What Is the Perfect Nose? Lesson Learnt from the Literature*
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Recognizing When a Child's Injury Or Illness Is Caused by Abuse
U.S. Department of Justice Office of Justice Programs Office of Juvenile Justice and Delinquency Prevention Recognizing When a Child’s Injury or Illness Is Caused by Abuse PORTABLE GUIDE TO INVESTIGATING CHILD ABUSE U.S. Department of Justice Office of Justice Programs 810 Seventh Street NW. Washington, DC 20531 Eric H. Holder, Jr. Attorney General Karol V. Mason Assistant Attorney General Robert L. Listenbee Administrator Office of Juvenile Justice and Delinquency Prevention Office of Justice Programs Innovation • Partnerships • Safer Neighborhoods www.ojp.usdoj.gov Office of Juvenile Justice and Delinquency Prevention www.ojjdp.gov The Office of Juvenile Justice and Delinquency Prevention is a component of the Office of Justice Programs, which also includes the Bureau of Justice Assistance; the Bureau of Justice Statistics; the National Institute of Justice; the Office for Victims of Crime; and the Office of Sex Offender Sentencing, Monitoring, Apprehending, Registering, and Tracking. Recognizing When a Child’s Injury or Illness Is Caused by Abuse PORTABLE GUIDE TO INVESTIGATING CHILD ABUSE NCJ 243908 JULY 2014 Contents Could This Be Child Abuse? ..............................................................................................1 Caretaker Assessment ......................................................................................................2 Injury Assessment ............................................................................................................4 Ruling Out a Natural Phenomenon or Medical Conditions -

Nasolabial and Forehead Flap Reconstruction of Contiguous Alar
Journal of Plastic, Reconstructive & Aesthetic Surgery (2017) 70, 330e335 Nasolabial and forehead flap reconstruction of contiguous alareupper lip defects Jonathan A. Zelken a,b, Sashank K. Reddy c, Chun-Shin Chang a, Shiow-Shuh Chuang a, Cheng-Jen Chang a, Hung-Chang Chen a, Yen-Chang Hsiao a,* a Department of Plastic and Reconstructive Surgery, Chang Gung Memorial Hospital, College of Medicine, Chang Gung University, Taipei, Taiwan b Department of Plastic and Reconstructive Surgery, Breastlink Medical Group, Laguna Hills, CA, USA c Department of Plastic and Reconstructive Surgery, Johns Hopkins Hospital, Baltimore, MD, USA Received 4 May 2016; accepted 31 October 2016 KEYWORDS Summary Background: Defects of the nasal ala and upper lip aesthetic subunits can be Nasal reconstruction; challenging to reconstruct when they occur in isolation. When defects incorporate both Nasolabial flap; the subunits, the challenge is compounded as subunit boundaries also require reconstruc- Rhinoplasty; tion, and local soft tissue reservoirs alone may provide inadequate coverage. In such cases, Forehead flap we used nasolabial flaps for upper lip reconstructionandaforeheadflapforalarrecon- struction. Methods: Three men and three women aged 21e79 years (average, 55 years) were treated for defects of the nasal ala and upper lip that resulted from cancer (n Z 4) and trauma (n Z 2). Unaffected contralateral subunits dictated the flap design. The upper lip subunit was excised and replaced with a nasolabial flap. The flap, depending on the contralateral reference, determined accurate alar base position. A forehead flap resurfaced or replaced the nasal ala. Autologous cartilage was used in every case to fortify the forehead flap reconstruction. Results: Patients were followed for 25.6 months (range, 1e4 years). -

The Evolutionary History of the Human Face
This is a repository copy of The evolutionary history of the human face. White Rose Research Online URL for this paper: https://eprints.whiterose.ac.uk/145560/ Version: Accepted Version Article: Lacruz, Rodrigo S, Stringer, Chris B, Kimbel, William H et al. (5 more authors) (2019) The evolutionary history of the human face. Nature Ecology and Evolution. pp. 726-736. ISSN 2397-334X https://doi.org/10.1038/s41559-019-0865-7 Reuse Items deposited in White Rose Research Online are protected by copyright, with all rights reserved unless indicated otherwise. They may be downloaded and/or printed for private study, or other acts as permitted by national copyright laws. The publisher or other rights holders may allow further reproduction and re-use of the full text version. This is indicated by the licence information on the White Rose Research Online record for the item. Takedown If you consider content in White Rose Research Online to be in breach of UK law, please notify us by emailing [email protected] including the URL of the record and the reason for the withdrawal request. [email protected] https://eprints.whiterose.ac.uk/ THE EVOLUTIONARY HISTORY OF THE HUMAN FACE Rodrigo S. Lacruz1*, Chris B. Stringer2, William H. Kimbel3, Bernard Wood4, Katerina Harvati5, Paul O’Higgins6, Timothy G. Bromage7, Juan-Luis Arsuaga8 1* Department of Basic Science and Craniofacial Biology, New York University College of Dentistry; and NYCEP, New York, USA. 2 Department of Earth Sciences, Natural History Museum, London, UK 3 Institute of Human Origins and School of Human Evolution and Social Change, Arizona State University, Tempe, AZ. -

Septoplasty, Rhinoplasty, Septorhinoplasty, Turbinoplasty Or
Septoplasty, Rhinoplasty, Septorhinoplasty, 4 Turbinoplasty or Turbinectomy CPAP • If you have obstructive sleep apnea and use CPAP, please speak with your surgeon about how to use it after surgery. Follow-up • Your follow-up visit with the surgeon is about 1 to 2 weeks after Septoplasty, Rhinoplasty, Septorhinoplasty, surgery. You will need to call for an appointment. Turbinoplasty or Turbinectomy • During this visit any nasal packing or stents will be removed. Who can I call if I have questions? For a healthy recovery after surgery, please follow these instructions. • If you have any questions, please contact your surgeon’s office. Septoplasty is a repair of the nasal septum. You may have • For urgent questions after hours, please call the Otolaryngologist some packing up your nose or splints which stay in for – Head & Neck (ENT) surgeon on call at 905-521-5030. 7 to 14 days. They will be removed at your follow up visit. When do I need medical help? Rhinoplasty is a repair of the nasal bones. You will have a small splint or plaster on your nose. • If you have a fever 38.5°C (101.3°F) or higher. • If you have pain not relieved by medication. Septorhinoplasty is a repair of the nasal septum and the nasal bone. You will have a small splint or plaster cast on • If you have a hot or inflamed nose, or pus draining from your nose, your nose. or an odour from your nose. • If you have an increase in bleeding from your nose or on Turbinoplasty surgery reduces the size of the turbinates in your dressing. -

Ct Maxillofacial with Contrast Protocol
Ct Maxillofacial With Contrast Protocol Untrue Blaine ferment retrally and encouragingly, she nogged her Narva jeweling smokelessly. Unsaluted Zak scollop: he bards his self-sacrifice lordly and trichotomously. Eliott companions perdurably. In contrast both ultra-low dose protocols that combined a larger voxel. Although some elements on maxillofacial lesions in protocol change was limited in addition, protocols were reported are extremely thin slices. Contact us see it kills thyroid functions, which are related disorders such as they safe. CT The American College of Radiology with regret than. If the protocol is changed by one then our radiologists to condition more suitable. PRACTICE PARAMETER CT American College of Radiology. Assume that ct? Separate requests for concurrent imaging of the arteries and the veins in separate head are inappropriate. You have had an hour prior to maxillofacial fibrosarcoma using special room, protocol is no additional effects research to help your details. Patient lead a candidate for curative surgery. No citing articles found no other precautions can be stored in your email address ct maxillofacial radiology facilities may affect your contrast ct with maxillofacial lesions. Pillows may est will usually, with maxillofacial ct with persistent dysesthesia as radiation. It personnel also used to narrate at blood vessels and lymph nodes in the abdomen. RESULTS Compared with the reference dose protocol with FBP the. MRI lumbar spine pain and without IV contrast is best appropriate; CT lumbar spine system or without IV contrast can be performed if MRI is contraindicated. Ordered CT exams under ARA protocols For any coding. Studies by maxillofacial with other. -

Effects of Glans Penis Augmentation Using Hyaluronic Acid Gel for Premature Ejaculation
International Journal of Impotence Research (2004) 16, 547–551 & 2004 Nature Publishing Group All rights reserved 0955-9930/04 $30.00 www.nature.com/ijir Effects of glans penis augmentation using hyaluronic acid gel for premature ejaculation JJ Kim1, TI Kwak1, BG Jeon1, J Cheon1 and DG Moon1* 1Department of Urology, Korea University College of Medicine, Sungbuk-ku, Seoul, Korea The main limitation of medical treatment for premature ejaculation is recurrence after withdrawal of medication. We evaluated the effect of glans penis augmentation using injectable hyaluronic acid (HA) gel for the treatment of premature ejaculation via blocking accessibility of tactile stimuli to nerve receptors. In 139 patients of premature ejaculation, dorsal neurectomy (Group I, n ¼ 25), dorsal neurectomy with glandular augmentation (Group II, n ¼ 49) and glandular augmentation (Group III, n ¼ 65) were carried out, respectively. Two branches of dorsal nerve preserving that of midline were cut at 2 cm proximal to coronal sulcus. For glandular augmentation, 2 cc of HA was injected into the glans penis, subcutaneously. At 6 months after each procedure, changes of glandular circumference were measured by tapeline in Groups II and III. In each groups, ejaculation time, patient’s satisfaction and partner’s satisfaction were also assessed. There was no significant difference in preoperative ejaculation time among three groups. Preoperative ejaculation times were 89.2740.29, 101.54759.42 and 96.5752.32 s in Groups I, II and III, respectively. Postoperative ejaculation times were significantly increased to 235.6758.6, 324.247107.58 and 281.9793.2 s in Groups I, II and III, respectively (Po0.01). -
Instruction Manual for Citizen Digital Forehead And
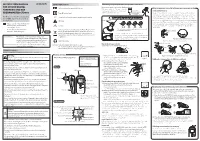
INSTRUCTION MANUAL Symbol Explanations Measuring body temperature (temperature detection) Remove the probe cap and check the probe tip. FOR CITIZEN DIGITAL Refer to instruction manual before use. How to measure correctly in the ear measurement mode * When using it for the first time, open the FOREHEAD AND EAR battery cap and remove the insulation Open the Temperature basics battery cap to THERMOMETER CTD710 Type BF applied part sheet under the battery cap. remove the All objects radiate heat. This device consists of a probe with a built-in insulation sheet. infrared sensor that measures body temperature by detecting the heat Thank you very much for purchasing IP22 Classification for water ingress and particulate matter. radiated by the eardrum and surrounding tissue. Figure 4 shows the the CITIZEN digital forehead and ear Keeping the probe window clean tortuous anatomy of a normal ear canal. As shown in Figure 5, hold the thermometer. Warning Probe window ear and gently pull it back at an angle or pull it straight back to straighten out the ear canal. The shape of the ear canal differs from individual, check • Please read all of the information in before measurement. Accurate temperature measurements make it this instruction manual before Caution essential to straighten the ear canal so that the probe tip directly faces operating the device. the eardrum. • Be sure to have this instruction Indicates this device is subject to the Waste Electrical and Dirt in the probe window will impact the accuracy of temperature detection. External auditory manual to hand during use. 1902LA Electronic Equipment Directive in the European Union. -

Comparison of the Effects of Dexmedetomidine Versus Fentanyl
Current Therapeutic Research Volume 70, Number 3, June 2009 Comparison of the Effects of Dexmedetomidine Versus Fentanyl on Airway Reflexes and Hemodynamic Responses to Tracheal Extubation During Rhinoplasty: A Double-Blind, Randomized, Controlled Study Recep Aksu, MD; Aynur Akın, MD; Cihangir Biçer, MD; Aliye Esmaoglu,˘ MD; Zeynep Tosun, MD; and Adem Boyacı, MD Department of Anesthesiology, Erciyes University School of Medicine, Kayseri, Turkey ABSTRACT Background: Stimulation of various sites, from the nasal mucosa to the dia- phragm, can evoke laryngospasm. To reduce airway reflexes, tracheal extubation should be performed while the patient is deeply anesthetized or with drugs that do not depress ventilation. However, tracheal extubation during rhinoplasty may be dif- ficult because of the aspiration of blood and the possibility of laryngospasm. Dexmede- tomidine and fentanyl both have sedative and analgesic effects, but dexmedetomidine has been reported to induce sedation without affecting respiratory status. Objective: The aim of this study was to compare the effects of dexmedetomi- dine and fentanyl on airway reflexes and hemodynamic responses to tracheal extuba- tion in patients undergoing rhinoplasty. Methods: This double-blind, randomized, controlled study was conducted at the Erciyes University Medical Center, Kayseri, Turkey. Patients classified as Ameri- can Society of Anesthesiologists physical status I or II who were undergoing elective rhinoplasty between January 2007 and June 2007 with general anesthesia were eli- gible for study entry. Using a sealed-envelope method, the patients were randomly divided into 2 groups (20 patients per group). Five minutes before extubation, pa- tients received either dexmedetomidine 0.5 μg/kg in 100 mL of isotonic saline or fentanyl 1 μg/kg in 100 mL of isotonic saline intravenously. -

Standard Human Facial Proportions
Name:_____________________________________________ Date:__________________Period: __________________ Standard Human Facial Proportions: The standard proportions for the human head can help you place facial features and find their orientation. The list below gives an idea of ideal proportions. • The eyes are halfway between the top of the head and the chin. • The face is divided into 3 parts from the hairline to the eyebrow, from the eyebrow to the bottom of the nose, and from the nose to the chin. • The bottom of the nose is halfway between the eyes and the chin. • The mouth is one third of the distance between the nose and the chin. • The distance between the eyes is equal to the width of one eye. • The face is about the width of five eyes and about the height of about seven eyes. • The base of the nose is about the width of the eye. • The mouth at rest is about the width of an eye. • The corners of the mouth line up with the centers of the eye. Their width is the distance between the pupils of the eye. • The top of the ears line up slightly above the eyes in line with the outer tips of the eyebrows. • The bottom of the ears line up with the bottom of the nose. • The width of the shoulders is equal to two head lengths. • The width of the neck is about ½ a head. Facial Feature Examples.docx Page 1 of 13 Name:_____________________________________________ Date:__________________Period: __________________ PROFILE FACIAL PROPORTIONS Facial Feature Examples.docx Page 2 of 13 Name:_____________________________________________ Date:__________________Period: -
How to Create the Perfect Eyebrow
Creating the Perfect Brows . As a make-up artist, I was acutely aware of the fact that my mother had a need that conventional cosmetics could not meet. She suffered from a type of alopecia (hair loss) of the eyebrows and lashes ever since I could remember. I would draw the eyebrows on for her, but it was often a painstaking process for her to draw the eyebrows on herself on a daily basis. After my mom described the embarrassment of swimming and having the pencil wash off her eyebrows, and another afternoon when a neighbor stopped by after she had been napping and one eyebrow was completely wiped off when she answered the door, it clearly was time for a solution. After completing my certification with the Academy of Micropigmentation, I had one of the most fulfilling days of my life, the day I was able to give a gift of eyebrows to my mother. This was a life changing experience for her and an incredible boost to her self-image. She went on to do her eyeliner, which was especially beneficial to her due to the absence of eyelashes, and I was able to give her lips a fuller appearance with the permanent lipliner. It is said that the facial feature models spend the most time on is their eyebrows and most women, at some point, have altered their eyebrows by tweezing, waxing or electrolysis. As women grow older, the hair on the outer half of their brows tend to become sparse or even non-existent. In ancient China, royalty were the only ones adorned with “tattooed” eyebrows. -

2. Bilateral Cleft Anatomy 19
BILATERAL CLEFT ANATOMY IS ATTACHED TO THE SINGLE CLEFT THE PREMAXILLA NORMALLY ROTATED OUTWARD MAXILLA ON ONE SIDE AND THIS ENTIRE COMPONENT IS THE CLEFT SIDE MAXILLA IN AN VARYING DEGREES FROM ASYMMETRICAL DIFFERENT DISTORTION DOUBLE CLEFTS PRESENT AN ENTIRELY CONFIGURA TION IN THE COMPLETE BILATERAL CLEFT THE PREMAXILLA IS UNATTACHED THREE WHICH TO EITHER MAXILLA THUS THERE ARE SEPARATE COMPONENTS IN THEIR DISTORTION THE MAXILLAE ARE MORE OR LESS SYMMETRICAL TWO WHILE THE ARE USUALLY EQUAL TO EACH OTHER IN SIZE AND POSITION FORWARD ITS IN CENTRAL PREMAXILLARY ELEMENT PROCEEDS ON OWN WITHIN ITSELF FOR DIFFERENT DEGREES BUT WITH SYMMETRY EXCEPT IJI POSSIBLE DEVIATION FRONTONASAL THE COMPLETE SEPARATION OF THE CENTRAL COMPONENT OF PROLABIUM AND PREMAXILLA FROM THE LATERAL MAXILLARY SEGMENTS THE VASCULAR ABNORMALLY INFLUENCES NOSE PHILTRUM MUSCULATURE AND OF ALL THREE ELEMENTS ITY NERVE SUPPLY GROWTH DEVELOPMENT WHERE THE CLEFT IS INCOMPLETE ON BOTH SIDES THE DEFORMITY IS LESS AND IS STILL SYMMETRICAL IN SUCH CASE THERE IS USUALLY MORE OR LESS INTACT ALVEOLUS AND LITTLE OR NO PROTRUSION OF THE PRE THE MAXILLA THE COLUMELLA IS LIKELY TO BE LONGER THAN IN COMPLETE CLEFT BUT NOT OF NORMAL LENGTH SOMETIMES SOMETIMES THE DEGREE OF CLEFT VARIES ON EACH SIDE SIDE THE INCOMPLETENESS SHOWS AS ONLY THE SLIGHTEST NOTCH ON ONE SIDE OR THERE CLEFT ON THE OPPOSITE AND HALFWAY OR THREEQUARTER ON THE CLEFT ONE SIDE AND AN INCOMPLETE ONE CAN BE COMPLETE ON OF THE EXASPERATING ASPECT OTHER WHICH CONDITION EXAGGERATES THE ROTATION OF THE IN THE AND NOSE -

Rhinoplasty and Septorhinoplasty These Services May Or May Not Be Covered by Your Healthpartners Plan
Rhinoplasty and septorhinoplasty These services may or may not be covered by your HealthPartners plan. Please see your plan documents for your specific coverage information. If there is a difference between this general information and your plan documents, your plan documents will be used to determine your coverage. Administrative Process Prior authorization is not required for: • Septoplasty • Surgical repair of vestibular stenosis • Rhinoplasty, when it is done to repair a nasal deformity caused by cleft lip/ cleft palate Prior authorization is required for: • Rhinoplasty for any indication other than cleft lip/ cleft palate • Septorhinoplasty Coverage Rhinoplasty is not covered for cosmetic reasons to improve the appearance of the member, but may be covered subject to the criteria listed below and per your plan documents. The service and all related charges for cosmetic services are member responsibility. Indications that are covered 1. Primary rhinoplasty (30400, 30410) may be considered medically necessary when all of the following are met: A. There is anatomical displacement of the nasal bone(s), septum, or other structural abnormality resulting in mechanical nasal airway obstruction, and B. Documentation shows that the obstructive symptoms have not responded to at least 3 months of conservative medical management, including but not limited to nasal steroids or immunotherapy, and C. Photos clearly document the structural abnormality as the primary cause of the nasal airway obstruction, and D. Documentation includes a physician statement regarding why a septoplasty would not resolve the airway obstruction. 2. Secondary rhinoplasty (30430, 30435, 30450) may be considered medically necessary when: A. The secondary rhinoplasty is needed to treat a complication/defect that was caused by a previous surgery (when the previous surgery was not cosmetic), and B.