Association of High-Dose Cyclophosphamide, Cisplatin, And
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Australian Public Assessment Report for Aminolevulinic Acid Hcl
Australian Public Assessment Report for Aminolevulinic acid HCl Proprietary Product Name: Gliolan Sponsor: Specialised Therapeutics Australia Pty Ltd March 2014 Therapeutic Goods Administration About the Therapeutic Goods Administration (TGA) · The Therapeutic Goods Administration (TGA) is part of the Australian Government Department of Health, and is responsible for regulating medicines and medical devices. · The TGA administers the Therapeutic Goods Act 1989 (the Act), applying a risk management approach designed to ensure therapeutic goods supplied in Australia meet acceptable standards of quality, safety and efficacy (performance), when necessary. · The work of the TGA is based on applying scientific and clinical expertise to decision- making, to ensure that the benefits to consumers outweigh any risks associated with the use of medicines and medical devices. · The TGA relies on the public, healthcare professionals and industry to report problems with medicines or medical devices. TGA investigates reports received by it to determine any necessary regulatory action. · To report a problem with a medicine or medical device, please see the information on the TGA website < http://www.tga.gov.au>. About AusPARs · An Australian Public Assessment Record (AusPAR) provides information about the evaluation of a prescription medicine and the considerations that led the TGA to approve or not approve a prescription medicine submission. · AusPARs are prepared and published by the TGA. · An AusPAR is prepared for submissions that relate to new chemical entities, generic medicines, major variations, and extensions of indications. · An AusPAR is a static document, in that it will provide information that relates to a submission at a particular point in time. · A new AusPAR will be developed to reflect changes to indications and/or major variations to a prescription medicine subject to evaluation by the TGA. -

Induction with Mitomycin C, Doxorubicin, Cisplatin And
British Journal of Cancer (1999) 80(12), 1962–1967 © 1999 Cancer Research Campaign Article no. bjoc.1999.0627 Induction with mitomycin C, doxorubicin, cisplatin and maintenance with weekly 5-fluorouracil, leucovorin for treatment of metastatic nasopharyngeal carcinoma: a phase II study RL Hong1, TS Sheen2, JY Ko2, MM Hsu2, CC Wang1 and LL Ting3 Departments of 1Oncology, 2Otolaryngology and 3Radiation Therapy, National Taiwan University Hospital, National Taiwan University, No. 7, Chung-Shan South Road, Taipei 10016, Taiwan Summary The combination of cisplatin and 5-fluorouracil (5-FU) (PF) is the most popular regimen for treating metastatic nasopharyngeal carcinoma (NPC) but it is limited by severe stomatitis and chronic cisplatin-related toxicity. A novel approach including induction with mitomycin C, doxorubicin and cisplatin (MAP) and subsequent maintenance with weekly 5-FU and leucovorin (FL) were designed with an aim to reduce acute and chronic toxicity of PF. Thirty-two patients of NPC with measurable metastatic lesions in the liver or lung were entered into this phase II trial. Mitomycin C 8 mg m–2, doxorubicin 40 mg m–2 and cisplatin 60 mg m–2 were given on day 1 every 3 weeks as initial induction. After either four courses or remission was achieved, patients received weekly dose of 5-FU 450 mg m–2 and leucovorin 30 mg m–2 for maintenance until disease progression. With 105 courses of MAP given, 5% were accompanied by grade 3 and 0% were accompanied by grade 4 stomatitis. The dose-limiting toxicity of MAP was myelosuppression. Forty per cent of courses had grade 3 and 13% of courses had grade 4 leukopenia. -

Arsenic Trioxide Is Highly Cytotoxic to Small Cell Lung Carcinoma Cells
160 Arsenic trioxide is highly cytotoxic to small cell lung carcinoma cells 1 1 Helen M. Pettersson, Alexander Pietras, effect of As2O3 on SCLC growth, as suggested by an Matilda Munksgaard Persson,1 Jenny Karlsson,1 increase in neuroendocrine markers in cultured cells. [Mol Leif Johansson,2 Maria C. Shoshan,3 Cancer Ther 2009;8(1):160–70] and Sven Pa˚hlman1 1Center for Molecular Pathology, CREATE Health and 2Division of Introduction Pathology, Department of Laboratory Medicine, Lund University, 3 Lung cancer is the most frequent cause of cancer deaths University Hospital MAS, Malmo¨, Sweden; and Department of f Oncology-Pathology, Cancer Center Karolinska, Karolinska worldwide and results in 1 million deaths each year (1). Institute and Hospital, Stockholm, Sweden Despite novel treatment strategies, the 5-year survival rate of lung cancer patients is only f15%. Small cell lung carcinoma (SCLC) accounts for 15% to 20% of all lung Abstract cancers diagnosed and is a very aggressive malignancy Small cell lung carcinoma (SCLC) is an extremely with early metastatic spread (2). Despite an initially high aggressive form of cancer and current treatment protocols rate of response to chemotherapy, which currently com- are insufficient. SCLC have neuroendocrine characteristics bines a platinum-based drug with another cytotoxic drug and show phenotypical similarities to the childhood tumor (3, 4), relapses occur in the absolute majority of SCLC neuroblastoma. As multidrug-resistant neuroblastoma patients. At relapse, the efficacy of further chemotherapy is cells are highly sensitive to arsenic trioxide (As2O3) poor and the need for alternative treatments is obvious. in vitro and in vivo, we here studied the cytotoxic effects Arsenic-containing compounds have been used in tradi- of As2O3 on SCLC cells. -

NOV 1 72010 1.0 Submitter
510(k) SUMMARY NOV 1 72010 1.0 Submitter Name Shen Wei (USA) Inc. Street Address 33278 Central Ave., Suite 102 Union City, CA. 94587 Phone No. (510)429-8692 Fax No. (510)487-5347 Date of Summary Prepared: 08/12/10 Prepared by: Albert Li 2.0 Name of the device: Glove Proprietary or Trade Name: Blue and Red with Pearlescent® Pigment, Powder Free Nitrile Examination Gloves with Aloe Vera, Tested for use with Chemotherapy Drugs Common Name: Exam gloves Classification Name: Patient examination glove, Specialty Chemotherapy'(per 21 CFR 880.6250 product code LZC) Classification Information: Class I Nitrile patient examination glove 8OLZC, powder-free and meeting all the requirements of ASTM D 631 9-O0a-05 and is tested with chemotherapy drugs according to ASTM D 6978-05. 3.0 Identification of the Legally Marketed Device: Blue and Red with Pearlescent® Pigment, Powder Free Nitrile Examination Gloves with Aloe Vera Regulatory Class I Nitrile patient examination Product code: 8OLZA 5 10(k): K092411 4.0 Description of the Device: Blue and Red with Pearlescent® Pigment, Powder Free Nitrite Examination Gloves with Aloe Vera, Tested for use with Chemotherapy Drugs meets all the requirements of ASTM D 6978-05, ASTM D63 19-00a(2005) and FDA 21 CFT 880.6250. 5.0 Intended Use of Device: Product: Red with Pearlescent® Pigment, Powder Free Nitrile Examination Gloves with Aloe Vera, Tested for use with Chemotherapy Drugs A disposable device intended for medical purpose that is worn on the examiner's hand to prevent contamination between patient and examiner. This device is single use only. -

Primary Central Nervous System Lymphoma: Consolidation Strategies
12 Review Article Page 1 of 12 Primary central nervous system lymphoma: consolidation strategies Carole Soussain1,2, Andrés J. M. Ferreri3 1Division of Hematology, Institut Curie, Site Saint-Cloud, Saint-Cloud, France; 2INSERM U932, Institut Curie, PSL Research University, Paris, France; 3Lymphoma Unit, Department of Onco-Hematology, IRCCS San Raffaele Scientific Institute, Milano, Italy Contributions: (I) Conception and design: All authors; (II) Administrative support: None; (III) Provision of study materials or patients: All authors; (IV) Collection and assembly of data: All authors; (V) Data analysis and interpretation: All authors; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Carole Soussain. Institut Curie, 35 rue Dailly, 92210 Saint-Cloud, France. Email: [email protected]. Abstract: To eliminate residual malignant cells and prevent relapse, consolidation treatment remains an essential part of the first-line treatment of patients with primary central nervous system lymphoma. Conventional whole-brain radiotherapy (WBRT) delivering 36–40 Gy was the first and most used consolidation strategy for decades. It is being abandoned because of the overt risk of neurotoxicity while other consolidation strategies have emerged. Reduced-dose WBRT is effective for reducing the risk of relapse in patients with complete response (CR) after induction chemotherapy compared to patients who did not receive consolidation treatment, with an apparent reduced risk of neurotoxicity, which needs to be confirmed in patients over 60 years of age. Preliminary results showed the feasibility of stereotaxic radiotherapy as an alternative to WBRT. Nonmyeloablative chemotherapy, consisting of high doses of etoposide and cytarabine, has shown encouraging therapeutic results in a phase II study, with a high risk of hematologic and infectious toxicity. -

Combination of Oxoplatin with Other FDA-Approved Oncology Drugs
International Journal of Molecular Sciences Article Theoretical Prediction of Dual-Potency Anti-Tumor Agents: Combination of Oxoplatin with Other FDA-Approved Oncology Drugs José Pedro Cerón-Carrasco Reconocimiento y Encapsulación Molecular, Universidad Católica San Antonio de Murcia Campus los Jerónimos, 30107 Murcia, Spain; [email protected] Received: 16 April 2020; Accepted: 2 July 2020; Published: 3 July 2020 Abstract: Although Pt(II)-based drugs are widely used to treat cancer, very few molecules have been approved for routine use in chemotherapy due to their side-effects on healthy tissues. A new approach to reducing the toxicity of these drugs is generating a prodrug by increasing the oxidation state of the metallic center to Pt(IV), a less reactive form that is only activated once it enters a cell. We used theoretical tools to combine the parent Pt(IV) prodrug, oxoplatin, with the most recent FDA-approved anti-cancer drug set published by the National Institute of Health (NIH). The only prerequisite imposed for the latter was the presence of one carboxylic group in the structure, a chemical feature that ensures a link to the coordination sphere via a simple esterification procedure. Our calculations led to a series of bifunctional prodrugs ranked according to their relative stabilities and activation profiles. Of all the designed molecules, the combination of oxoplatin with aminolevulinic acid as the bioactive ligand emerged as the most promising strategy by which to design enhanced dual-potency oncology drugs. Keywords: cancer; drug design; organometallics; platinum-based drugs; bifunctional compounds; theoretical tools 1. Introduction The unexpected discovery of the bioactivity of Pt salts by Rosenberg about 60 years ago opened the door to a new type of cancer treatment: chemotherapy with transition metals [1]. -
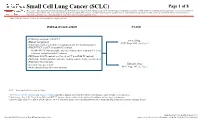
Small Cell Lung Cancer (SCLC) Algorithm
Small Cell Lung Cancer (SCLC) Page 1 of 8 Disclaimer: This algorithm has been developed for MD Anderson using a multidisciplinary approach considering circumstances particular to MD Anderson’s specific patient population, services and structure, and clinical information. This is not intended to replace the independent medical or professional judgment of physicians or other health care providers in the context of individual clinical circumstances to determine a patient's care. This algorithm should not be used to treat pregnant women. Note: Consider Clinical Trials as treatment options for eligible patients. INITIAL EVALUATION STAGE ● Pathology consistent with SCLC Limited Stage ● History and physical AJCC Stage I-III2, see Page 2 ● Laboratory studies to include hematological and full chemistry panels ● FDG PET/CT and CT chest with IV contrast ○ If FDG PET/CT not available: nuclear medicine bone scan and CT chest, abdomen, and pelvis with IV contrast ● MRI brain with IV contrast (preferred) or CT head with IV contrast ● MRI spine, lumbar puncture and bone marrow aspirate/biopsy as indicated ● Pulmonary function tests 1 Extensive Stage ● Lifestyle risk assessment AJCC Stage IV3, see Page 3 ● Molecular profiling (for never smokers) AJCC = American Joint Committee on Cancer 1 See Physical Activity, Nutrition, and Tobacco Cessation algorithms; ongoing reassessment of lifestyle risks should be a part of routine clinical practice 2 Limited stage: Stage I-III (T any, N any, M0) per AJCC 8th edition or disease confined to the ipsilateral hemithorax -

Cisplatin and Etoposide (Lung)
Cisplatin and Etoposide (lung) _____________________________________________________________________________________________ Indication First line chemotherapy for patients with small cell lung cancer (SCLC), who have a good performance status (WHO PS 0-2). Concomitant radiotherapy may start with cycle 2. ICD-10 codes Codes pre-fixed with C34 Regimen details Day Drug Dose Route 1 Cisplatin 75-80mg/m² IV infusion 1 Etoposide 100mg/m² IV infusion 2 and 3 or Etoposide 100mg/m² IV infusion 2 and 3 Etoposide 200mg/m2 PO Cycle frequency 21 days Number of cycles 4 - 6 cycles (usually 4) Administration Cisplatin is administered in 500mL sodium chloride 0.9% over 60 minutes following the pre and post hydration protocol below. Infusion Fluid & Additives Volume Infusion Time Sodium Chloride 0.9% 1000mL 1 hour Mannitol 20% 200mL 30 minutes OR Mannitol 10% 400mL 30 minutes Ensure urine output > 100mL / hour prior to giving cisplatin. Give a single dose of furosemide 20mg iv if necessary. Cisplatin 500mL 1 hour Sodium Chloride 0.9% + 2g MgSO4 + 1000mL 2 hours 20mmol KCl TOTAL 2700mL or 2900mL 4 hours 30 minutes Note: Patients with magnesium or potassium below the normal range should have 2g MgSO4 and 20mmol KCl added to the pre-hydration bag and the duration of the infusion increased to 2 hours. All patients must be advised to drink at least 2 litres of fluid over the following 24 hours. IV etoposide is administered in 1000mL sodium chloride 0.9% and infused over a minimum of 1 hour. Version 1 Review date June 2018 Page 1 of 4 Oral etoposide is available as 50mg and 100mg capsules. -

Pulmonary Toxicity Following Carmustine-Based Preparative Regimens and Autologous Peripheral Blood Progenitor Cell Transplantation in Hematological Malignancies
Bone Marrow Transplantation (2000) 25, 309–313 2000 Macmillan Publishers Ltd All rights reserved 0268–3369/00 $15.00 www.nature.com/bmt Pulmonary toxicity following carmustine-based preparative regimens and autologous peripheral blood progenitor cell transplantation in hematological malignancies EP Alessandrino1, P Bernasconi1, A Colombo1, D Caldera1, G Martinelli1, P Vitulo2, L Malcovati1, C Nascimbene2, M Varettoni1, E Volpini2, C Klersy3 and C Bernasconi1 1Centro Trapianti di Midollo Osseo, Istituto di Ematologia, 2Divisione di Pneumologia, 3Biometry-Scientific Direction IRCCS, Policlinico S Matteo, Pavia, Italy Summary: the use of BCNU is suspected to be caused by damage to the glutathione system.2 BCNU has been included in high- Sixty-five patients with hematological malignancies (25 dose conditioning regimens for gliomas, breast cancer, multiple myeloma, 18 Hodgkin’s disease, 22 non-Hodg- Hodgkin’s disease, non-Hodgkin’s lymphomas, multiple kin’s lymphomas) who received a carmustine-based myeloma. Toxic pulmonary reactions have been recognized regimen followed by autologous PBPC transplantation, in as many as 16–64% of patients;3–13 onset generally were studied retrospectively to evaluate the incidence of occurs within 1 year of starting BCNU. Events occurring post-transplant non-infective pulmonary complications up to 17 years later have been reported.14 The drug seems (NIPCs), risk factors predictive of NIPCs, and response to cause pulmonary damage in a dose-related manner:5,10,11 to steroids. Carmustine (BCNU) given i.v. at a dose of Phillips et al6 reported a 9.5% incidence of fatal pulmonary 600 mg/m2 was combined with etoposide and cyclophos- toxicity in patients receiving BCNU doses as high as 1.200 phamide in 40 patients (BCV regimen) and with etopo- mg/m2 as a single agent; another report suggests no pul- side and melphalan in 25 patients (BEM regimen). -

Adcetris, INN-Brentuximab Vedotin
ANNEX I SUMMARY OF PRODUCT CHARACTERISTICS 1 This medicinal product is subject to additional monitoring. This will allow quick identification of new safety information. Healthcare professionals are asked to report any suspected adverse reactions. See section 4.8 for how to report adverse reactions. 1. NAME OF THE MEDICINAL PRODUCT ADCETRIS 50 mg powder for concentrate for solution for infusion. 2. QUALITATIVE AND QUANTITATIVE COMPOSITION Each vial contains 50 mg of brentuximab vedotin. After reconstitution (see section 6.6), each mL contains 5 mg of brentuximab vedotin. ADCETRIS is an antibody-drug conjugate composed of a CD30-directed monoclonal antibody (recombinant chimeric immunoglobulin G1 [IgG1], produced by recombinant DNA technology in Chinese Hamster ovary cells) that is covalently linked to the antimicrotubule agent monomethyl auristatin E (MMAE). Excipient with known effect Each vial contains approximately 13.2 mg of sodium. For the full list of excipients, see section 6.1. 3. PHARMACEUTICAL FORM Powder for concentrate for solution for infusion. White to off-white cake or powder. 4. CLINICAL PARTICULARS 4.1 Therapeutic indications Hodgkin lymphoma ADCETRIS is indicated for adult patients with previously untreated CD30+ Stage IV Hodgkin lymphoma (HL) in combination with doxorubicin, vinblastine and dacarbazine (AVD) (see sections 4.2 and 5.1). ADCETRIS is indicated for the treatment of adult patients with CD30+ HL at increased risk of relapse or progression following autologous stem cell transplant (ASCT) (see section 5.1). ADCETRIS is indicated for the treatment of adult patients with relapsed or refractory CD30+ Hodgkin lymphoma (HL): 1. following ASCT, or 2. following at least two prior therapies when ASCT or multi-agent chemotherapy is not a treatment option. -

Wear the Battle Gear That Protects Against 52 Chemotherapy Drugs!
YOU’RE FIGHTING CANCER. Wear the Battle Gear That Protects Against 52 Chemotherapy Drugs! PURPLE NITRILE-XTRA* Gloves and HALYARD* Procedure Gowns for Chemotherapy Use have been tested It’s 52 vs. You. for resistance to 52 chemotherapy drugs.† Arsenic Trioxide (1 mg/ml) Cyclophosphamide (20 mg/ml) Fludarabine (25 mg/ml) Mitomycin (0.5 mg/ml) Temsirolimus (25 mg/ml) Azacitidine (Vidaza) (25 mg/ml) Cytarabine HCl (100 mg/ml) Fluorouracil (50 mg/ml) Mitoxantrone (2 mg/ml) Trastuzumab (21 mg/ml) Bendamustine (5 mg/ml) Cytovene (10 mg/ml) Fulvestrant (50 mg/ml) Oxaliplatin (2 mg/ml) ThioTEPA (10 mg/ml) Bleomycin Sulfate (15 mg/ml) Dacarbazine (10 mg/ml) Gemcitabine (38 mg/ml) Paclitaxel (6 mg/ml) Topotecan HCl (1 mg/ml) Bortezomib (Velcade) (1 mg/ml) Daunorubicin HCl (5 mg/ml) Idarubicin (1 mg/ml) Paraplatin (10 mg/ml) Triclosan (1 mg/ml) Busulfan (6 mg/ml) Decitabine (5 mg/ml) Ifosfamide (50 mg/ml) Pemetrexed (25 mg/ml) Trisenox (0.1 mg/ml) Carboplatin (10 mg/ml) Docetaxel (10 mg/ml) Irinotecan (20 mg/ml) Pertuzumab (30 mg/ml) Vincrinstine Sulfate (1 mg/ml) Carfilzomib (2 mg/ml) Doxorubicin HCl (2 mg/ml) Mechlorethamine HCl (1 mg/ml) Raltitrexed (0.5 mg/ml) Vinblastine (1 mg/ml) Carmustine (3.3 mg/ml)† Ellence (2 mg/ml) Melphalan (5 mg/ml) Retrovir (10 mg/ml) Vinorelbine (10 mg/ml) Cetuximab (Erbitux) (2 mg/ml) Eribulin Mesylate (0.5 mg/ml) Methotrexate (25 mg/ml) Rituximab (10 mg/ml) Zoledronic Acid (0.8 mg/ml) Cisplatin (1 mg/ml) Etoposide (20 mg/ml) † Testing measured no breakthrough at the Standard Breakthrough Rate of 0.1ug/cm2/minute, up to 240 minutes for gloves and 480 minutes for gowns, except for carmustine. -

The Effects of the Nanosphere Carrier for the Combined Carmustine-Busulfan Trastuzumab in Human Breast Cancer Tissue Culture
Sahib et al (2019): Nanosphere carrier in human breast cancer November 2019 Vol. 22 (7) The effects of the nanosphere carrier for the combined carmustine-busulfan trastuzumab in human breast cancer tissue culture Zena Hasan Sahib 1 , Sarmad Nory Gany Al-Dujaili 1 , Hussein Abdulkadhim 1 , Rana A. Ghaleb 2 1 Department of Pharmacology and Therapeutics, College of Medicine, University of Kufa 2 Department of Anatomy and Histology, College of medicine, University of Babylon Corresponding author email: [email protected] Abstract Cancer of the breast is from the highest cancer type’s incidence. Cancer in general represents a high therapeutic challenge. Considerable adverse effects and cytotoxicity of highly potent drugs for healthy tissue require the development of novel drug delivery systems to improve pharmacokinetics and result in selective distribution of the loaded agent. Targeted therapy is a novel maneuver to achieve proper selectivity index. And as the main goal of nanocarriers is to target specific sites and improve the circulation time of the drug which is entrapped, encapsulate or conjugate in the carrier system so we chose nanoliposome as a drug carrier. Liposomes improved a potent drug targeting successfully in the last decade, but nanoliposomes offer more surface area and they have more solubility, improve controlled release, enhance bioavailability, and permit precision targeting of the material that is encapsulated to a greater extent. The Aims and objectives of the study is the formulation of HER2 Ab directed nanosphere carrier for a combined Carmustine-busulfan and trastuzumab (LCBT), then Assessing antineoplastic efficacy of (LCBT) in lung carcinoma cell line. A dose-dependent cellular growth inhibition on all three cell lines (P-value < 0.001) was seen.