COVID-19 Pneumonia: Different Respiratory Treatment for Different Phenotypes? L
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Speakers and Topics
SPEAKERS AND TOPICS SALZBURG WEILL CORNELL SEMINAR ANESTHESIOLOGY AND INTENSIVE CARE Sunday, October 18 – Saturday, October 24, 2020 Schloss Arenberg, Salzburg, Austria Course Director: Hugh C. Hemmings Jr., MD, PhD, FRCA Co-Course Director: Klaus Markstaller, MD Co-Course Director: Kane O. Pryor, MD Co-Course Director: Peter Marhofer, MD SPEAKERS AND TOPICS: Meghann M. Fitzgerald, MD Assistant Professor of Clinical Anesthesiology Weill Cornell Medical College Assistant Attending Anesthesiologist NewYork-Presbyterian Hospital Weill Cornell Medicine Anesthesiology New York, NY USA • Robotic Cardiac Surgery • Blood Management in Cardiac Surgery • TAAA Repair Lukas Kirchmair, MD, PD, DESA, EDRA Department of Anesthesiology and Intensive Care District Hospital Schwaz Schwaz Austria • Polytrauma Management Rudolf Likar, MD, MSc Professor Head, Department of Anesthesiology and Intensive Care General Hospital Klagenfurt Klagenfurt am Woerthersee Austria • Invasive Methods in Cancer Pain • Invasive Methods in Low Back Pain © Open Medical Institute 2020 SPEAKERS AND TOPICS Peter Marhofer, MD Professor of Anesthesia and Intensive Care Medicine Department of Anesthesia and Intensive Care Medicine Medical University of Vienna Vienna Austria • Principles of Regional Anaesthesia I • Principles of Regional Anaesthesia II • Ultrasound in Anaesthesia and Intensive Care Medicine I • Ultrasound in Anaesthesia and Intensive Care Medicine II Rohan Panchamia, MD Assistant Professor of Clinical Anesthesiology Weill Cornell Medical College Assistant Attending -

Ventilation Patterns Influence Airway Secretion Movement Marcia S Volpe, Alexander B Adams MPH RRT FAARC, Marcelo B P Amato MD, and John J Marini MD
Original Contributions Ventilation Patterns Influence Airway Secretion Movement Marcia S Volpe, Alexander B Adams MPH RRT FAARC, Marcelo B P Amato MD, and John J Marini MD BACKGROUND: Retention of airway secretions is a common and serious problem in ventilated patients. Treating or avoiding secretion retention with mucus thinning, patient-positioning, airway suctioning, or chest or airway vibration or percussion may provide short-term benefit. METHODS: In a series of laboratory experiments with a test-lung system we examined the role of ventilator settings and lung-impedance on secretion retention and expulsion. Known quantities of a synthetic dye-stained mucus simulant with clinically relevant properties were injected into a transparent tube the diameter of an adult trachea and exposed to various mechanical-ventilation conditions. Mucus- simulant movement was measured with a photodensitometric technique and examined with image- analysis software. We tested 2 mucus-simulant viscosities and various peak flows, inspiratory/ expiratory flow ratios, intrinsic positive end-expiratory pressures, ventilation waveforms, and impedance values. RESULTS: Ventilator settings that produced flow bias had a major effect on mucus movement. Expiratory flow bias associated with intrinsic positive end-expiratory pressure generated by elevated minute ventilation moved mucus toward the airway opening, whereas in- trinsic positive end-expiratory pressure generated by increased airway resistance moved the mucus toward the lungs. Inter-lung transfer of mucus simulant occurred rapidly across the “carinal divider” between interconnected test lungs set to radically different compliances; the mucus moved out of the low-compliance lung and into the high-compliance lung. CONCLUSIONS: The move- ment of mucus simulant was influenced by the ventilation pattern and lung impedance. -

Intensive Care Medicine in 10 Years
BOOKS,FILMS,TAPES &SOFTWARE are difficult to read, the editing is inconsis- tory for critical care medicine. The book is initiate a planning process for leaders who tent, and the content that was omitted indi- divided into sections entitled “Setting the recognize the imperative for change and ad- cates that “efforts to bring this work from Stage,” “Diagnostic, Therapeutic, and In- aptation in critical care. Accordingly, I rec- conception to fruition in less than one year” formation Technologies 10 Years From ommend this book to individuals and groups (as stated in the book’s acknowledgments Now,” “How Might Critical Care Medicine engaged in all aspects of critical care man- section) prevented this book from being a Be Organized and Regulated?” “Training,” agement, now and in the future. “gold standard” text. and “The Critical Care Agenda.” Each sec- J Christopher Farmer MD tion consists of a series of essays/chapters Marie E Steiner MD MSc Department of Medicine that discuss various aspects of the topic, and Department of Pediatrics Mayo Clinic all the sections have solid scientific support Divisions of Pulmonary/ Rochester, Minnesota and bibliographies. The individual topics Critical Care and Hematology/ span the entire range of critical-care clinical Oncology/Blood and Marrow The author reports no conflict of interest related practice, administration, quality and safety, Transplantation to the content of this book review. and so forth. The contributors are acknowl- University Children’s Hospital, Fairview edged senior clinical and scientific leaders University of Minnesota Mechanical Ventilation: Physiological in critical care medicine from around the Minneapolis, Minnesota and Clinical Applications, 4th edition. -
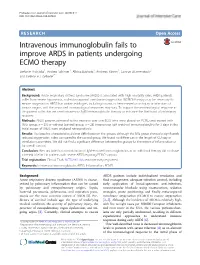
Intravenous Immunoglobulin Fails to Improve ARDS in Patients
Prohaska et al. Journal of Intensive Care (2018) 6:11 DOI 10.1186/s40560-018-0278-8 RESEARCH Open Access Intravenous immunoglobulin fails to improve ARDS in patients undergoing ECMO therapy Stefanie Prohaska1, Andrea Schirner1, Albina Bashota1, Andreas Körner1, Gunnar Blumenstock2 and Helene A. Haeberle1* Abstract Background: Acute respiratory distress syndrome (ARDS) is associated with high mortality rates. ARDS patients suffer from severe hypoxemia, and extracorporeal membrane oxygenation (ECMO) therapy may be necessary to ensure oxygenation. ARDS has various etiologies, including trauma, ischemia-reperfusion injury or infections of various origins, and the associated immunological responses may vary. To support the immunological response in this patient collective, we used intravenous IgM immunoglobulin therapy to enhance the likelihood of pulmonary recovery. Methods: ARDS patients admitted to the intensive care unit (ICU) who were placed on ECMO and treated with (IVIG group; n = 29) or without (control group; n = 28) intravenous IgM-enriched immunoglobulins for 3 days in the initial stages of ARDS were analyzed retrospectively. Results: The baseline characteristics did not differ between the groups, although the IVIG group showed a significantly reduced oxygenation index compared to the control group. We found no differences in the length of ICU stay or ventilation parameters. We did not find a significant difference between the groups for the extent of inflammation or for overall survival. Conclusion: We conclude that administration -

The Basics of Ventilator Management Overview How We Breath
3/23/2019 The Basics of Ventilator Management What are we really trying to do here Peter Lutz, MD Pulmonary and Critical Care Medicine Pulmonary Associates, Mobile, Al Overview • Approach to the physiology of the lung and physiological goals of mechanical Ventilation • Different Modes of Mechanical Ventilation and when they are indicated • Ventilator complications • Ventilator Weaning • Some basic trouble shooting How we breath http://people.eku.edu/ritchisong/301notes6.htm 1 3/23/2019 How a Mechanical Ventilator works • The First Ventilator- the Iron Lung – Worked by creating negative atmospheric pressure around the lung, simulating the negative pressure of inspiration How a Mechanical Ventilator works • The Modern Ventilator – The invention of the demand oxygen valve for WWII pilots if the basis for the modern ventilator https://encrypted-tbn0.gstatic.com/images?q=tbn:ANd9GcRI5v-veZULMbt92bfDmUUW32SrC6ywX1vSzY1xr40aHMdsCVyg6g How a Mechanical Ventilator works • The Modern Ventilator – How it works Inspiratory Limb Flow Sensor Ventilator Pressure Sensor Expiratory Limb 2 3/23/2019 So what are the goals of Mechanical Ventilation • What are we trying to control – Oxygenation • Amount of oxygen we are getting into the blood – Ventilation • The movement of air into and out of the lungs, mainly effects the pH and level of CO 2 in the blood stream Lab Oxygenation Ventilation Pulse Ox Saturation >88-90% Arterial Blood Gas(ABG) Po 2(75-100 mmHg) pCO 2(40mmHg) pH(~7.4) Oxygenation How do we effect Oxygenation • Fraction of Inspired Oxygen (FIO 2) – Percentage of the gas mixture given to the patient that is Oxygen • Room air is 21% • On the vent ranges from 30-100% • So if the patient’s blood oxygen levels are low, we can just increase the amount of oxygen we give them 3 3/23/2019 How do we effect Oxygenation • Positive End Expiratory Pressure (PEEP) – positive pressure that will remains in the airways at the end of the respiratory cycle (end of exhalation) that is greater than the atmospheric pressure in mechanically ventilated patients. -

Neonatal Ventilation
Neonatal Ventilation Edward G. Shepherd History • Bourgeois, 1609: – “…give a small spoonfulof pure wine into the neonate’s mouth, …[to] help the infant to regain its spirits when being agitated by the labors, which sometimes make it so weak that it seems more dead than alive.” • Mauriceau, mid-1600’s: – “[The baby] should be rested on a warmed bed and brought near the fire, where the midwife having taken some wine into her mouth shall blow it into the infant’s mouth, which can be repeated several times if necessary … She should warm all the parts of the body to recall the blood and the spirits which retired during the weakness and endangered suffocation.” Neonatology 2008;94:144–149 History • Levret, 1766: – “There is one more means which sometimes works as by enchantment, it is to apply one’s mouth on that of the infant and to blow into it, taking care to pinch the tip of the nose simultaneously. This method is so effective that it is really rare that others are useful if it fails” Neonatology 2008;94:144–149 History • First ventilators: – Hunter, Chaussier, and Gorcy in the mid 1700’s • Bellows or gas attached to masks or tubes • 1800’s – Discovery of the breathing center – Determination of survival time in asphyxiated animals – First attempts at electrical resuscitation Neonatology 2008;94:144–149 History • By mid 1800’s ventilation fell out of favor – Fears of pnuemothorax, infection, and sudden death – Various positional techniques were developed • “Schultze swingings” • Arm extension and then chest compression – Stayed in practice -

Respiratory Therapy Pocket Reference
Pulmonary Physiology Volume Control Pressure Control Pressure Support Respiratory Therapy “AC” Assist Control; AC-VC, ~CMV (controlled mandatory Measure of static lung compliance. If in AC-VC, perform a.k.a. a.k.a. AC-PC; Assist Control Pressure Control; ~CMV-PC a.k.a PS (~BiPAP). Spontaneous: Pressure-present inspiratory pause (when there is no flow, there is no effect ventilation = all modes with RR and fixed Ti) PPlateau of Resistance; Pplat@Palv); or set Pause Time ~0.5s; RR, Pinsp, PEEP, FiO2, Flow Trigger, rise time, I:E (set Pocket Reference RR, Vt, PEEP, FiO2, Flow Trigger, Flow pattern, I:E (either Settings Pinsp, PEEP, FiO2, Flow Trigger, Rise time Target: < 30, Optimal: ~ 25 Settings directly or by inspiratory time Ti) Settings directly or via peak flow, Ti settings) Decreasing Ramp (potentially more physiologic) PIP: Total inspiratory work by vent; Reflects resistance & - Decreasing Ramp (potentially more physiologic) Card design by Respiratory care providers from: Square wave/constant vs Decreasing Ramp (potentially Flow Determined by: 1) PS level, 2) R, Rise Time ( rise time ® PPeak inspiratory compliance; Normal ~20 cmH20 (@8cc/kg and adult ETT); - Peak Flow determined by 1) Pinsp level, 2) R, 3)Ti (shorter Flow more physiologic) ¯ peak flow and 3.) pt effort Resp failure 30-40 (low VT use); Concern if >40. Flow = more flow), 4) pressure rise time (¯ Rise Time ® Peak v 0.9 Flow), 5) pt effort ( effort ® peak flow) Pplat-PEEP: tidal stress (lung injury & mortality risk). Target Determined by set RR, Vt, & Flow Pattern (i.e. for any set I:E Determined by patient effort & flow termination (“Esens” – PDriving peak flow, Square (¯ Ti) & Ramp ( Ti); Normal Ti: 1-1.5s; see below “Breath Termination”) < 15 cmH2O. -

Characteristics and Risk Factors for Intensive Care Unit Cardiac Arrest in Critically Ill Patients with COVID-19—A Retrospective Study
Journal of Clinical Medicine Article Characteristics and Risk Factors for Intensive Care Unit Cardiac Arrest in Critically Ill Patients with COVID-19—A Retrospective Study Kevin Roedl 1,* , Gerold Söffker 1, Dominic Wichmann 1 , Olaf Boenisch 1, Geraldine de Heer 1 , Christoph Burdelski 1, Daniel Frings 1, Barbara Sensen 1, Axel Nierhaus 1 , Dirk Westermann 2, Stefan Kluge 1 and Dominik Jarczak 1 1 Department of Intensive Care Medicine, University Medical Centre Hamburg-Eppendorf, 20246 Hamburg, Germany; [email protected] (G.S.); [email protected] (D.W.); [email protected] (O.B.); [email protected] (G.d.H.); [email protected] (C.B.); [email protected] (D.F.); [email protected] (B.S.); [email protected] (A.N.); [email protected] (S.K.); [email protected] (D.J.) 2 Department of Interventional and General Cardiology, University Heart Centre Hamburg, 20246 Hamburg, Germany; [email protected] * Correspondence: [email protected]; Tel.: +49-40-7410-57020 Abstract: The severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) causing the coron- avirus disease 2019 (COVID-19) led to an ongoing pandemic with a surge of critically ill patients. Very little is known about the occurrence and characteristic of cardiac arrest in critically ill patients Citation: Roedl, K.; Söffker, G.; with COVID-19 treated at the intensive care unit (ICU). The aim was to investigate the incidence Wichmann, D.; Boenisch, O.; de Heer, and outcome of intensive care unit cardiac arrest (ICU-CA) in critically ill patients with COVID-19. G.; Burdelski, C.; Frings, D.; Sensen, This was a retrospective analysis of prospectively recorded data of all consecutive adult patients B.; Nierhaus, A.; Westermann, D.; with COVID-19 admitted (27 February 2020–14 January 2021) at the University Medical Centre et al. -
ASV Quick Guide
ASV Quick Guide Hamilton Medical | ASV 1 ! Warning This Quick Guide is based on evaluations by clinicians within and outside Hamilton Medical and is intended to serve as an example. This Quick Guide does not replace either the official operator’s manual of your ventilator or the clinical judgment of a physician. This Quick Guide should not - on its own - be used for clinical decision making. 2 Table of contents 1. Adaptive Support Ventilation (ASV) basics 4 2. Preparing for ventilation with ASV 6 3. Settings 8 4. ASV graph 12 5. Working principles of ASV 14 6. Monitoring ASV 16 7. Adjusting ASV 18 8. Weaning in ASV 20 Appendix 22 Lung-protective rules 22 Understanding the ASV safety box 24 Glossary 26 Hamilton Medical | ASV 3 1. Adaptive Support Ventilation (ASV) basics 1 ... 2 CO elimination ... 2 3 Oxygenation Conventional ventilation ASV 4 ASV focuses on simplification of mechanical ventilation. This means: 1 Eliminating separate modes for passive and active patients 2 Reducing controls relevant for CO2 elimination to just %MinVol 3 Adding direct access to controls relevant for oxygenation (PEEP/CPAP and Oxygen) ASV maintains an operator-preset minimum minute volume independent of the patient‘s activity. The breathing pattern (tidal volume, rate, and inspiratory time) is calculated, based on the assump- tion that the optimal breathing pattern results in: a The least work of breathing b The least amount of ventilator-applied inspiratory pressure A lung-protection strategy ensures ASV’s safety. ASV attempts to guide the patient using a favorable breathing pattern and avoids potentially detrimental patterns such as rapid shallow breathing, excessive dead space ventilation, intrinsic PEEP, barotrauma, and volutrauma. -

Rapid Evidence Review
Rapid Evidence Review Clinical evidence for the use of intravenous immunoglobulin in the treatment of COVID- 19 Version 2, 14th May 2020 1 Prepared by the COVID-19 Evidence Review Group with clinical contribution from Dr. Niall Conlon, Consultant Immunologist, St. James Hospital, Dr. Mary Keogan, Clinical Lead National Clinical Programme for Pathology & Consultant Immunologist, Beaumont Hospital. Key changes between version 1 and version 2 (14th May 2020) A number of case reports describing the use of IVIG are included in this version and 2 additional studies which focused specifically on the use of IVIG in patients with COVID-19 – one case series and one retrospective cohort study (available as a pre-print). A number of guidelines have included a reference to IVIG, but the general consensus is not to use IVIG. The recent reports of Kawasaki Disease in children with COVID-19 highlight the role of IVIG and aspirin to treat this condition and supporting evidence of its benefit are available from 2 case reports and one case series. The COVID-19 Evidence Review Group for Medicines was established to support the HSE in managing the significant amount of information on treatments for COVID-19. This COVID-19 Evidence Review Group is comprised of evidence synthesis practitioners from across the National Centre for Pharmacoeconomics (NCPE), Medicines Management Programme (MMP) and the National Medicines Information Centre (NMIC). The group respond to queries raised via the Office of the CCO, National Clinical Programmes and the Department of Health and respond in a timely way with the evidence review supporting the query. -

Surviving Sepsis Campaign Guidelines for COVID-19
DISCLAIMER. The information contained herein is subject to change. The final version of the article will be published as soon as approved on ccmjournal.org. Surviving Sepsis Campaign: Guidelines on the Management of Critically Ill Adults with Coronavirus Disease 2019 (COVID-19) Waleed Alhazzani1,2, Morten Hylander Møller3,4, Yaseen M. Arabi5, Mark Loeb1,2, Michelle Ng Gong6, Eddy Fan7, Simon Oczkowski1,2, Mitchell M. Levy8,9, Lennie Derde10,11, Amy Dzierba12, Bin Du13, Michael Aboodi6, Hannah Wunsch14,15, Maurizio Cecconi16,17, Younsuck Koh18, Daniel S. Chertow19, Kathryn Maitland20, Fayez Alshamsi21, Emilie Belley-Cote1,22, Massimiliano Greco16,17, Matthew Laundy23, Jill S. Morgan24, Jozef Kesecioglu10, Allison McGeer25, Leonard Mermel8, Manoj J. Mammen26, Paul E. Alexander2,27, Amy Arrington28, John Centofanti29, Giuseppe Citerio30,31, Bandar Baw1,32, Ziad A. Memish33, Naomi Hammond34,35, Frederick G. Hayden36, Laura Evans37, Andrew Rhodes38 Affiliations 1 Department of Medicine, McMaster University, Hamilton, Canada 2 Department of Health Research Methods, Evidence, and Impact, McMaster University, Canada 3 Copenhagen University Hospital Rigshospitalet, Department of Intensive Care, Copenhagen, Denmark 4 Scandinavian Society of Anaesthesiology and Intensive Care Medicine (SSAI) 5 Intensive Care Department, Ministry of National Guard Health Affairs, King Saud Bin Abdulaziz University for Health Sciences, King Abdullah International Medical Research Center, Riyadh, Kingdom of Saudi Arabia 6 Department of Medicine, Montefiore Healthcare -

1. Ventilator Management
1. Ventilator Management Indications for Mechanical Ventilation Apnea Ventilatory insufficiency Increase in PaCo2 and decrease in ph Refractory hypoxemia Complications Associated with Mechanical Ventilation Hypotension Increased intrathoracic pressure decreases venous return to the heart Increased risk of ventilator associated pneumonia (VAP) Keep HOB at > 30 Maintain frequent, good oral care Problems with endotracheal tube Mucous plugging Tube my become dislodged Kinking or biting of tube Cuff rupture Pneumothorax Initial Ventilator Settings—parameters to be clarified Type of ventilation Mode of ventilation Tidal volume or peak inspiratory setting Respiratory rate FiO2 PEEP (Positive End Expiratory Pressure) Types of Ventilation Volume Cycled Ventilation(VCV) A pre-selected tidal volume is delivered at the pressure required. Tidal volume guaranteed. Peak inspiratory pressure will vary depending on airway resistance and lung compliance. Pressure Control Time-Cycled Ventilation (PCV) Operator selects inspiratory pressure and inspiratory time Breath is terminated when inspiratory time is reached Inspiratory pressure is guaranteed; tidal volume is dependant on airway resistance and lung compliance Pressure Support (PSV) Requires intact respiratory drive Operator selects inspiratory pressure Patient initiates breath, pressure quickly rises to set pressure and is maintained throughout the inspiratory phase Tidal volume determined by lung compliance and inspiratory effort Modes of Ventilation Assist/Control