Physiology of Ventilation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Solutes and Solution
Solutes and Solution The first rule of solubility is “likes dissolve likes” Polar or ionic substances are soluble in polar solvents Non-polar substances are soluble in non- polar solvents Solutes and Solution There must be a reason why a substance is soluble in a solvent: either the solution process lowers the overall enthalpy of the system (Hrxn < 0) Or the solution process increases the overall entropy of the system (Srxn > 0) Entropy is a measure of the amount of disorder in a system—entropy must increase for any spontaneous change 1 Solutes and Solution The forces that drive the dissolution of a solute usually involve both enthalpy and entropy terms Hsoln < 0 for most species The creation of a solution takes a more ordered system (solid phase or pure liquid phase) and makes more disordered system (solute molecules are more randomly distributed throughout the solution) Saturation and Equilibrium If we have enough solute available, a solution can become saturated—the point when no more solute may be accepted into the solvent Saturation indicates an equilibrium between the pure solute and solvent and the solution solute + solvent solution KC 2 Saturation and Equilibrium solute + solvent solution KC The magnitude of KC indicates how soluble a solute is in that particular solvent If KC is large, the solute is very soluble If KC is small, the solute is only slightly soluble Saturation and Equilibrium Examples: + - NaCl(s) + H2O(l) Na (aq) + Cl (aq) KC = 37.3 A saturated solution of NaCl has a [Na+] = 6.11 M and [Cl-] = -

Ventilation Patterns Influence Airway Secretion Movement Marcia S Volpe, Alexander B Adams MPH RRT FAARC, Marcelo B P Amato MD, and John J Marini MD
Original Contributions Ventilation Patterns Influence Airway Secretion Movement Marcia S Volpe, Alexander B Adams MPH RRT FAARC, Marcelo B P Amato MD, and John J Marini MD BACKGROUND: Retention of airway secretions is a common and serious problem in ventilated patients. Treating or avoiding secretion retention with mucus thinning, patient-positioning, airway suctioning, or chest or airway vibration or percussion may provide short-term benefit. METHODS: In a series of laboratory experiments with a test-lung system we examined the role of ventilator settings and lung-impedance on secretion retention and expulsion. Known quantities of a synthetic dye-stained mucus simulant with clinically relevant properties were injected into a transparent tube the diameter of an adult trachea and exposed to various mechanical-ventilation conditions. Mucus- simulant movement was measured with a photodensitometric technique and examined with image- analysis software. We tested 2 mucus-simulant viscosities and various peak flows, inspiratory/ expiratory flow ratios, intrinsic positive end-expiratory pressures, ventilation waveforms, and impedance values. RESULTS: Ventilator settings that produced flow bias had a major effect on mucus movement. Expiratory flow bias associated with intrinsic positive end-expiratory pressure generated by elevated minute ventilation moved mucus toward the airway opening, whereas in- trinsic positive end-expiratory pressure generated by increased airway resistance moved the mucus toward the lungs. Inter-lung transfer of mucus simulant occurred rapidly across the “carinal divider” between interconnected test lungs set to radically different compliances; the mucus moved out of the low-compliance lung and into the high-compliance lung. CONCLUSIONS: The move- ment of mucus simulant was influenced by the ventilation pattern and lung impedance. -

COVID-19 Pneumonia: Different Respiratory Treatment for Different Phenotypes? L
Intensive Care Medicine EDITORIAL Un-edited accepted proof COVID-19 pneumonia: different respiratory treatment for different phenotypes? L. Gattinoni1, D. Chiumello2, P. Caironi3, M. Busana1, F. Romitti1, L. Brazzi4, L. Camporota5 Affiliations: 1Department of Anesthesiology and Intensive Care, Medical University of GöttinGen 4Department of Anesthesia, Intensive Care and Emergency - 'Città della Salute e della Scienza’ Hospital - Turin 5Department of Adult Critical Care, Guy’s and St Thomas’ NHS Foundation Trust, Health Centre for Human and Applied Physiological Sciences - London Corresponding author: Luciano Gattinoni Department of Anesthesiology and Intensive Care, Medical University of Göttingen, Robert-Koch Straße 40, 37075, Göttingen, Germany Conflict of interests: The authors have no conflict of interest to disclose NOTE: This article is the pre-proof author’s accepted version. The final edited version will appear soon on the website of the journal Intensive Care Medicine with the following DOI number: DOI 10.1007/s00134-020-06033-2 1 Gattinoni L. et al. COVID-19 pneumonia: different respiratory treatment for different phenotypes? (2020) Intensive Care Medicine; DOI: 10.1007/s00134-020-06033-2 Intensive Care Medicine EDITORIAL Un-edited accepted proof The Surviving Sepsis CampaiGn panel (ahead of print, DOI: 10.1007/s00134-020-06022-5) recently recommended that “mechanically ventilated patients with COVID-19 should be managed similarly to other patients with acute respiratory failure in the ICU.” Yet, COVID-19 pneumonia [1], despite falling in most of the circumstances under the Berlin definition of ARDS [2], is a specific disease, whose distinctive features are severe hypoxemia often associated with near normal respiratory system compliance (more than 50% of the 150 patients measured by the authors and further confirmed by several colleagues in Northern Italy). -

Pulmonary Surfactant: the Key to the Evolution of Air Breathing Christopher B
Pulmonary Surfactant: The Key to the Evolution of Air Breathing Christopher B. Daniels and Sandra Orgeig Department of Environmental Biology, University of Adelaide, Adelaide, South Australia 5005, Australia Pulmonary surfactant controls the surface tension at the air-liquid interface within the lung. This sys- tem had a single evolutionary origin that predates the evolution of the vertebrates and lungs. The lipid composition of surfactant has been subjected to evolutionary selection pressures, partic- ularly temperature, throughout the evolution of the vertebrates. ungs have evolved independently on several occasions pendent units, do not necessarily stretch upon inflation but Lover the past 300 million years in association with the radi- unpleat or unfold in a complex manner. Moreover, the many ation and diversification of the vertebrates, such that all major fluid-filled corners and crevices in the alveoli open and close vertebrate groups have members with lungs. However, lungs as the lung inflates and deflates. differ considerably in structure, embryological origin, and Surfactant in nonmammals exhibits an antiadhesive func- function between vertebrate groups. The bronchoalveolar lung tion, lining the interface between apposed epithelial surfaces of mammals is a branching “tree” of tubes leading to millions within regions of a collapsed lung. As the two apposing sur- of tiny respiratory exchange units, termed alveoli. In humans faces peel apart, the lipids rise to the surface of the hypophase there are ~25 branches and 300 million alveoli. This structure fluid at the expanding gas-liquid interface and lower the sur- allows for the generation of an enormous respiratory surface face tension of this fluid, thereby decreasing the work required area (up to 70 m2 in adult humans). -

Maximum Expiratory Flow Rates in Induced Bronchoconstriction in Man
Maximum expiratory flow rates in induced bronchoconstriction in man A. Bouhuys, … , B. M. Kim, A. Zapletal J Clin Invest. 1969;48(6):1159-1168. https://doi.org/10.1172/JCI106073. Research Article We evaluated changes of maximum expiratory flow-volume (MEFV) curves and of partial expiratory flow-volume (PEFV) curves caused by bronchoconstrictor drugs and dust, and compared these to the reverse changes induced by a bronchodilator drug in previously bronchoconstricted subjects. Measurements of maximum flow at constant lung inflation (i.e. liters thoracic gas volume) showed larger changes, both after constriction and after dilation, than measurements of peak expiratory flow rate, 1 sec forced expiratory volume and the slope of the effort-independent portion of MEFV curves. Changes of flow rates on PEFV curves (made after inspiration to mid-vital capacity) were usually larger than those of flow rates on MEFV curves (made after inspiration to total lung capacity). The decreased maximum flow rates after constrictor agents are not caused by changes in lung static recoil force and are attributed to narrowing of small airways, i.e., airways which are uncompressed during forced expirations. Changes of maximum expiratory flow rates at constant lung inflation (e.g. 60% of the control total lung capacity) provide an objective and sensitive measurement of changes in airway caliber which remains valid if total lung capacity is altered during treatment. Find the latest version: https://jci.me/106073/pdf Maximum Expiratory Flow Rates in Induced Bronchoconstriction in Man A. Bouiuys, V. R. HuNTr, B. M. Kim, and A. ZAPLETAL From the John B. Pierce Foundation Laboratory and the Yale University School of Medicine, New Haven, Connecticut 06510 A B S T R A C T We evaluated changes of maximum ex- rates are best studied as a function of lung volume. -

Page 1 of 6 This Is Henry's Law. It Says That at Equilibrium the Ratio of Dissolved NH3 to the Partial Pressure of NH3 Gas In
CHMY 361 HANDOUT#6 October 28, 2012 HOMEWORK #4 Key Was due Friday, Oct. 26 1. Using only data from Table A5, what is the boiling point of water deep in a mine that is so far below sea level that the atmospheric pressure is 1.17 atm? 0 ΔH vap = +44.02 kJ/mol H20(l) --> H2O(g) Q= PH2O /XH2O = K, at ⎛ P2 ⎞ ⎛ K 2 ⎞ ΔH vap ⎛ 1 1 ⎞ ln⎜ ⎟ = ln⎜ ⎟ − ⎜ − ⎟ equilibrium, i.e., the Vapor Pressure ⎝ P1 ⎠ ⎝ K1 ⎠ R ⎝ T2 T1 ⎠ for the pure liquid. ⎛1.17 ⎞ 44,020 ⎛ 1 1 ⎞ ln⎜ ⎟ = − ⎜ − ⎟ = 1 8.3145 ⎜ T 373 ⎟ ⎝ ⎠ ⎝ 2 ⎠ ⎡1.17⎤ − 8.3145ln 1 ⎢ 1 ⎥ 1 = ⎣ ⎦ + = .002651 T2 44,020 373 T2 = 377 2. From table A5, calculate the Henry’s Law constant (i.e., equilibrium constant) for dissolving of NH3(g) in water at 298 K and 340 K. It should have units of Matm-1;What would it be in atm per mole fraction, as in Table 5.1 at 298 K? o For NH3(g) ----> NH3(aq) ΔG = -26.5 - (-16.45) = -10.05 kJ/mol ΔG0 − [NH (aq)] K = e RT = 0.0173 = 3 This is Henry’s Law. It says that at equilibrium the ratio of dissolved P NH3 NH3 to the partial pressure of NH3 gas in contact with the liquid is a constant = 0.0173 (Henry’s Law Constant). This also says [NH3(aq)] =0.0173PNH3 or -1 PNH3 = 0.0173 [NH3(aq)] = 57.8 atm/M x [NH3(aq)] The latter form is like Table 5.1 except it has NH3 concentration in M instead of XNH3. -

Statistical Mechanics I: Exam Review 1 Solution
8.333: Statistical Mechanics I Fall 2007 Test 1 Review Problems The first in-class test will take place on Wednesday 9/26/07 from 2:30 to 4:00 pm. There will be a recitation with test review on Friday 9/21/07. The test is ‘closed book,’ but if you wish you may bring a one-sided sheet of formulas. The test will be composed entirely from a subset of the following problems. Thus if you are familiar and comfortable with these problems, there will be no surprises! ******** You may find the following information helpful: Physical Constants 31 27 Electron mass me 9.1 10− kg Proton mass mp 1.7 10− kg ≈ × 19 ≈ × 34 1 Electron Charge e 1.6 10− C Planck’s const./2π ¯h 1.1 10− Js− ≈ × 8 1 ≈ × 8 2 4 Speed of light c 3.0 10 ms− Stefan’s const. σ 5.7 10− W m− K− ≈ × 23 1 ≈ × 23 1 Boltzmann’s const. k 1.4 10− JK− Avogadro’s number N 6.0 10 mol− B ≈ × 0 ≈ × Conversion Factors 5 2 10 4 1atm 1.0 10 Nm− 1A˚ 10− m 1eV 1.1 10 K ≡ × ≡ ≡ × Thermodynamics dE = T dS+dW¯ For a gas: dW¯ = P dV For a wire: dW¯ = Jdx − Mathematical Formulas √π ∞ n αx n! 1 0 dx x e− = αn+1 2 ! = 2 R 2 2 2 ∞ x √ 2 σ k dx exp ikx 2σ2 = 2πσ exp 2 limN ln N! = N ln N N −∞ − − − →∞ − h i h i R n n ikx ( ik) n ikx ( ik) n e− = ∞ − x ln e− = ∞ − x n=0 n! � � n=1 n! � �c P 2 4 P 3 5 cosh(x) = 1 + x + x + sinh(x) = x + x + x + 2! 4! · · · 3! 5! · · · 2πd/2 Surface area of a unit sphere in d dimensions Sd = (d/2 1)! − 1 1. -
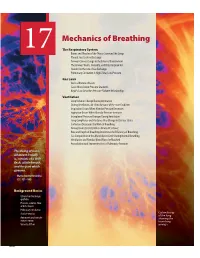
17 the Respiratory System
Mechanics of Breathing The Respiratory System 17 Bones and Muscles of the Thorax Surround the Lungs Pleural Sacs Enclose the Lungs Airways Connect Lungs to the External Environment The Airways Warm, Humidify, and Filter Inspired Air Alveoli Are the Site of Gas Exchange Pulmonary Circulation Is High-Flow, Low-Pressure G a s L a w s Air Is a Mixture of Gases Gases Move Down Pressure Gradients Boyle’s Law Describes Pressure-Volume Relationships Ventilation Lung Volumes Change During Ventilation During Ventilation, Air Flows Because of Pressure Gradients Inspiration Occurs When Alveolar Pressure Decreases Expiration Occurs When Alveolar Pressure Increases Intrapleural Pressure Changes During Ventilation Lung Compliance and Elastance May Change in Disease States Surfactant Decreases the Work of Breathing Airway Diameter Determines Airway Resistance Rate and Depth of Breathing Determine the Effi ciency of Breathing Gas Composition in the Alveoli Varies Little During Normal Breathing Ventilation and Alveolar Blood Flow Are Matched Auscultation and Spirometry Assess Pulmonary Function This being of mine, whatever it really is, consists of a little fl esh, a little breath, and the part which governs. — Marcus Aurelius Antoninus ( C . E . 121–180) Background Basics Ciliated and exchange epithelia Pressure, volume, fl ow, and resistance Pulmonary circulation Surface tension Colored x-ray of the lung Autonomic and somatic showing the motor neurons branching Velocity of fl ow airways. 600 Mechanics of Breathing magine covering the playing surface of a racquetball court cavity to control their contact with the outside air. Internalization (about 75 m2 ) with thin plastic wrap, then crumpling up the creates a humid environment for the exchange of gases with the wrap and stuffi ng it into a 3-liter soft drink bottle. -
Unit 11 Sound Speed of Sound Speed of Sound Sound Can Travel Through Any Kind of Matter, but Not Through a Vacuum
Unit 11 Sound Speed of Sound Speed of Sound Sound can travel through any kind of matter, but not through a vacuum. The speed of sound is different in different materials; in general, it is slowest in gases, faster in liquids, and fastest in solids. The speed depends somewhat on temperature, especially for gases. vair = 331.0 + 0.60T T is the temperature in degrees Celsius Example 1: Find the speed of a sound wave in air at a temperature of 20 degrees Celsius. v = 331 + (0.60) (20) v = 331 m/s + 12.0 m/s v = 343 m/s Using Wave Speed to Determine Distances At normal atmospheric pressure and a temperature of 20 degrees Celsius, speed of sound: v = 343m / s = 3.43102 m / s Speed of sound 750 mi/h Speed of light 670 616 629 mi/h c = 300,000,000m / s = 3.00 108 m / s Delay between the thunder and lightning Example 2: The thunder is heard 3 seconds after the lightning seen. Find the distance to storm location. The speed of sound is 345 m/s. distance = v t = (345m/s)(3s) = 1035m Example 3: Another phenomenon related to the perception of time delays between two events is an echo. In a canyon, an echo is heard 1.40 seconds after making the holler. Find the distance to the canyon wall (v=345m/s) distanceround trip = vt = (345 m/s )( 1.40 s) = 483 m d= 484/2=242m Applications: Sonar, Ultrasound, and Medical Imaging • Ultrasound or ultrasonography is a medical imaging technique that uses high frequency sound waves and their echoes. -

Respiratory Therapy Pocket Reference
Pulmonary Physiology Volume Control Pressure Control Pressure Support Respiratory Therapy “AC” Assist Control; AC-VC, ~CMV (controlled mandatory Measure of static lung compliance. If in AC-VC, perform a.k.a. a.k.a. AC-PC; Assist Control Pressure Control; ~CMV-PC a.k.a PS (~BiPAP). Spontaneous: Pressure-present inspiratory pause (when there is no flow, there is no effect ventilation = all modes with RR and fixed Ti) PPlateau of Resistance; Pplat@Palv); or set Pause Time ~0.5s; RR, Pinsp, PEEP, FiO2, Flow Trigger, rise time, I:E (set Pocket Reference RR, Vt, PEEP, FiO2, Flow Trigger, Flow pattern, I:E (either Settings Pinsp, PEEP, FiO2, Flow Trigger, Rise time Target: < 30, Optimal: ~ 25 Settings directly or by inspiratory time Ti) Settings directly or via peak flow, Ti settings) Decreasing Ramp (potentially more physiologic) PIP: Total inspiratory work by vent; Reflects resistance & - Decreasing Ramp (potentially more physiologic) Card design by Respiratory care providers from: Square wave/constant vs Decreasing Ramp (potentially Flow Determined by: 1) PS level, 2) R, Rise Time ( rise time ® PPeak inspiratory compliance; Normal ~20 cmH20 (@8cc/kg and adult ETT); - Peak Flow determined by 1) Pinsp level, 2) R, 3)Ti (shorter Flow more physiologic) ¯ peak flow and 3.) pt effort Resp failure 30-40 (low VT use); Concern if >40. Flow = more flow), 4) pressure rise time (¯ Rise Time ® Peak v 0.9 Flow), 5) pt effort ( effort ® peak flow) Pplat-PEEP: tidal stress (lung injury & mortality risk). Target Determined by set RR, Vt, & Flow Pattern (i.e. for any set I:E Determined by patient effort & flow termination (“Esens” – PDriving peak flow, Square (¯ Ti) & Ramp ( Ti); Normal Ti: 1-1.5s; see below “Breath Termination”) < 15 cmH2O. -

Epidemiology and Pulmonary Physiology of Severe Asthma
Epidemiology and Pulmonary Physiology of Severe Asthma a b Jacqueline O’Toole, DO , Lucas Mikulic, MD , c, David A. Kaminsky, MD * KEYWORDS Demographics Phenotype Health care utilization Pulmonary function Lung elastic recoil Ventilation heterogeneity Gas trapping Airway hyperresponsiveness KEY POINTS The definition of severe asthma is still a work in progress. The severity of asthma is predictive of higher health care utilization. Cluster analysis is useful in characterizing severe asthma phenotypes. Airway hyperresponsiveness in severe asthma is a result of abnormal airflow, lung recoil, ventilation, and gas trapping. Patients with severe asthma may have a reduced perception of dyspnea. INTRODUCTION Severe asthma is a characterized by a complex set of clinical, demographic, and physiologic features. In this article, we review both the epidemiology and pulmonary physiology associated with severe asthma. DEMOGRAPHICS OF SEVERE ASTHMA Asthma has long been recognized as a worldwide noncommunicable disease of importance. Within the population of individuals with asthma, there is a subgroup of individuals at high risk for complications, exacerbations, and a poor quality of life. The authors have nothing to disclose. a Department of Medicine, University of Vermont Medical Center, 111 Colchester Avenue, Bur- lington, VT 05401, USA; b Division of Pulmonary and Critical Care Medicine, University of Ver- mont Medical Center, Given D208, 89 Beaumont Avenue, Burlington, VT 05405, USA; c Division of Pulmonary and Critical Care Medicine, University of Vermont College of Medicine, Given D213, 89 Beaumont Avenue, Burlington, VT 05405, USA * Corresponding author. E-mail address: [email protected] Immunol Allergy Clin N Am 36 (2016) 425–438 http://dx.doi.org/10.1016/j.iac.2016.03.001 immunology.theclinics.com 0889-8561/16/$ – see front matter Ó 2016 Elsevier Inc. -

Atmospheric Cold Front-Generated Waves in the Coastal Louisiana
Journal of Marine Science and Engineering Article Atmospheric Cold Front-Generated Waves in the Coastal Louisiana Yuhan Cao 1 , Chunyan Li 2,* and Changming Dong 1,3,* 1 School of Marine Sciences, Nanjing University of Information Science and Technology, Nanjing 210044, China; [email protected] 2 Department of Oceanography and Coastal Sciences, College of the Coast and Environment, Louisiana State University, Baton Rouge, LA 70803, USA 3 Southern Laboratory of Ocean Science and Engineering (Zhuhai), Zhuhai 519000, China * Correspondence: [email protected] (C.L.); [email protected] (C.D.); Tel.: +1-225-578-2520 (C.L.); +86-025-58695733 (C.D.) Received: 15 October 2020; Accepted: 9 November 2020; Published: 11 November 2020 Abstract: Atmospheric cold front-generated waves play an important role in the air–sea interaction and coastal water and sediment transports. In-situ observations from two offshore stations are used to investigate variations of directional waves in the coastal Louisiana. Hourly time series of significant wave height and peak wave period are examined for data from 2004, except for the summer time between May and August, when cold fronts are infrequent and weak. The intra-seasonal scale variations in the wavefield are significantly affected by the atmospheric cold frontal events. The wave fields and directional wave spectra induced by four selected cold front passages over the coastal Louisiana are discussed. It is found that significant wave height generated by cold fronts coming from the west change more quickly than that by other passing cold fronts. The peak wave direction rotates clockwise during the cold front events.