Health & Diving Reference Series
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Urinary Problems in Decompression Sickness*
Paraplegia 23 (1985) 20-25 © 1985 International Medical Society of Paraplegia Urinary Problems in Decompression Sickness* Athanasios Dounis, M.D. and Dionisios Mitropoulos, M.D. The Naval Medical Hyperbaric Center) Piraeus Naval Hospital and Department of Urology) Athens Naval Hospital) Greece Summary The records of 25 patients with type II decompression sickness and urinary problems have been reviewed. Seventeen patients were professionals and 8 were above the age of 40. The disease appeared within the 1st hour of emergence from the water in 70% of the cases and within the first 4 hours in the remaining 30%. Nine patients were diagnosed as paraplegic and two as tetraplegic. All patients had urinary disturbances and 14 were on Foley-catheter drainage during the decompression while 11 were on intermittent catheterisation. Fifteen patients had improved urinary function after recompression) 8 had some difficulty) 2 underwent a sphincterotomy and one a transurethral prostatectomy. The low percentage of complete recovery was due to the delayed arrival at the decompression chamber. Key words: Diving; Decompression sickness; Urinary disturbances. Introduction Diving for sponge fishery is the main professional occupation of the young men in the South-East Aegean islands. Although the use of recompression has decreased the number of decompression sickness victims, patients with remaining neurological problems still present. During the last 20 years, although there is a decrease of the professional divers' accidents there is an increase of the number of patients with decompression sickness. This is due to the continuously increasing numbers of sport divers in Greece. In Greece, the field of underwater medicine is covered mainly by the Naval Medical Service. -

Course Description
Instructor: Walter W Lancaster II Off Campus phone: 951-351-1445 x204 Dept phone: NA Cell phone: 951-312-2589 Department of Health and Exercise Science e-mail: [email protected] Spring Quarter, 2016 Alternate e-mail: [email protected] Off Campus Office: La Sierra Academy Office Hours: M-Th 8am – 4pm Consultations by appointment PEAC 106 Scuba Diving Walter Lancaster Location: Health and Exercise Science Classroom 1 (or other assigned instructional locaton) & Pool Tuesdays 6:30pm ~ 9:45pm I. COURSE DESCRIPTION: A. Bulletin Course Description: Course Description Basic SCUBA Diver is an entry-level course for people who have not been previously certified to SCUBA dive, and provides a comprehensive overview of basic concepts that are required to dive safely. Topics include diving equipment, diving physiology, dive planing, environmental considerations, and recognizing and managing risks associated with Open Water diving. Participants who successfully complete the classroom and pool work will qualify for an Open Water certification experience, which must be completed if the student wishes to become a certified diver. Successful completion of the Open Water experience will result in an industry recognized and accepted certification at the level of Basic SCUBA Diver through the National Assocaiton of Underwater Instructors (NAUI). All attendees must be age 16 or older. Students must be able to demonstrate a 10-minute swim/float in water too deep to stand in without the use of swim aids, complete a 200 meter/yard continuous surface swim and demonstrate an underwater (single breath) free dive for a horizontal minimum distance of 25 yards. B. Instructional Materials: Use of the recommended text and Comprehesive Resource Notebook is made available to all students as part of the comprehensive Lab Fee. -
Hyperbaric Oxygen Therapy in Dermatology
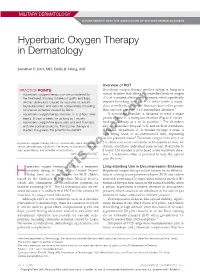
MILITARY DERMATOLOGY IN PARTNERSHIP WITH THE ASSOCIATION OF MILITARY DERMATOLOGISTS Hyperbaric Oxygen Therapy in Dermatology Jonathan P. Jeter, MD; Emily B. Wong, MD Overview of HOT PRACTICE POINTS Hyperbaric oxygen therapy involves sitting or lying in a • Hyperbaric oxygen therapy can be considered for special chamber that allows for controlled levels of oxygen the treatment of failing cutaneous grafts and flaps, (O2) at increased atmospheric pressure, which specifically chronic ulcerations caused by vasculitis or autoim- involves breathing near 100% O2 while inside a mono- mune disorders, and vascular compromise, including place or multiplace chamber5 that is pressurized to greater cutaneous ischemia caused by fillers. than sea level pressure (≥1.4 atmosphere absolute).2 • Hyperbaric oxygen therapy involves 1- to 2-hour treat- A monoplace chamber is designed to treat a single ments, 5 days a week, for as long as 1 month. person (Figure 1);copy a multiplace chamber (Figure 2) accom- 5,6 • Hyperbaric oxygen therapy is safe and well-tolerated, modates as many as 5 to 25 patients. The chambers with few contraindications. The sooner therapy is also accommodate hospital beds and medical attendants, started, the greater the potential for benefit. if needed. Hyperbaric O2 is inhaled through a mask, a tight-fitting hood, or an endotracheal tube, depending on notthe patient’s status.7 Treatment ranges from only 1 or Hyperbaric oxygen therapy (HOT) is a potentially useful technique for 2 iterations for acute conditions to 30 sessions or more for certain dermatologic conditions. We review its indications, dermato- chronic conditions. Individual sessions last 45 minutes to logic applications, and potential complications. -

Mansfield, NG18 2AD to the Editor: Dear Sir, VERTIGO in DIVERS Thank You for Asking for My Comments on Noel Roydhouse's Letter Which I Have Read with Interest
Br J Sports Med: first published as 10.1136/bjsm.17.3.210 on 1 September 1983. Downloaded from 210 CORRESPONDENCE 14 Woodhouse Road, Mansfield, NG18 2AD To the Editor: Dear Sir, VERTIGO IN DIVERS Thank you for asking for my comments on Noel Roydhouse's letter which I have read with interest. He is technically correct in stating that vertigo is not inevitable when the tympanic membrane ruptures. Vertigo is not dependent on the size of perforation that is sustained, but is dependent on the rate of ingress of cold water into the tympanic cavity. The caloric effect produced by rapid ingress of water is entirely dependent on the temperature difference between the water that has entered the tympanic cavity and body temperature. Once the water temperature reaches approximate body temperature then the caloric effect ceases as does the vertigo. As ENT surgeons we use this caloric phenomenon for testing labyrinthine function (vestibular function); and under test conditions we use water at 300C and 440C, in ears with intact tympanic membranes, in order to induce a vertigo. If an article were to be directed at "diving doctors" I think that it would be fair comment for it to be stated that a vertigo sustained on descent should be assumed to be due to a tympanic membrane rupture with rapid ingress of water, until proven otherwise, by inspection of the ear; if the tympanic membrane is found to be intact, then a diagnosis of perilymph fistula must be made, which will only be proved or disproved by performing an exploratory tympanotomy. -
22575VIC Course in Basic Oxygen Administration for First Aid
22575VIC Course in Basic Oxygen Administration for First Aid This course has been accredited under Part 4.4 of the Education and Training Reform Act 2006 Version 1 Accredited for the period: 1 January 2021 to 31 December 2025 © State of Victoria (Department of Education and Training) 2021. Copyright of this material is reserved to the Crown in the right of the State of Victoria. This work is licensed under a Creative Commons Attribution-NoDerivs 3.0 Australia licence (see Creative Commons for more information). You are free use, copy and distribute to anyone in its original form as long as you attribute Department of Education and Training as the author, and you license any derivative work you make available under the same licence. Disclaimer In compiling the information contained in and accessed through this resource, the Department of Education and Training (DET) has used its best endeavours to ensure that the information is correct and current at the time of publication but takes no responsibility for any error, omission or defect therein. To the extent permitted by law, DET, its employees, agents and consultants exclude all liability for any loss or damage (including indirect, special or consequential loss or damage) arising from the use of, or reliance on the information contained herein, whether caused or not by any negligent act or omission. If any law prohibits the exclusion of such liability, DET limits its liability to the extent permitted by law, for the resupply of the information. Third party sites This resource may contain links to third party websites and resources. -

Hyperbaric Physiology the Rouse Story Arrival at Recompression
Hyperbaric Physiology The Rouse Story • Oct 12, 1992, off the New Jersey coast • father/son team of experienced divers • explore submarine wreck in 230 ft (70 m) • breathing compressed air • trapped in wreck & escaped with no time for decompression Chris and Chrissy Rouse Arrival at recompression Recompression efforts facility • Both divers directly ascend to dive boat • Recompression starts about 3 hrs after • Helicopter arrives at boat in 1 hr 27 min ascent • Bronx Municipal Hospital recompression facility – put on pure O2 and compressed to 60 ft – Chris (39 yrs) pronounced dead • extreme pain as circulation returned – compressed to 165 ft, then over 5.5 hrs – Chrissy (22 yrs) gradually ascended back to 30 ft., lost • coherent and talking consciousness • paralysis from chest down • no pain – back to 60 ft. Heart failure and death • blood sample contained foam • autopsy revealed that the heart contained only foam Medical Debriefing Gas Laws • Boyle’s Law • Doctors conclusions regarding their – P1V1 = P2V2 treatment • Dalton’s Law – nothing short of recompression to extreme – total pressure is the sum of the partial pressures depths - 300 to 400 ft • Henry’s Law – saturation treatment lasting several days – the amt of gas dissolved in liquid at any temp is – complete blood transfusion proportional to it’s partial pressure and solubility – deep helium recompression 1 Scuba tank ~ 64 cf of air Gas problems during diving Henry, 1 ATM=33 ft gas (10 m) dissovled = gas Pp & tissue • Rapture of the deep (Nitrogen narcosis) solubility • Oxygen -

Heat Stroke Heat Exhaustion
Environmental Injuries Co lin G. Ka ide, MD , FACEP, FAAEM, UHM Associate Professor of Emergency Medicine Board-Certified Specialist in Hyperbaric Medicine Specialist in Wound Care The Ohio State University Wexner Medical Center The Most Dangerous Drug Combination… Accidental Testosterone Hypothermia and Alcohol! The most likely victims… Photo: Ralf Roletschek 1 Definition of Blizzard Hypothermia of Subnormal T° when the body is unable to generate sufficient heat to sustain normal functions Core Temperature < 95°F 1979 (35°C) Most Important Temperatures Thermoregulation 95°F (35° C) Hyper/Goofy The body uses a Poikilothermic shell to maintain a Homeothermic core 90°F (32°C) Shivering Stops Maintains core T° w/in 1.8°F(1°C) 80°F (26. 5°C) Vfib, Coma Hypothalamus Skin 65°F (18°C) Asystole Constant T° 96.896.8-- 100.4° F 2 Thermoregulation The 2 most important factors Only 3 Causes! Shivering (10x increase) Decreased Heat Production Initiated by low skin temperature Increased Heat Loss Warming the skin can abolish Impaired Thermoregulation shivering! Peripheral vasoconstriction Sequesters heat Predisposing Predisposing Factors Factors Decreased Production Increased Loss –Endocrine problems Radiation Evaporation • Thyroid Conduction* • Adrenal Axis Convection** –Malnutrition *Depends on conducting material **Depends on wind velocity –Neuromuscular disease 3 Predisposing Systemic Responses CNS Factors T°< 90°F (34°C) Impaired Regulation Hyperactivity, excitability, recklessness CNS injury T°< 80°F (27°C) Hypothalamic injuries Loss of voluntary -

Analysis of Accidents and Sickness of Divers and Scuba Divers at the Training Centre for Divesr and Scuba Divers of the Polish Army
POLISH HYPERBARIC RESEARCH 2(71)2020 Journal of Polish Hyperbaric Medicine and Technology Society ANALYSIS OF ACCIDENTS AND SICKNESS OF DIVERS AND SCUBA DIVERS AT THE TRAINING CENTRE FOR DIVESR AND SCUBA DIVERS OF THE POLISH ARMY Władysław Wolański Polish Army Diver and Diver Training Centre, Naval Psychological Laboratory, Gdynia, Poland ARTICLE INFO PolHypRes 2020 Vol. 71 Issue 2 pp. 75 – 78 ISSN: 1734-7009 eISSN: 2084-0535 DOI: 10.2478/phr-2020-0013 Pages: 14, figures: 0, tables: 0 page www of the periodical: www.phr.net.pl Publisher Polish Hyperbaric Medicine and Technology Society 2020 Vol. 71 Issue 2 INTRODUCTION The first group of diseases occurs as a result of mechanical action directly on the body of the diver. Among The prerequisite for the prevention of diving- them are: ear and paranasal sinus barotrauma, pulmonary related sicknesses and accidents is strict compliance with barotrauma, crushing. both technical and medical regulations during diving In the second group we most often encounter the training and work [3,4]. consequences of the toxic effects of gaseous components of A very important issue is good knowledge of the air on the human body. This group includes decompression work of a diver and the anticipation of possible dangers by sickness, oxygen poisoning, nitrogen poisoning, CO2 the personnel participating in the dive [1]. The Military poisoning, carbon monoxide (CO) poisoning. Maritime Medical Committee (WKML) determines When analysing the causes of diving sicknesses whether or not an individual is healthy enough to dive, and accidents at the Diver and Scuba Diver Training Centre granting those who meet the required standards a medical of the Polish Army, certain groups of additional factors certificate that is valid for one year [1,2]. -

Vocabulario De Morfoloxía, Anatomía E Citoloxía Veterinaria
Vocabulario de Morfoloxía, anatomía e citoloxía veterinaria (galego-español-inglés) Servizo de Normalización Lingüística Universidade de Santiago de Compostela COLECCIÓN VOCABULARIOS TEMÁTICOS N.º 4 SERVIZO DE NORMALIZACIÓN LINGÜÍSTICA Vocabulario de Morfoloxía, anatomía e citoloxía veterinaria (galego-español-inglés) 2008 UNIVERSIDADE DE SANTIAGO DE COMPOSTELA VOCABULARIO de morfoloxía, anatomía e citoloxía veterinaria : (galego-español- inglés) / coordinador Xusto A. Rodríguez Río, Servizo de Normalización Lingüística ; autores Matilde Lombardero Fernández ... [et al.]. – Santiago de Compostela : Universidade de Santiago de Compostela, Servizo de Publicacións e Intercambio Científico, 2008. – 369 p. ; 21 cm. – (Vocabularios temáticos ; 4). - D.L. C 2458-2008. – ISBN 978-84-9887-018-3 1.Medicina �������������������������������������������������������������������������veterinaria-Diccionarios�������������������������������������������������. 2.Galego (Lingua)-Glosarios, vocabularios, etc. políglotas. I.Lombardero Fernández, Matilde. II.Rodríguez Rio, Xusto A. coord. III. Universidade de Santiago de Compostela. Servizo de Normalización Lingüística, coord. IV.Universidade de Santiago de Compostela. Servizo de Publicacións e Intercambio Científico, ed. V.Serie. 591.4(038)=699=60=20 Coordinador Xusto A. Rodríguez Río (Área de Terminoloxía. Servizo de Normalización Lingüística. Universidade de Santiago de Compostela) Autoras/res Matilde Lombardero Fernández (doutora en Veterinaria e profesora do Departamento de Anatomía e Produción Animal. -

Dysbarism - Barotrauma
DYSBARISM - BAROTRAUMA Introduction Dysbarism is the term given to medical complications of exposure to gases at higher than normal atmospheric pressure. It includes barotrauma, decompression illness and nitrogen narcosis. Barotrauma occurs as a consequence of excessive expansion or contraction of gas within enclosed body cavities. Barotrauma principally affects the: 1. Lungs (most importantly): Lung barotrauma may result in: ● Gas embolism ● Pneumomediastinum ● Pneumothorax. 2. Eyes 3. Middle / Inner ear 4. Sinuses 5. Teeth / mandible 6. GIT (rarely) Any illness that develops during or post div.ing must be considered to be diving- related until proven otherwise. Any patient with neurological symptoms in particular needs urgent referral to a specialist in hyperbaric medicine. See also separate document on Dysbarism - Decompression Illness (in Environmental folder). Terminology The term dysbarism encompasses: ● Decompression illness And ● Barotrauma And ● Nitrogen narcosis Decompression illness (DCI) includes: 1. Decompression sickness (DCS) (or in lay terms, the “bends”): ● Type I DCS: ♥ Involves the joints or skin only ● Type II DCS: ♥ Involves all other pain, neurological injury, vestibular and pulmonary symptoms. 2. Arterial gas embolism (AGE): ● Due to pulmonary barotrauma releasing air into the circulation. Epidemiology Diving is generally a safe undertaking. Serious decompression incidents occur approximately only in 1 in 10,000 dives. However, because of high participation rates, there are about 200 - 300 cases of significant decompression illness requiring treatment in Australia each year. It is estimated that 10 times this number of divers experience less severe illness after diving. Physics Boyle’s Law: The air pressure at sea level is 1 atmosphere absolute (ATA). Alternative units used for 1 ATA include: ● 101.3 kPa (SI units) ● 1.013 Bar ● 10 meters of sea water (MSW) ● 760 mm of mercury (mm Hg) ● 14.7 pounds per square inch (PSI) For every 10 meters a diver descends in seawater, the pressure increases by 1 ATA. -

Chapter 23 ENVIRONMENTAL EXTREMES: ALTERNOBARIC
Environmental Extremes: Alternobaric Chapter 23 ENVIRONMENTAL EXTREMES: ALTERNOBARIC RICHARD A. SCHEURING, DO, MS*; WILLIAM RAINEY JOHNSON, MD†; GEOFFREY E. CIARLONE, PhD‡; DAVID KEYSER, PhD§; NAILI CHEN, DO, MPH, MASc¥; and FRANCIS G. O’CONNOR, MD, MPH¶ INTRODUCTION DEFINITIONS MILITARY HISTORY AND EPIDEMIOLOGY Altitude Aviation Undersea Operations MILITARY APPLIED PHYSIOLOGY Altitude Aviation Undersea Operations HUMAN PERFORMANCE OPTIMIZATION STRATEGIES FOR EXTREME ENVIRONMENTS Altitude Aviation Undersea Operations ONLINE RESOURCES FOR ALTERNOBARIC ENVIRONMENTS SUMMARY *Colonel, Medical Corps, US Army Reserve; Associate Professor, Military and Emergency Medicine, Uniformed Services University of the Health Sci- ences, Bethesda, Maryland †Lieutenant, Medical Corps, US Navy; Undersea Medical Officer, Undersea Medicine Department, Naval Medical Research Center, Silver Spring, Maryland ‡Lieutenant, Medical Service Corps, US Navy; Research Physiologist, Undersea Medicine Department, Naval Medical Research Center, Silver Spring, Maryland §Program Director, Traumatic Injury Research Program; Assistant Professor, Military and Emergency Medicine, Uniformed Services University of the Health Sciences, Bethesda, Maryland ¥Colonel, Medical Corps, US Air Force; Assistant Professor, Military and Emergency Medicine, Uniformed Services University of the Health Sciences, Bethesda, Maryland ¶Colonel (Retired), Medical Corps, US Army; Professor and former Department Chair, Military and Emergency Medicine, Uniformed Services University of the Health Sciences, -

Risk Management Plan Snorkeling
OUTER LIMITS ADVENTURE FITNESS RISK MANAGEMENT PLAN RISK MANAGEMENT PLAN SNORKELING Outer Limits Adventure Fitness Sam Stedman 85 Chandler Street, Garbutt 4814 Mobile: 0421 484 211 1 OUTER LIMITS ADVENTURE FITNESS RISK MANAGEMENT PLAN Table of Contents Activity Description 3 Minimum Supervision and Qualifications 3 Minimum activity-specific Equipment/Facilities 4 Standard Operating Procedures 5 Risk Assessment 8 Safety and Emergency Procedures 13 Incident Register 15 Approval 16 2 OUTER LIMITS ADVENTURE FITNESS RISK MANAGEMENT PLAN ACTIVITY DESCRIPTION Details Title: Date: Activity: SNORKELING Details: Number of participants: Age Group: Experience level: Duration of activity: Program Sam Stedman; Outer Limits Adventure Fitness Manager: Activity Leader(s): Client: Snorkeling Snorkeling is a great activity to introduce participants to exploring the beach and ocean. Snorkeling is conducted at sheltered (not open to normal wave/tide/weather action) beach locations. The activity is designed as an entry level with participants learning how to use a snorkel and mask, swimming on the surface of the water (positive buoyancy) to explore ocean environments. This activity may be modified to a land based beach exploration program if conditions are not safe to enter the water. MINIMUM SUPERVISION AND QUALIFICATIONS • 1 instructor and two assistants for up to 20 children • Sufficient leaders with minimum qualifications supervising activity: 1 o Minimum Qualification: Certificate 3 in Outdoor Recreation or nationally recognised qualification as snorkeling/diving guide, or relevant experience in facilitating adventure based learning activities, Bronze Medallion r other relevant water rescue qualification • Sufficient leaders with current First Aid and CPR: 1 MINIMUM ACTIVITY-SPECIFIC EQUIPMENT/FACILITIES • First Aid Kit suitable for activity • Sun Safe equipment: hats, sunscreen, shade structure etc.