... A Drainage of throat ab- 5.42 5.24 3.93 0.39 11.05 9.74 010 scess. 42725 ....... ........... A Drainage of throat ab- 10.72 N/A 8.26 0.80 N/A 19.78 090 scess. 42800 ....... ........... A Biopsy of throat ................ 1.39 2.35 1.45 0.10 3.84 2.94 010 42802 ....... ........... A Biopsy of throat ................ 1.54 3.17 1.62 0.11 4.82 3.27 010 42804 ....... ........... A Biopsy of upper nose/ 1.24 3.16 1.54 0.09 4.49 2.87 010 throat. 42806 ....... ........... A Biopsy of upper nose/ 1.58 3.17 1.66 0.12 4.87 3.36 010 throat. 42808 ....... ........... A Excise pharynx lesion ...... 2.30 3.31 1.99 0.17 5.78 4.46 010 42809 ....... ........... A Remove pharynx foreign 1.81 2.46 1.40 0.13 4.40 3.34 010 body. 42810 ....... ........... A Excision of neck cyst ........ 3.25 5.05 3.53 0.25 8.55 7.03 090 42815 ....... ........... A Excision of neck cyst ........ 7.07 N/A 5.63 0.53 N/A 13.23 090 42820 ....... ........... A Remove tonsils and ade- 3.91 N/A 3.63 0.28 N/A 7.82 090 noids. -

Incidental Drainage of a Periappendicular Abscess During Colonoscopy
UCTN – Unusual cases and technical notes E175 Incidental drainage of a periappendicular abscess during colonoscopy A 50-year-old man was referred to the of oral metronidazole and ciprofloxacin. A P. Figueiredo, V. Fernandes, J. Freitas outpatient colonoscopy clinic after a posi- computed tomography (CT) scan 1 week Department of Gastroenterology, tive fecal occult blood test during screen- after the procedure revealed no abnormal Hospital Garcia de Orta, Almada, Portugal ing for colorectal cancer. Colonoscopy, findings and the patient remained asymp- which was performed with the patient tomatic. sedated, revealed a 12-mm tumor covered Acute appendicitis is the most frequent References by normal, smooth mucosa at the site of acute abdominal emergency seen in de- 1 Oliak D, Yamini D, Udani VM et al. Can per- forated appendicitis be diagnosed preopera- the appendicular orifice. A biopsy was veloped countries. Its most common com- tively based on admission factors? J Gastro- taken, but this led to an immediate puru- plication is perforation and this may be intest Surg 2000; 4: 470–474 lent discharge occurring from the lesion followed by abscess formation [1]. Colo- 2 Ohtaka M, Asakawa A, Kashiwagi A et al. (●" Video 1). Therefore, a diagnosis of a noscopic diagnosis and treatment of a Pericecal appendiceal abscess with drainage periappendicular abscess was incidentally periappendicular abscess is rare [2]. In during colonoscopy. Gastrointest Endosc 1999; 49: 107–109 established. this case a periappendicular abscess was 3 Antevil J, Brown C. Percutaneous drainage After the patient had recovered from the incidentally discovered and drained dur- and interval appendectomy. In: Scott-Turner sedation, he was specifically questioned ing a colonoscopy. -

Immune Functions of the Vermiform Appendix
The Proceedings of the International Conference on Creationism Volume 3 Print Reference: Pages 335-342 Article 30 1994 Immune Functions of the Vermiform Appendix Frank Maas Follow this and additional works at: https://digitalcommons.cedarville.edu/icc_proceedings DigitalCommons@Cedarville provides a publication platform for fully open access journals, which means that all articles are available on the Internet to all users immediately upon publication. However, the opinions and sentiments expressed by the authors of articles published in our journals do not necessarily indicate the endorsement or reflect the views of DigitalCommons@Cedarville, the Centennial Library, or Cedarville University and its employees. The authors are solely responsible for the content of their work. Please address questions to [email protected]. Browse the contents of this volume of The Proceedings of the International Conference on Creationism. Recommended Citation Maas, Frank (1994) "Immune Functions of the Vermiform Appendix," The Proceedings of the International Conference on Creationism: Vol. 3 , Article 30. Available at: https://digitalcommons.cedarville.edu/icc_proceedings/vol3/iss1/30 IMMUNE FUNCTIONS OF THE VERMIFORM APPENDIX FRANK MAAS, M.S. 320 7TH STREET GERVAIS, OR 97026 KEYWORDS Mucosal immunology, gut-associated lymphoid tissues. immunocompetence, appendix (human and rabbit), appendectomy, neoplasm, vestigial organs. ABSTRACT The vermiform appendix Is purported to be the classic example of a vestigial organ, yet for nearly a century it has been known to be a specialized organ highly infiltrated with lymphoid tissue. This lymphoid tissue may help protect against local gut infections. As the vertebrate taxonomic scale increases, the lymphoid tissue of the large bowel tends to be concentrated In a specific region of the gut: the cecal apex or vermiform appendix. -
Appendicitis
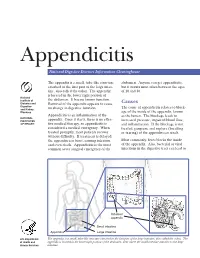
Appendicitis National Digestive Diseases Information Clearinghouse The appendix is a small, tube-like structure abdomen. Anyone can get appendicitis, attached to the first part of the large intes- but it occurs most often between the ages tine, also called the colon. The appendix of 10 and 30. is located in the lower right portion of National Institute of the abdomen. It has no known function. Diabetes and Removal of the appendix appears to cause Causes Digestive The cause of appendicitis relates to block- and Kidney no change in digestive function. Diseases age of the inside of the appendix, known Appendicitis is an inflammation of the as the lumen. The blockage leads to NATIONAL INSTITUTES appendix. Once it starts, there is no effec- increased pressure, impaired blood flow, OF HEALTH tive medical therapy, so appendicitis is and inflammation. If the blockage is not considered a medical emergency. When treated, gangrene and rupture (breaking treated promptly, most patients recover or tearing) of the appendix can result. without difficulty. If treatment is delayed, the appendix can burst, causing infection Most commonly, feces blocks the inside and even death. Appendicitis is the most of the appendix. Also, bacterial or viral common acute surgical emergency of the infections in the digestive tract can lead to Inflamed appendix Small intestine Appendix Large intestine U.S. Department The appendix is a small, tube-like structure attached to the first part of the large intestine, also called the colon. The of Health and appendix is located in the lower right portion of the abdomen, near where the small intestine attaches to the large Human Services intestine. -

Office Brochure-2
COLOPROCTOLOGY ASSOCIATES, PA COLONRECTAL SURGERY HERNIA REPAIR CENTER FOR PRECISION PROCTOLOGY Over the last 20 years, we have striven for one thing above quality service and care.. TRUST... Our patients usually leave our offices with a secure feeling, confident that their problems will be addressed in an Marcus Michael Aquino, honest and cost efficient attempt at successful MD, FACS, FRCS, FASCRS resolution. They realize that Dr. Aquino approaches ColonRectal Surgeon the patient's symptoms and signs as a good detective methodically analyzes a crime scene, looking for a Born and raised in Bangalore, South India, Marcus reason behind every one, and grouping them into a completed his basic surgical training in the United Kingdom unifying diagnosis when possible. before immigrating to the United States of America, where he underwent a 5 year General Surgery residency training in New York City. Following this, he completed a ColonRectal Surgery fellowship training program in Baltimore, Maryland and has subsequently established his practice in Houston since 1988. Dr. Aquino is certified by the American Boards of both (General) Surgery and ColonRectal Surgery. He is a Fellow of the American College of Surgeons, the Royal College of Surgeons (Glasgow, UK) and the American Society of Colon and Rectal Surgeons. Most of his surgery is done in an outpatient setting as this has been shown to be both cost effective and well accepted by patients. Whenever possible, special long acting local anesthetic techniques are used to maximize patient comfort. Dr. Aquino is the only board certified Colon/Rectal surgeon in the entire Galveston Bay area, East of Dr. -

Inguinal Hernia Repair Procedure Guide
INGUINAL HERNIA REPAIR PROCEDURE GUIDE EXAMPLE OPERATING ROOM (OR) CONFIGURATION PATIENT POSITIONING & PREPARATION PORT PLACEMENT SYSTEM DEPLOYMENT & DOCKING SUGGESTED INGUINAL HERNIA PROCEDURE STEPS INSTRUMENT GUIDE IMPORTANT SAFETY INFORMATION Inguinal Hernia Repair – Transabdominal Preperitoneal (TAPP). For use with the da Vinci Xi Surgical System. Developed with, reviewed and approved by Brian Harkins, MD. 1 2 3 4 5 6 7 8 9 PN1039738 REV A 08/2017 INGUINAL HERNIA REPAIR PROCEDURE GUIDE EXAMPLE OPERATING EXAMPLE OPERATING ROOM CONFIGURATION ROOM (OR) CONFIGURATION The following figure shows an overhead view of the recommended OR configuration for a da Vinci PATIENT POSITIONING Inguinal Hernia Repair (Figure 1). & PREPARATION NOTE: Configuration of the operating room suite is dependent on room dimensions as well as the preference and experience of the surgeon. PORT PLACEMENT SYSTEM DEPLOYMENT & DOCKING SUGGESTED INGUINAL HERNIA PROCEDURE STEPS INSTRUMENT GUIDE IMPORTANT SAFETY INFORMATION Inguinal Hernia Repair – Transabdominal Preperitoneal (TAPP). For use with the da Vinci Xi Surgical System. FIGURE 1 Developed with, reviewed and approved by Brian Harkins, MD. 1 2 3 4 5 6 7 8 9 PN1039738 REV A 08/2017 INGUINAL HERNIA REPAIR PROCEDURE GUIDE EXAMPLE OPERATING PATIENT POSITIONING & PREPARATION ROOM (OR) CONFIGURATION > Place the patient in the supine position. PATIENT POSITIONING > Tuck the arms and pad pressure points and bony prominences. & PREPARATION > Secure the patient to the table to avoid any shifting with the Trendelenburg position. > Sterilely prep the abdomen. PORT PLACEMENT > Insufflate the peritoneal cavity up to 12 mmHg. > Before docking, place the patient in approximately 15° Trendelenburg and lower the table as much as possible (Figure 2).