Aviation Physiology Education Advisory
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Chapter 23 ENVIRONMENTAL EXTREMES: ALTERNOBARIC
Environmental Extremes: Alternobaric Chapter 23 ENVIRONMENTAL EXTREMES: ALTERNOBARIC RICHARD A. SCHEURING, DO, MS*; WILLIAM RAINEY JOHNSON, MD†; GEOFFREY E. CIARLONE, PhD‡; DAVID KEYSER, PhD§; NAILI CHEN, DO, MPH, MASc¥; and FRANCIS G. O’CONNOR, MD, MPH¶ INTRODUCTION DEFINITIONS MILITARY HISTORY AND EPIDEMIOLOGY Altitude Aviation Undersea Operations MILITARY APPLIED PHYSIOLOGY Altitude Aviation Undersea Operations HUMAN PERFORMANCE OPTIMIZATION STRATEGIES FOR EXTREME ENVIRONMENTS Altitude Aviation Undersea Operations ONLINE RESOURCES FOR ALTERNOBARIC ENVIRONMENTS SUMMARY *Colonel, Medical Corps, US Army Reserve; Associate Professor, Military and Emergency Medicine, Uniformed Services University of the Health Sci- ences, Bethesda, Maryland †Lieutenant, Medical Corps, US Navy; Undersea Medical Officer, Undersea Medicine Department, Naval Medical Research Center, Silver Spring, Maryland ‡Lieutenant, Medical Service Corps, US Navy; Research Physiologist, Undersea Medicine Department, Naval Medical Research Center, Silver Spring, Maryland §Program Director, Traumatic Injury Research Program; Assistant Professor, Military and Emergency Medicine, Uniformed Services University of the Health Sciences, Bethesda, Maryland ¥Colonel, Medical Corps, US Air Force; Assistant Professor, Military and Emergency Medicine, Uniformed Services University of the Health Sciences, Bethesda, Maryland ¶Colonel (Retired), Medical Corps, US Army; Professor and former Department Chair, Military and Emergency Medicine, Uniformed Services University of the Health Sciences, -

Resident Scholarly Work
RESIDENT SCHOLARLY WORK Process Improvement 2020-2021 CPIP Curriculum Ongoing Projects: Alexander Gavralidis, Stephanie tin, Matthew Macey, Allisa Alport, Beenish Furquan, Justin Byrne • Unnecessary laboratory draws in patients at a Community Hospital - evaluating whether inpatients at Salem Hospital staying overnight for a social reason undergo unnecessary laboratory draws Daria Ade, Mayuri Rapolu, Usman Mughal, Eva Kubrova, Barbara Lambl, Patrick Lee • Procalcitonin utilization to tailor antibiotic use at Salem Hospital- part of Antibiotic Stewardship program Sneha Lakshman, Arturo Castro, Ashley So, George Kavalam, Hassan Kazmi, Daniela Urma, Patrick Gordan • Development of a standardized ultrasound guided central venus catheter insertion curriculum Nupur Dandawate, Farideh Davoudi , Usama Talib, Patrick Lee • Inpatient Echo utilization – guidelines updates Anneris Estevez, Usmam Mughal, Zach Abbott, Evita Joseph, Caroline Cubbison, Faith Omede, Daniela Urma • Decrease health disparities for Hispanic community at Lynn NSPG by standardizing diabetes education referral patterns and patient education Imama Ahmad, Usama Talib, Muhammad Akash, Pablo Ledesma, Patrick Lee • Inpatient Telemetry Utilization Usman Mughal, Anneris Estevez, Patrick Lee, Barbara Lambl • Health Disparities & Covid-19 Impact on Minorities, sponsored by Dr. Patrick Lee, Chair of Medicine, Dr. Barb Lambl, Infectious Disease 2017-2020 Alexander Gavralidis, Emre Tarhan, Anneris Estevez, Daniela Urma, Austin Turner, Patrick Lee • Expanded Access to Convalescent Plasma for the Treatment of Patients with COVID-19 – 5/2020 implementing use of Convalescent Plasma to MGB Salem hospital in collaboration with research team. Arturo Castro-Diaz, Dr. Daniela Urma • Improving Hospital Care and Post - acute Care of SARS CoV2 patients 4/2020- 8/2020 Caroline Cubbison, Sohaib Ansari, Adam Matos • Code Status Documentation for admitted patients at Salem Hospital - Project accepted to SHM national meeting to be presented in April 2020 Caroline Cubbison, Coleen Reid, Dr. -

Prioritization of Health Services
PRIORITIZATION OF HEALTH SERVICES A Report to the Governor and the 74th Oregon Legislative Assembly Oregon Health Services Commission Office for Oregon Health Policy and Research Department of Administrative Services 2007 TABLE OF CONTENTS List of Figures . iii Health Services Commission and Staff . .v Acknowledgments . .vii Executive Summary . ix CHAPTER ONE: A HISTORY OF HEALTH SERVICES PRIORITIZATION UNDER THE OREGON HEALTH PLAN Enabling Legislatiion . 3 Early Prioritization Efforts . 3 Gaining Waiver Approval . 5 Impact . 6 CHAPTER TWO: PRIORITIZATION OF HEALTH SERVICES FOR 2008-09 Charge to the Health Services Commission . .. 25 Biennial Review of the Prioritized List . 26 A New Prioritization Methodology . 26 Public Input . 36 Next Steps . 36 Interim Modifications to the Prioritized List . 37 Technical Changes . 38 Advancements in Medical Technology . .42 CHAPTER THREE: CLARIFICATIONS TO THE PRIORITIZED LIST OF HEALTH SERVICES Practice Guidelines . 47 Age-Related Macular Degeneration (AMD) . 47 Chronic Anal Fissure . 48 Comfort Care . 48 Complicated Hernias . 49 Diagnostic Services Not Appearing on the Prioritized List . 49 Non-Prenatal Genetic Testing . 49 Tuberculosis Blood Test . 51 Early Childhood Mental Health . 52 Adjustment Reactions In Early Childhood . 52 Attention Deficit and Hyperactivity Disorders in Early Childhood . 53 Disruptive Behavior Disorders In Early Childhood . 54 Mental Health Problems In Early Childhood Related To Neglect Or Abuse . 54 Mood Disorders in Early Childhood . 55 Erythropoietin . 55 Mastocytosis . 56 Obesity . 56 Bariatric Surgery . 56 Non-Surgical Management of Obesity . 58 PET Scans . 58 Prenatal Screening for Down Syndrome . 59 Prophylactic Breast Removal . 59 Psoriasis . 59 Reabilitative Therapies . 60 i TABLE OF CONTENTS (Cont’d) CHAPTER THREE: CLARIFICATIONS TO THE PRIORITIZED LIST OF HEALTH SERVICES (CONT’D) Practice Guidelines (Cont’d) Sinus Surgery . -

Thermoregulatory Correlates of Nausea in Rats and Musk Shrews
www.impactjournals.com/oncotarget/ Oncotarget, Vol. 5, No. 6 Thermoregulatory correlates of nausea in rats and musk shrews Sukonthar Ngampramuan1, Matteo Cerri2, Flavia Del Vecchio2, Joshua J. Corrigan3, Amornrat Kamphee1, Alexander S. Dragic3, John A. Rudd4, Andrej A. Romanovsky3, and Eugene Nalivaiko5 1 Research Center for Neuroscience and Institute of Molecular Bioscience, Mahidol University, Bangkok, Thailand; 2 Department of Biomedical and Motor Sciences, University of Bologna, Bologna, Italy; 3 FeverLab, Trauma Research, St. Joseph’s Hospital and Medical Center, Phoenix, AZ, USA; 4 School of Biomedical Sciences, Chinese University of Hong Kong, Hong Kong, China; 5 School of Biomedical Sciences and Pharmacy, University of Newcastle, Newcastle, NSW, Australia. Correspondence to: Eugene Nalivaiko, email: [email protected] Correspondence to: Andrej A. Romanovsky, email: [email protected] Keywords: nausea, chemotherapy, temperature, hypothermia. Received: December 21, 2013 Accepted: February 21, 2014 Published: February 22 2014 This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. ABSTRACT: Nausea is a prominent symptom and major cause of complaint for patients receiving anticancer chemo- or radiation therapy. The arsenal of anti-nausea drugs is limited, and their efficacy is questionable. Currently, the development of new compounds with anti-nausea activity is hampered by the lack of physiological correlates of nausea. Physiological correlates are needed because common laboratory rodents lack the vomiting reflex. Furthermore, nausea does not always lead to vomiting. Here, we report the results of studies conducted in four research centers to investigate whether nausea is associated with any specific thermoregulatory symptoms. -

Medical Aspects of Harsh Environments, Volume 2, Chapter
Medical Aspects of Harsh Environments, Volume 2 Chapter 32 PRESSURE CHANGES AND HYPOXIA IN AVIATION R. M. HARDING, BSC, MB BS, PHD* INTRODUCTION THE ATMOSPHERE Structure Composition THE PHYSIOLOGICAL CONSEQUENCES OF RAPID ASCENT TO ALTITUDE Hypoxia Hyperventilation Barotrauma: The Direct Effects of Pressure Change Altitude Decompression Sickness LIFE-SUPPORT SYSTEMS FOR FLIGHT AT HIGH ALTITUDE Cabin Pressurization Systems Loss of Cabin Pressurization Personal Oxygen Equipment SUMMARY *Principal Consultant, Biodynamic Research Corporation, 9901 IH-10 West, Suite 1000, San Antonio, Texas 78230; formerly, Royal Air Force Consultant in Aviation Medicine and Head of Aircrew Systems Division, Department of Aeromedicine and Neuroscience of the UK Centre for Human Science, Farnborough, Hampshire, United Kingdom 984 Pressure Changes and Hypoxia in Aviation INTRODUCTION The physiological consequences of rapid ascent and life-support engineers has established reliable to high altitude are a core problem in the field of techniques for safe flight at high altitudes, as demon- aerospace medicine. Those who live and work in strated by current atmospheric flight in all its forms, mountain terrain experience a limited range of al- military and civilian, from balloon flights to sail planes titudes and have time to adapt to the hypoxia ex- to supersonic aircraft and spacecraft. Although reli- perienced at high terrestrial elevations. In contrast, able cabin pressurization and oxygen delivery systems flyers may be exposed to abrupt changes in baro- have greatly reduced incidents and accidents due to metric pressure and to acute, life-threatening hy- hypoxia in flight, constant vigilance is required for poxia (see also Chapter 28, Introduction to Special their prevention. -

Bluemagazine Caribbeanexplor
38 SABA KITTS /ST. LUXURY LIVEABOARD Caribbean Explorer II The liveaboard experience is luxurious and focused on one thing—maximum diving pleasure. Hard-core divers who don’t mind interacting with a small group out at sea for a week, would love this excursion. By SOLOMON BAKSH Tent Reef is probably the most striking reef in Saba with vibrant sponges, enormous gorgonians and teeming with fish life 39 THE Boat at. Dive. Sleep…well, sleeping my shoes into. That was the last I saw of crew members on board: Tim Heaton, is optional. It’s a liveaboard them until seven days later. Captain, USA; Chris Johnson, Engineer, lifestyle—getting up from your I was the first guest to arrive on board USA; Nichol Schilling, Purser, Germany; Ebed every day for a week with a the boat and was given the best location to Instructors Claire Keany, Scotland; Brett view of a breathtaking sunrise from your set up my gear—right next to the exit. Lockhoff, USA; Joe Lamontage, Canada. window, the ocean always in sight, a hot The person responsible for keeping all of us breakfast and another day of great diving. Amenities well fed was chef, Sarah Dauphinee, USA. It’s the nature of these trips that make The Caribbean Explorer II was well laid Every day was an epicurean delight with them so attractive. Plying the open ocean out. The upper deck housed the galley, air- Sarah serving up Mexican, Mediterranean, to different dive sites every day and over conditioned dining area and sun deck. Italian, Caribbean and BBQ dishes. -

Carbon Monoxide Poisoning
Carbon Monoxide Department of Boating and Waterways www.BoatResponsibly.com Exposure to CO in large amounts or for a long duration results in death. Carbon monoxide (CO) is an odorless, colorless gas in the exhaust produced in gasoline engines. Boats release CO through the exhaust ports of vessels that are either idling or underway. When inhaled, CO replaces oxygen in tissues. What are the symptoms of carbon monoxide poisoning? Symptoms of CO poisoning may include nausea, dizziness, confusion, headache and fainting; however, people often mistakenly attribute these symptoms to too much alcohol, sun, and noise, or to motion sickness from the water or exhaustion. How are people exposed to carbon monoxide in a marine environment? Traditionally, CO poisonings have occurred on houseboats, vessels with overhead canopies or other vessels that have poor ventilation. CO also accumulates onboard a vessel through a process known as the ‘station wagon effect.’ This occurs as air moves around a boat and forms a low pressure area immediately behind the broad, flat transom. CO from the exhaust system enters the low-pressure area and is fed back into the cockpit and into the cabin. Many cases of carbon monoxide inhalation have involved a recreational activity known as ‘teak surfing’. ‘Teak surfing’ involves holding onto the swim platform or transom of an underway vessel to bodysurf on the wake of the vessel. As of January 1, 2005, ‘teak surfing’ and other similar recreational activities are against the law in California. How common is carbon monoxide poisoning in a marine environment? Nationwide, between 1990 and 2004, there were 571 reported boating-related CO poisonings, including 113 deaths; 43 in California alone. -

Discover Scuba
Discover Scuba Come explore the amazing underwater world in the Bradford Woods swimming pool with a maximum depth of 5 ft. Participation requirements: -Minimum age of 12 -PADI Liability release -RSTC Medical History form— To be completed prior to camp with personal physician and submitted during registration. Discover Scuba or Medical History Questions? Bob Kessler [email protected] Non-Agency Disclosure and Acknowledgment Agreement In European Union and European Free Trade Association countries use alternative form. Please read carefully and fill in all blanks before signing. I understand and agree that PADI Members (“Members”), including _______________________________store/resort and/or any individual PADI Instructors and Divemasters associated with the program in which I am participat- ing, are licensed to use various PADI Trademarks and to conduct PADI training, but are not agents, employees or franchisees of PADI Americas, Inc, or its parent, subsidiary and affiliated corporations (“PADI”). I further understand that Member business activities are independent, and are neither owned nor operated by PADI, and that while PADI establishes the standards for PADI diver train- ing programs, it is not responsible for, nor does it have the right to control, the operation of the Members’ business activities and the day-to day conduct of PADI programs and supervision of divers by the Members or their associated staff. I further understand and agree on behalf of myself, my heirs and my estate that in the event of an injury or death during this activity, neither I nor my es- tate shall seek to hold PADI liable for the actions, inactions or negligence of _________________________________________store/resort and/or the instructors and divemasters associated with the activity. -

Journal of the Aerospace Medical Association Index
Journal of the Aerospace Medical Association Index Clinical Problems in Aviation Medicine You’re the Flight Surgeon Cases from the Aerospace Medicine Residents' Teaching File Aeromedical Grand Rounds Topics in Aeromedical Certification Cases from CAMI Clinical articles with aeromedical disposition I have indexed the "Clinical Problems in Aviation Medicine" (CPAM), "You’re the Flight Surgeon" (YTFS), "Cases From The Aerospace Medicine Residents' Teaching File" (AMRTF), "Aeromedical Grand Rounds" (AGR), "Topics in Aeromedical Certification" (TAC), "Cases from CAMI" (FAA Civil Aerospace Medical Institute Aerospace Medical Certification Division) columns, and other articles discussing the aeromedical disposition of particular clinical conditions in the journal of the Aerospace Medical Association from its inception in 1930 through December 2016 by topic. The CPAM series published 14 article from September 1961 to November 1963 from Mayo Clinic. The first YTFS article was in January 1975 and continues to the present. YTFS articles before August 1990 are not indexed in PubMed; and prior to April 1989 no authors were listed. The AMRTF series published 80 numbered cases from October 1984 through 2004. Case number 5 I cannot find in PubMed or the AsMA index. The AGR series published 19 articles from November 1993 through December 1996. The TAC series published 21 articles from January 1998 to August 2001. The CAMI series published 19 articles from June 2006 through September 2008. In the clinical and review articles I not did not include retrospective reviews or prospective incidence studies of a population; mishap or inflight incapacitation review; specific medication review, unless it was in the context of a clinical condition; and non-aviation environments (including parachuting, diving) and passenger- and aeromedical evacuation- related conditions. -

Medical Release Form
MEDICAL STATEMENT Participant Record (Confidential Information) Please read carefully before signing. This is a statement in which you are informed of some potential risks disease, a current cold or congestion, epilepsy, a severe medical involved in scuba diving and of the conduct required of you during problem or who is under the influence of alcohol or drugs should not the Shark Dive program. Your signature on this statement is required dive. If you have asthma, heart disease, other chronic medical for you to participate in the Shark Dive program offered by conditions or you are taking medications on a regular basis, you should consult your doctor and the instructor before participating in __________________________from Hampton Dive Center and this program, and on a regular basis thereafter upon completion. You Instructor will also learn from the instructor the important safety rules regarding breathing and equalization while scuba diving. Improper use of scuba Atlantis Marine World LLC located in the city of Riverhead, equipment can result in serious injury. You must be thoroughly state/province of New York. instructed in its use under direct supervision of a qualified professional to use it safely. Read this statement prior to signing it. You must complete this Medical Statement, which includes the medical questionnaire section, Medical Statement and Guidelines for Recreational Scuba Diver’s to enroll in the Shark Dive program. If you are a minor, you must Physical Examination to take to your physician are attached to this have this Statement signed by a parent or guardian. form. Diving is an exciting and demanding activity. -
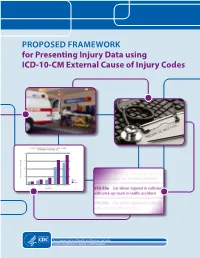
For Presenting Injury Data Using ICD-10-CM External Cause of Injury Codes
PROPOSED FRAMEWORK for Presenting Injury Data using ICD-10-CM External Cause of Injury Codes NONFATAL UNINTENTIONAL MOTOR VEHICLE-TRAFFIC OCCUPANT INJURY RATES, UNITED STATES, 2012 2000 1500 1000 500 RATE PER 100,000 POPULATION RATE MALE FEMALE 0 00–04 yrs 05–09 yrs 10–14 yrs 15–19 yrs 20–24 yrs AGE GROUP U.S. Department of Health and Human Services Centers for Disease Control and Prevention Proposed Framework for Presenting Injury Data using ICD-10-CM External Cause of Injury Codes Joseph L Annest, PhD, MS,1 Holly Hedegaard, MD, MSPH,2 Li-Hui Chen, PhD,2 Margaret Warner, PhD,2 Equater (Ann) Smalls1 March 2014 A Collaboration of CDC’s National Center for Injury Prevention and Control,1 Atlanta, GA and National Center for Health Statistics,2 Hyattsville, MD Proposed Framework for Presenting Injury Data using ICD-10-CM External Cause of Injury Codes is a publication of The National Center for Injury Prevention and Control and the National Center for Health Statistics within the Centers for Disease Control and Prevention. Centers for Disease Control and Prevention Thomas R. Frieden, MD, MPH, Director National Center for Injury Prevention and Control Daniel M. Sosin, MD, MPH, FACP, Acting Director National Center for Health Statistics Charles J. Rothwell, MBA, MS, Director Suggested citation: Annest, J., Hedegaard, H., Chen, L., Warner, M., and Small, E. (2014). Proposed Framework for Presenting Injury Data using ICD-10-CM External Cause of Injury Codes. Atlanta, GA: National Center for Injury Prevention and Control, National Center for Health Statistics, Centers for Disease Control and Prevention. -

What Is Motion Sickness?
What is Motion Sickness? SYMPTOMS Originally adapted with permission from a publication by the American Academy of Otolaryngology—Head and Neck Surgery, Alexandria, Virginia, with edits by Dr. Jeremy Hinton. CONFLICTING SIGNALS Motion sickness is the most common medical problem associated with travel. Symptoms appear when the central nervous system WHAT IS MOTION SICKNESS? receives conflicting messages from the visual system and Some people experience nausea and even vomiting when riding in an the vestibular system airplane, automobile, or amusement park ride. This is called motion in the inner ears. sickness. Motion sickness is often caused by multi-axial motion and acceleration, especially if the eyes are seeing one thing while the body experiences another. An example of this would be if a person was sitting in the back seat of a car looking out the side window while the car ARTICLE accelerates down a hill and turns a corner at the same time. The sensation is often temporary, but for many it continues for a prolonged period of time, resulting in extreme discomfort and anxiety. Early symptoms of motion sickness may include nausea, increased salivation, belching, feeling clammy (diapohoretic), hyperventilating, and 091 a feeling of general unease. Because hyperventilation and progressive nausea are so unsettling, many people will report a feeling of impending doom that can lead to serious complications such as difficulty breathing, blood pressure drops (especially orthostatic hypotension), and even DID THIS ARTICLE passing out (syncope). Motion HELP YOU? sickness itself will not cause these SUPPORT VEDA @ symptoms, but can lead to a person feeling overwhelmed. VESTIBULAR.ORG Many people experience motion sickness when riding on a boat or ship.