Report of Profiles of Slums/Underserved Areas of 08
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Economics of Slums in the Developing World
The Economics of Slums in the Developing World The MIT Faculty has made this article openly available. Please share how this access benefits you. Your story matters. Citation Marx, Benjamin, Thomas Stoker, and Tavneet Suri. “The Economics of Slums in the Developing World.” Journal of Economic Perspectives 27, no. 4 (November 2013): 187–210. As Published http://dx.doi.org/10.1257/jep.27.4.187 Publisher American Economic Association Version Final published version Citable link http://hdl.handle.net/1721.1/88128 Terms of Use Article is made available in accordance with the publisher's policy and may be subject to US copyright law. Please refer to the publisher's site for terms of use. Journal of Economic Perspectives—Volume 27, Number 4—Fall 2013—Pages 187–210 The Economics of Slums in the Developing World† Benjamin Marx, Thomas Stoker, and Tavneet Suri rrbanban ppopulationsopulations hhaveave sskyrocketedkyrocketed ggloballylobally aandnd ttodayoday rrepresentepresent mmoreore tthanhan hhalfalf ooff tthehe wworld’sorld’s ppopulation.opulation. IInn somesome ppartsarts ooff tthehe ddevelopingeveloping wworld,orld, tthishis U ggrowthrowth hhasas mmore-than-proportionatelyore-than-proportionately iinvolvednvolved rruralural mmigrationigration ttoo iinformalnformal ssettlementsettlements iinn aandnd aaroundround ccities,ities, kknownnown mmoreore ccommonlyommonly aass ““slums”—slums”— ddenselyensely ppopulatedopulated uurbanrban aareasreas ccharacterizedharacterized bbyy ppoor-qualityoor-quality hhousing,ousing, a llackack ooff aadequatedequate llivingiving sspacepace aandnd ppublicublic sservices,ervices, aandnd aaccommodatingccommodating llargearge nnumbersumbers ooff iinformalnformal rresidentsesidents wwithith ggenerallyenerally iinsecurensecure ttenure.enure.1 WWorldwide,orldwide, aatt lleasteast 8860 million60 million ppeopleeople aarere nnowow llivingiving iinn sslums,lums, aandnd tthehe nnumberumber ooff sslumlum ddwellerswellers ggrewrew bbyy ssix millionix million eeachach yyearear ffromrom 22000000 ttoo 22010010 ((UN-HabitatUN-Habitat 22012a).012a). -

Order Sheet in the Islamabad High Court, Islamabad
Form No: HCJD/C-121 ORDER SHEET IN THE ISLAMABAD HIGH COURT, ISLAMABAD (JUDICIAL DEPARTMENT) W. P. No.676/2017 Shahzada Sikandar ul Mulk & 4 others Versus The Capital Development Authority & 4 others Petitioners by : Dr. Muhammad Aslam Khakhi, Advocate. Syed Asghar Hussain Sabwari, Advocate. Dr Babar Awan, Advocate. Mr Sajjar Abbas Hamdani, Advocate. Mr Qausain Faisal Mufti, Advocate. Mr Tajammal Hussain Lathi, Advocate. Malik Zafar Husain, Advocate. Mr Ishtiaq Ahmed Raja, Advocate. Ms Kalsoom Rafique, Advocate. Ms Yasmin Haider, Advocate. Respondents by : Mr Fiaz Ahmed Anjum Jandran, Advocate. Mr Babar Sattar, Advocate. Mr Sultan Mazhar Sher, Advocate. Mr Waqar Hassan Janjua, Advocate. Malik Qamar Afzal, Advocate. Mr Khurram Mehmood Qureshi, Advocate. Mr Muhammad Anwar Mughal, Advocate. Ch. Hafeez Ullah Yaqoob, Advocate. Mr Muhammad Waqas Malik, Advocate. Mr Amjad Zaman, Advocate. Mr Muhammad Khalid Zaman, Advocate. Mr Mujeeb ur Rehman Kiani, Advocate. Barrister Jehangir Khan Jadoon, Advocate. Malik Mazhar Javed, Advocate. Raja Inam Amin Minhas, Advocate. Ch. Waqas Zamir, Advocate. Fazal ur Rehman, Advocate. Ms Zaitoon Hafeez, Advocate. -2- W.P No.676/2017 Ms Zainab Janjua, Advocate. Barrister Amna Abbas, Advocate. Ms Ayesha Ahmed, Advocate. Mr Kashif Ali Malik, Advocate. Mr Amir Latif Gill, Advocate. Mr Tariq Mehmood Jehangiri, Advocate General, Islamabad Capital Territory. Mr Awais Haider Malik, State Counsel. Mr Asad Mehboob Kiyani, Member (P&D), Mr Zafar Iqbal, Director (Master Plan), Mr Faraz Malik, Director (HS), Sh. Ijaz, Director (Urban Planning), Mr Arshad Chohan, Director (Rural Planning), for Capital Development Authority. Mr Mehrban Ali, & Arbab Ali, Zoologists on behalf of Secretary, M/o Climate Change. Date of Hearing : 19-04-2018. -
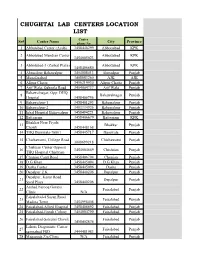
Chughtai Lab Centers Location List
CHUGHTAI LAB CENTERS LOCATION LIST Center Sr# Center Name City Province phone No 1 Abbotabad Center (Ayub) 3458448299 Abbottabad KPK 2 Abbotabad Mandian Center Abbottabad KPK 3454005023 3 Abbotabad-3 (Zarbat Plaza) Abbottabad KPK 3458406680 4 Ahmedpur Bahawalpur 3454008413 Ahmedpur Punjab 5 Muzafarabad 3408883260 AJK AJK 6 Alipur Chatta 3456219930 Alipur Chatta Punjab 7 Arif Wala, Qaboola Road 3454004737 Arif Wala Punjab Bahawalnagar, Opp: DHQ 8 Bahawalnagar Punjab Hospital 3458406756 9 Bahawalpur-1 3458401293 Bahawalpur Punjab 10 Bahawalpur-2 3403334926 Bahawalpur Punjab 11 Iqbal Hospital Bahawalpur 3458494221 Bahawalpur Punjab 12 Battgaram 3458406679 Battgaram KPK Bhakhar Near Piyala 13 Bhakkar Punjab Chowk 3458448168 14 THQ Burewala-76001 3458445717 Burewala Punjab 15 Chichawatni, College Road Chichawatni Punjab 3008699218 Chishtian Center Opposit 16 3454004669 Chishtian Punjab THQ Hospital Chishtian 17 Chunian Cantt Road 3458406794 Chunian Punjab 18 D.G Khan 3458445094 D.G Khan Punjab 19 Daska Center 3458445096 Daska Punjab 20 Depalpur Z.K 3458440206 Depalpur Punjab Depalpur, Kasur Road 21 Depalpur Punjab Syed Plaza 3458440206 Arshad Farooq Goraya 22 Faisalabad Punjab Clinic N/A Faisalabad-4 Susan Road 23 Faisalabad Punjab Madina Town 3454998408 24 Faisalabad-Allied Hospital 3458406692 Faisalabad Punjab 25 Faisalabad-Jinnah Colony 3454004790 Faisalabad Punjab 26 Faisalabad-Saleemi Chowk Faisalabad Punjab 3458402874 Lahore Diagonistic Center 27 Faisalabad Punjab samnabad FSD 3444481983 28 Maqsooda Zia Clinic N/A Faisalabad Punjab Farooqabad, -

S.No Institutename Enrolled Appeared Passed Promoted Fail Absent Percen
FEDERAL DIRECTORATE OF EDUCATION EXAMINATION SECTION Centralized Annual Examination Class-V,2017 **** INSTITUTION WISE RESULT BRIEFPASS/PROMOTED/FAILED/PASS PERCENTAGE/GRADES/GPA S.No InstituteName Enrolled Appeared Passed Promoted Fail Absent Percen. GPA 1 Islamabad College for Boys G-6/3, Islamabad. 349 348 314 32 2 1 99.43 4.18 2 Islamabad Model College for Boys F-7/3, Islamabad. 184 180 162 15 3 4 98.33 3.68 3 Islamabad Model College for Boys F-8/4, Islamabad. 172 171 158 12 1 1 99.42 4.50 4 Islamabad Model College for Boys I-8/3, Islamabad. 129 128 106 18 4 1 96.88 3.41 5 Islamabad Model College for Boys I-10/1, Islamabad. 145 145 142 3 0 0 100.00 4.54 6 Islamabad Model College for Boys G-10/4, Islamabad. 196 194 192 2 0 2 100.00 4.82 7 Islamabad Model College for Boys G-11/1, Islamabad. 75 75 54 15 6 0 92.00 2.79 8 Islamabad Model School ( I-V ) G-11/1, Islamabad. 65 65 50 15 0 0 100.00 2.85 9 Islamabad Model College for Boys F-10/3, Islamabad. 74 73 65 6 2 1 97.26 3.82 10 Islamabad Model School ( I-V ) F-10/1, Islamabad. 26 26 21 4 1 0 96.15 3.65 11 Islamabad Model School ( I-V ) F-10/2, Islamabad. 37 37 31 4 2 0 94.59 3.16 12 Islamabad Model School ( I-V ) F-10/4, Islamabad. -

Survey of Ecotourism Potential in Pakistan's Biodiversity Project Area (Chitral and Northern Areas): Consultancy Report for IU
Survey of ecotourism potential in Pakistan’s biodiversity project area (Chitral and northern areas): Consultancy report for IUCN Pakistan John Mock and Kimberley O'Neil 1996 Keywords: conservation, development, biodiversity, ecotourism, trekking, environmental impacts, environmental degradation, deforestation, code of conduct, policies, Chitral, Pakistan. 1.0.0. Introduction In Pakistan, the National Tourism Policy and the National Conservation Strategy emphasize the crucial interdependence between tourism and the environment. Tourism has a significant impact upon the physical and social environment, while, at the same time, tourism's success depends on the continued well-being of the environment. Because the physical and social environment constitutes the resource base for tourism, tourism has a vested interest in conserving and strengthening this resource base. Hence, conserving and strengthening biodiversity can be said to hold the key to tourism's success. The interdependence between tourism and the environment is recognized worldwide. A recent survey by the Industry and Environment Office of the United Nations Environment Programme (UNEP/IE) shows that the resource most essential for the growth of tourism is the environment (UNEP 1995:7). Tourism is an environmentally-sensitive industry whose growth is dependent upon the quality of the environment. Tourism growth will cease when negative environmental effects diminish the tourism experience. By providing rural communities with the skills to manage the environment, the GEF/UNDP funded project "Maintaining Biodiversity in Pakistan with Rural Community Development" (Biodiversity Project), intends to involve local communities in tourism development. The Biodiversity Project also recognizes the potential need to involve private companies in the implementation of tourism plans (PC II:9). -

PRCS Sitrep No.6, Monsoon Floods 15Th Sep, 14
MONSOON 2014 Info Report - 6: Dated 15-09-14 18-09- HIGHLIGHT Forecast from Pakistan Meteorological Department says “Seasonal low lies over north Baluchistan and adjoining areas. A shallow trough of westerly wave is also prevailing over Kashmir and adjoining areas”. As per the report of NDMA dated 14th September, 2014, Monsoon rains have affected 2,459,704 individuals caused 301 deaths and 507 people got injured in AJK, Punjab and GB. As per UNOCH report of 11th September, the authorities expect an estimated 3 million people to be affected by the floods in the coming days. PRCS is responding in Punjab, AJK, GB and Sindh with an initial plan to assist 13,000 families (91,000 indiv), with provision of food, non food items, emergency shelter and health and care services. In Punjab three PRCS health units have already started working and disaster preparedness stocks are being sent to the affected districts for distribution. So far PRCS Punjab Provincial Branch has distributed 2,350 x food packs to the flood affected families of Jhang, Sialkot, Shikarpur, Chinniot, Gujrat, Hafizabad and Toba Take Singh. In GB 70 x NFIs have been distributed among the flood affected families of Astor District. In AJK 840 families have been assisted with provision of emergency shelter and NFIs in district Bagh, Poonch, Haveli and Muzafarabad. 2 MHUs have also been deployed in District Haveli today. So far, 51 patients were treated in Hallan Shamil of Union Council Kala Mula, District Haveli. than 15,200 flood afected people all over Pakistan with services including food and non food items provision, 1.WEATHER OUTLOOK (as of 15th Sep,2014 at 1045 hrs by pak met) HYDROLOGICAL SITUATION: River Chenab at Punjnad is in High Flood Level. -

Favelas in the Media Report
Favelas in the Media: How the Global Narrative on Favelas Changed During Rio’s Mega-Event Years 1094 articles - eight global outlets - 2008-2016 Research conducted by Catalytic Communities in Rio de Janeiro December 2016 Lead Researcher: Cerianne Robertson, Catalytic Communities Research Coordinator Contents Research Contributors: Lara Mancinelli Alex Besser Nashwa Al-sharki Sophia Zaia Gabi Weldon Chris Peel Megan Griffin Raven Hayes Amy Rodenberger Natalie Southwick Claudia Sandell Juliana Ritter Aldair Arriola-Gomez Mikayla Ribeiro INTRODUCTION 5 Nicole Pena Ian Waldron Sam Salvesen Emilia Sens EXECUTIVE SUMMARY 9 Benito Aranda-Comer Wendy Muse Sinek Marcela Benavides (CatComm Board of Directors) METHODOLOGY 13 Gabriela Brand Theresa Williamson Clare Huggins (CatComm Executive Director) FINDINGS 19 Jody van Mastrigt Roseli Franco Ciara Long (CatComm Program Director) 01. Centrality ................................................................................................ 20 Rhona Mackay 02. Favela Specificity .................................................................................... 22 Translation: 03. Perspective ............................................................................................. 29 04. Language ................................................................................................ 33 Geovanna Giannini Leonardo Braga Nobre 05. Topics ..................................................................................................... 39 Kris Bruscatto Arianne Reis 06. Portrayal ................................................................................................ -

Guide to Islamabad
GUIDE TO ISLAMABAD Abstract We at the World Bank Group Family Network (WBGFN) Islamabad have put together this short guide to help you with all the basic needs. If you need any more help, feel free to contact the author or any of the other members listed in this guide. WBGFN Islamabad Pakistan Table of Contents WBGFN Islamabad Contacts ................................................................................................................... 2 Introduction ................................................................................................................................................... 3 Climate .................................................................................................................................................................. 4 Language .............................................................................................................................................................. 4 Time Zone ............................................................................................................................................................. 4 Currency ............................................................................................................................................................... 4 Living ............................................................................................................................................................... 5 Childcare and Household Staff ........................................................................................................................ -

List of Ngos
Registration Sr. Name of NGO Address Status(Reg No,& No Date & Relevant Law Malot Commercial Center, Shahpur VSWA/ICT/494 ,Date: 1. Aas Welfare Association Simly Dam Road, Islamabad. 051- 6/9/2006, VSWA 2232394, 03005167142 Ordinance 1961 VSWA/ICT/439, Village Khana Dak, Madina Town, Date:31/3/2004, 2. Abaseen Welfare Society Jabbah, Barma Chowk, Islamabad. VSWA Ordinance 03005308511 1961 Office No.5, 1st Floor, A & K Plaza, F- VSWA/ICT/511,Date 3. Acid Survivors Foundation. 10 Markaz, Islamabad. 051-2214052, 02/08/2007, VSWA 03008438984 Ordinance 1961 VSWA/ICT/282, Date Ali Pur Frash Lehtrar Road, 4. Akhmat Welfare Centre 24/04/1998, VSWA Islamabad. 051-2519062 Ordinance 1961 Al Mustafa Towers VSWA/ICT/438, Date # 204, Al Mustafa Towers F-10 5. Residents Associations 27/03/2004,VSWA Markaz, Islamabad. 03458555872 (AMPTRWA) Ordinance 1961 VSWA/ICT/520, Date Al-Firdous Welfare Mohallah Ara, Bharakau, Islamabad. 6. 2/04/2008, VSWA Association 051-2512308, 03008565227 Ordinance 1961 VSWA/ICT/261,Date:0 Model Village Ali Pur Farash 7. Al-Itehad Welfare Society 5/08/1996, VSWA Islamabad. Ordinance 1961 VSWA/ICT/202,Date:1 NearF.G.Boys High School Shahdra 8. Al-Jihad Youth Organization 7/06/1993,VSWA Islamabad Ordinance 1961 VSWA/ICT/377, Date H.No.39 Gali No.67 I- 9. Al-Noor Foundation. 17.4.2002, VSWA 10/1,Islamabad.051-4443227 Ordinance 1961 VSWA/ICT/90, Date 10. Al-Noor Islamic Center Rawal Town Islamabad 2.12.1990 VSWA Ordinance 1961 VSWA/ICT/89, Date 11. Al-Noor Islamic Center Sharifabad Tarlai Islamabad 2.12.1990 VSWA Ordinance 1961 VSWA/ICT/271, Date PEC Building, Ataturk Avenue, G-5/2, 12. -
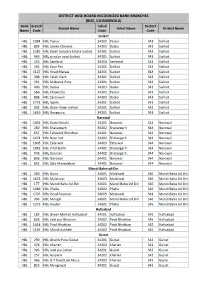
District Wise Board Recognized Bank Branches
DISTRICT WISE BOARD RECOGNIZED BANK BRANCHES (BISE, GUJRANWALA) Bank Branch Tehsil District Branch Name Tehsil Name District Name Name Code Code Code Sialkot HBL 1084 HBL Pasrur 34302 Pasrur 343 Sialkot HBL 895 HBL Jamke Cheema 34303 Daska 343 Sialkot HBL 1285 HBL Small Industry Estate Sialkot 34301 Sialkot 343 Sialkot HBL 969 HBL circular road Sialkot 34301 Sialkot 343 Sialkot HBL 425 HBL Sambrial 34304 Sambrial 343 Sialkot HBL 492 HBL Koor Pur 34301 Sialkot 343 Sialkot HBL 1127 HBL Head Marala 34301 Sialkot 343 Sialkot HBL 308 HBL Fateh Garh 34301 Sialkot 343 Sialkot HBL 291 HBL Mubarak Pura 34301 Sialkot 343 Sialkot HBL 406 HBL Daska 34303 Daska 343 Sialkot HBL 566 HBL Chawinda 34302 Pasrur 343 Sialkot HBL 808 HBL Saranwali 34303 Daska 343 Sialkot HBL 1773 HBL Ugoki 34301 Sialkot 343 Sialkot HBL 992 HBL Bazar Kalan Sialkot 34301 Sialkot 343 Sialkot HBL 1619 HBL Rungpura 34301 Sialkot 343 Sialkot Narowal HBL 1405 HBL Bado Malahi 34401 Narowal 344 Narowal HBL 260 HBL Shakargarh 34402 Shakargarh 344 Narowal HBL 637 HBL Talwandi Bhindran 34401 Narowal 344 Narowal HBL 1474 HBL Noor kot 34402 Shakargarh 344 Narowal HBL 1805 HBL Zafarwal 34403 Zafarwal 344 Narowal HBL 1842 HBL Pindi Bohri 34401 Shakargarh 344 Narowal HBL 978 HBL Darman 34402 Shakargarh 344 Narowal HBL 836 HBL Narowal 34401 Narowal 344 Narowal HBL 852 HBL Qila Ahmedabad 34401 Narowal 344 Narowal Mandi Baha-ud-Din HBL 560 HBL Gojra 34601 Malakwal 346 Mandi Baha Ud Din HBL 1623 HBL Malakwal 34603 Malakwal 346 Mandi Baha Ud Din HBL 177 HBL Mandi Baha Ud Din 34601 Mandi Baha Ud -
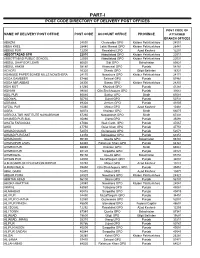
Part-I: Post Code Directory of Delivery Post Offices
PART-I POST CODE DIRECTORY OF DELIVERY POST OFFICES POST CODE OF NAME OF DELIVERY POST OFFICE POST CODE ACCOUNT OFFICE PROVINCE ATTACHED BRANCH OFFICES ABAZAI 24550 Charsadda GPO Khyber Pakhtunkhwa 24551 ABBA KHEL 28440 Lakki Marwat GPO Khyber Pakhtunkhwa 28441 ABBAS PUR 12200 Rawalakot GPO Azad Kashmir 12201 ABBOTTABAD GPO 22010 Abbottabad GPO Khyber Pakhtunkhwa 22011 ABBOTTABAD PUBLIC SCHOOL 22030 Abbottabad GPO Khyber Pakhtunkhwa 22031 ABDUL GHAFOOR LEHRI 80820 Sibi GPO Balochistan 80821 ABDUL HAKIM 58180 Khanewal GPO Punjab 58181 ACHORI 16320 Skardu GPO Gilgit Baltistan 16321 ADAMJEE PAPER BOARD MILLS NOWSHERA 24170 Nowshera GPO Khyber Pakhtunkhwa 24171 ADDA GAMBEER 57460 Sahiwal GPO Punjab 57461 ADDA MIR ABBAS 28300 Bannu GPO Khyber Pakhtunkhwa 28301 ADHI KOT 41260 Khushab GPO Punjab 41261 ADHIAN 39060 Qila Sheikhupura GPO Punjab 39061 ADIL PUR 65080 Sukkur GPO Sindh 65081 ADOWAL 50730 Gujrat GPO Punjab 50731 ADRANA 49304 Jhelum GPO Punjab 49305 AFZAL PUR 10360 Mirpur GPO Azad Kashmir 10361 AGRA 66074 Khairpur GPO Sindh 66075 AGRICULTUR INSTITUTE NAWABSHAH 67230 Nawabshah GPO Sindh 67231 AHAMED PUR SIAL 35090 Jhang GPO Punjab 35091 AHATA FAROOQIA 47066 Wah Cantt. GPO Punjab 47067 AHDI 47750 Gujar Khan GPO Punjab 47751 AHMAD NAGAR 52070 Gujranwala GPO Punjab 52071 AHMAD PUR EAST 63350 Bahawalpur GPO Punjab 63351 AHMADOON 96100 Quetta GPO Balochistan 96101 AHMADPUR LAMA 64380 Rahimyar Khan GPO Punjab 64381 AHMED PUR 66040 Khairpur GPO Sindh 66041 AHMED PUR 40120 Sargodha GPO Punjab 40121 AHMEDWAL 95150 Quetta GPO Balochistan 95151 -

Islamabad.Pdf
S.No. Brand Name Category OFFER OFFER DESCRIPTION City ADDRESS Valid till On Purchase of Rs.5,000, Get 1 Pair of Local Socks Free. | On Purchase of Rs.10,000, Get 1 Pair of Hush 1 Hush Puppies Apparel & Footwear Save Up to 10% | Save Up to 10% Islamabad Shop # 185, 1st Floor, Centaurus Mall. Islmabad 31-Dec-20 Puppies Socks & Kiwi Polish Free. On Purchase of Rs.5,000, Get 1 Pair of Local Socks Free. | On Purchase of Rs.10,000, Get 1 Pair of Hush 2 Hush Puppies Apparel & Footwear Save Up to 10% | Save Up to 10% Islamabad Shop #13-14, Asad Plaza, Sector G-9 Markaz. Islamabad 31-Dec-20 Puppies Socks & Kiwi Polish Free. On Purchase of Rs.5,000, Get 1 Pair of Local Socks Free. | On Purchase of Rs.10,000, Get 1 Pair of Hush 3 Hush Puppies Apparel & Footwear Save Up to 10% | Save Up to 10% Islamabad Shop No. 11, Block? 12 C, F-7 Markaz. Islamabad 31-Dec-20 Puppies Socks & Kiwi Polish Free. On Purchase of Rs.5,000, Get 1 Pair of Local Socks Free. | On Purchase of Rs.10,000, Get 1 Pair of Hush Shop # 9, Block D, Super Market, Sector F-6 Markaz. 4 Hush Puppies Apparel & Footwear Save Up to 10% | Save Up to 10% Islamabad 31-Dec-20 Puppies Socks & Kiwi Polish Free. Islamabad Shop # 6, Sama Plaza 68-W Jinnah Avenue Blue Area, 5 Sports One International Health & Fitness Flat 10% Off Except For Promotion Items Islamabad 31-Dec-20 Islamabad.