On-Pump Vascular Reperfusion of Thiel Embalmed Cadavers
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Minimally Invasive Superficial Femoral Artery Endarterectomy: Early Experience with a Modified Technique
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector Eur J Vasc Endovasc Surg 16, 254-258 (1998) ENDOVASCULAR AND SURGICAL TECHNIQUES Minimally Invasive Superficial Femoral Artery Endarterectomy: Early Experience with a Modified Technique M. S. Whiteley 1, T. R. Magee 1, E. P. H. Torrie 2 and R. B. Galland* Department of ~Surgery and 2Radiology, Royal Berkshire Hospital, London Road, Reading, U.K. Objectives: To describe our experience of a modified technique for carrying out remote endarterectomy for superficial femoral artery occlusive disease. Methods: A 4-French arterial dilator is inserted using a Smart needle into the popliteal artery below the occlusion. A remote endarterectomy is carried out through an arteriotomy in the proximal superficial femoral artery. The atheroma is cut distal to the lower extent of disease using a Moll ring cutter. The lower flap of atheroma is secured with an intraluminaI stent inserted from the arteriotomy in the superficial femoral artery. The arteriotomy is extended into the common femoral artery and closed with a vein patch. Results: The procedure was completed in 21 of 26 limbs. In 18 cases the superficial femoral artery remained patent at 30 days. Of the 21 cases all but four stayed in hospital for one night. A successful femoropopliteal bypass was carried out in the five patients in whom the procedure was not completed. Conclusion: Insertion of the dilator into the popliteal artery distal to the occlusion before carrying out the remote endarterectomy has two advantages. Firstly, the stent insertion is carried out in the correct plane and prevents dissection of the distal cut atheroma when attempting to pass the guidewire from above. -

Targeting Endothelial Kruppel-Like Factor 2 (KLF2) in Arteriovenous
Targeting Endothelial Krüppel-like Factor 2 (KLF2) in Arteriovenous Fistula Maturation Failure A dissertation submitted to the Graduate School of the University of Cincinnati in partial fulfillment of the requirements for the degree of DOCTOR OF PHILOSOPHY (Ph.D.) in the Biomedical Engineering Program Department of Biomedical Engineering College of Engineering and Applied Science 2018 by Keith Louis Saum B.S., Wright State University, 2012 Dissertation Committee: Albert Phillip Owens III, Ph.D. (Committee Chair) Begona Campos-Naciff, Ph.D Christy Holland, Ph.D. Daria Narmoneva, Ph.D. Prabir Roy-Chaudhury, M.D., Ph.D Charuhas Thakar, M.D. Abstract The arteriovenous fistula (AVF) is the preferred form of vascular access for hemodialysis. However, 25-60% of AVFs fail to mature to a state suitable for clinical use, resulting in significant morbidity, mortality, and cost for end-stage renal disease (ESRD) patients. AVF maturation failure is recognized to result from changes in local hemodynamics following fistula creation which lead to venous stenosis and thrombosis. In particular, abnormal wall shear stress (WSS) is thought to be a key stimulus which alters endothelial function and promotes AVF failure. In recent years, the transcription factor Krüppel-like factor-2 (KLF2) has emerged as a key regulator of endothelial function, and reduced KLF2 expression has been shown to correlate with disturbed WSS and AVF failure. Given KLF2’s importance in regulating endothelial function, the objective of this dissertation was to investigate how KLF2 expression is regulated by the hemodynamic and uremic stimuli within AVFs and determine if loss of endothelial KLF2 is responsible for impaired endothelial function. -

ICD~10~PCS Complete Code Set Procedural Coding System Sample
ICD~10~PCS Complete Code Set Procedural Coding System Sample Table.of.Contents Preface....................................................................................00 Mouth and Throat ............................................................................. 00 Introducton...........................................................................00 Gastrointestinal System .................................................................. 00 Hepatobiliary System and Pancreas ........................................... 00 What is ICD-10-PCS? ........................................................................ 00 Endocrine System ............................................................................. 00 ICD-10-PCS Code Structure ........................................................... 00 Skin and Breast .................................................................................. 00 ICD-10-PCS Design ........................................................................... 00 Subcutaneous Tissue and Fascia ................................................. 00 ICD-10-PCS Additional Characteristics ...................................... 00 Muscles ................................................................................................. 00 ICD-10-PCS Applications ................................................................ 00 Tendons ................................................................................................ 00 Understandng.Root.Operatons..........................................00 -
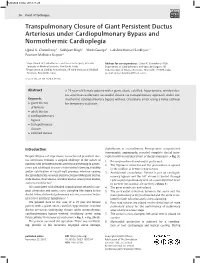
Transpulmonary Closure of Giant Persistent Ductus Arteriosus Under Cardiopulmonary Bypass and Normothermic Cardioplegia
Published online: 2019-11-25 THIEME 36 TranspulmonaryPoint of Technique Closure of Giant Persistent Ductus Arteriosus Chowdhury et al. Transpulmonary Closure of Giant Persistent Ductus Arteriosus under Cardiopulmonary Bypass and Normothermic Cardioplegia Ujjwal K. Chowdhury1 Sukhjeet Singh1 Niwin George1 Lakshmi Kumari Sankhyan1 Poonam Malhotra Kapoor2 1Department of Cardiothoracic and Vascular Surgery, All India Address for correspondence Ujjwal K. Chowdhury, MCh, Institute of Medical Sciences, New Delhi, India Department of Cardiothoracic and Vascular Surgery, All 2Department of Cardiac Anaesthesia, All India Institute of Medical India Institute of Medical Sciences, New Delhi 110029, India Sciences, New Delhi, India (e-mail: [email protected]). J Card Crit Care TSS 2020;3:36–38 Abstract A 25-year-old female patient with a giant, short, calcified, hypertensive, window duc- tus arteriosus underwent successful closure via transpulmonary approach under nor- Keywords mothermic cardiopulmonary bypass without circulatory arrest using a Foley catheter ► giant ductus for temporary occlusion. arteriosus ► adult ductus ► cardiopulmonary bypass ► transpulmonary closure ► calcified ductus Introduction chylothorax, or recanalization. Postoperative computerized tomographic angiography revealed complete ductal inter‑ Despite 80 years of experience, correction of persistent duc‑ ruption with no residual shunt or ductal aneurysm (►Fig. 3). tus arteriosus remains a surgical challenge in the subset of 1. Primary median sternotomy is performed. patients -

Curriculum Vitae
Curriculum Vitae INFORMAZIONI PERSONALI Nome SERGIO Cognome SALERNO Recapiti Sezione di Radiologia DIBIMEF E-mail [email protected] FORMAZIONE TITOLI • Studente in Medicina dal novembre 1986 al novembre 1992. • Specializzando in Radiodiagnostica dal Novembre 1992 al Dicembre 1996. • Esperienza come Assistente in Formazione presso l'Istituto di Radiologia della Università degli studi di Trieste diretto dal Prof. L. Dalla Palma (maggio 1994 e febbraio 1995). • Fellow al Diagnostic Radiology Department del Hammersmith Hospital di Londra (marzo-luglio 1996). • Dottorando di Ricerca in Radiologia Oncologica (ciclo XII) dal novembre 1997 al febbraio 2000. • Fellow al Diagnostic Radiology Department del St' Georges Hospital di Londra (aprile-luglio 1997). • Research Fellow del CIRSE al Diagnostic Radiology Department del St' Georges Hospital di Londra (luglio-ottobre 1999). ATTIVITA' DIDATTICA • Componente del Collegio dei Docenti del Dottorato di Ricerca in Scienze Stomatologiche dal Ciclo XVIII. • Docente nel Corso integrato di Diagnostica per Immagini del Corso di Laurea in Medicina e Chirurgia dell’Università di Palermo dall’anno accademico 2001-2002 al 2007-2008. • Docente del Corso di Laurea in Fisioterapia per la materia Diagnostica per Immagini dell’Università di Palermo dall’anno accademico 2002-2003 al 2007-2008. • Docente del Corso di Laurea in Tecniche della Riabilitazione Neuropsicomotoria per la materia Diagnostica per Immagini dell’Università di Palermo dall’anno accademico 2003-2004 al 2007-2008. • Docente del Corso di Laurea in Tecniche della Riabilitazione Neuropsicomotoria per la materia Neuroradiologia nell’ anno accademico nel 2008-2009. • Docente del Corso di Laurea in Tecniche della Riabilitazione Psichiatrica per la materia Diagnostica per Immagini dell’Università di Palermo dall’anno accademico 2004-2005 al 2006-2007. -

Multiple Yellow Plaques Assessed by Angioscopy with Quantitative Colorimetry in Patients with Myocardial Infarction
Circ J 2008; 72: 399–403 Multiple Yellow Plaques Assessed by Angioscopy With Quantitative Colorimetry in Patients With Myocardial Infarction Shigenobu Inami, MD*; Fumiyuki Ishibashi, MD*,**; Sergio Waxman, MD**; Kentaro Okamatsu, MD*; Koji Seimiya, MD*; Masamichi Takano, MD*; Ryota Uemura, MD*; Junko Sano, MD*; Kyoichi Mizuno, MD* Background Multiple angioscopic yellow plaques are associated with diffuse atherosclerotic plaque, and may be prevalent in patients with myocardial infarction (MI), so in the present study the yellow plaques in the coronary arteries of patients with MI was evaluated using quantitative colorimetry, and compared with those of patients with stable angina (SA). Methods and Results In the recorded angioscopic images of 3 coronary vessels in 29 patients (15 patients with MI, 14 with SA), yellow plaques were determined as visually yellow regions with b* value >0 (yellow color intensity) measured by the quantitative colorimetric method. A total of 90 yellow plaques were identified (b*=19.35±8.3, 3.05–45.35). Yellow plaques were significantly more prevalent in 14 (93%) of 15 culprit lesions of MI as compared with 8 (57%) of 14 of SA (p=0.03). In non-culprit segments, yellow plaques were similarly prevalent in 13 (87%) patients with MI and 11 (79%) with SA (p=0.65). Overall, multiple (≥2) yellow plaques were prevalent in 13 (87%) patients with MI, similar to the 10 (71%) with SA (p=0.38). The number of yellow plaques was significantly higher in patients with MI (3.8±1.9) than in those with SA (2.4±1.6, p=0.03). -

Icd-9-Cm (2010)
ICD-9-CM (2010) PROCEDURE CODE LONG DESCRIPTION SHORT DESCRIPTION 0001 Therapeutic ultrasound of vessels of head and neck Ther ult head & neck ves 0002 Therapeutic ultrasound of heart Ther ultrasound of heart 0003 Therapeutic ultrasound of peripheral vascular vessels Ther ult peripheral ves 0009 Other therapeutic ultrasound Other therapeutic ultsnd 0010 Implantation of chemotherapeutic agent Implant chemothera agent 0011 Infusion of drotrecogin alfa (activated) Infus drotrecogin alfa 0012 Administration of inhaled nitric oxide Adm inhal nitric oxide 0013 Injection or infusion of nesiritide Inject/infus nesiritide 0014 Injection or infusion of oxazolidinone class of antibiotics Injection oxazolidinone 0015 High-dose infusion interleukin-2 [IL-2] High-dose infusion IL-2 0016 Pressurized treatment of venous bypass graft [conduit] with pharmaceutical substance Pressurized treat graft 0017 Infusion of vasopressor agent Infusion of vasopressor 0018 Infusion of immunosuppressive antibody therapy Infus immunosup antibody 0019 Disruption of blood brain barrier via infusion [BBBD] BBBD via infusion 0021 Intravascular imaging of extracranial cerebral vessels IVUS extracran cereb ves 0022 Intravascular imaging of intrathoracic vessels IVUS intrathoracic ves 0023 Intravascular imaging of peripheral vessels IVUS peripheral vessels 0024 Intravascular imaging of coronary vessels IVUS coronary vessels 0025 Intravascular imaging of renal vessels IVUS renal vessels 0028 Intravascular imaging, other specified vessel(s) Intravascul imaging NEC 0029 Intravascular -
V5 Data Dictionary Supplement with Pending Data Element Updates
V5 Data Dictionary Supplement with Pending Data Element Updates The mission of the NCDR® is to improve the quality of cardiovascular patient CathPCI by providing information, knowledge and tools; implementing quality initiatives; and supporting research that improves patient CathPCI and outcomes. The NCDR® is an initiative of the American College of Cardiology Foundation, with partnering support from the Society for Cardiovascular Angiography and Interventions for the CathPCI Registry. CONFIDENTIALITY NOTICE This document contains information confidential and proprietary to the American College of Cardiology Foundation. This document is intended to be a confidential communication between ACCF and participants of the CathPCI Registry and may involve information or material that may not be used, disclosed or reproduced without the written authorization of the ACCF. Those so authorized may only use this information for a purpose consistent with the authorization. Reproduction of any section of this document with permission must include this notice. Table of Contents Section G. Cath Lab Visit Seq#7400 Indications for Cath Lab Visit....................................................................................Page 3 Seq#7405 Chest Pain Symptom Assessment…………………………………….…………………………………..Page 5 Section I. PCI Procedure Seq#7825 Percutaneous Coronary Intervention Indication......................................................Page 6 Review of Cath Lab Indications & PCI Indications…………………………………………….….….……….…. Page 8 Section K. Intra and Post-Procedure -

NCDR® Cathpci Registry® V4.4 Coder's Data Dictionary
NCDR® CathPCI Registry® v4.4 Coder's Data Dictionary A. Demographics Seq. #: 2000 Name: Last Name Coding Instructions: Indicate the patient's last name. Hyphenated names should be recorded with a hyphen. Target Value: The value on arrival at this facility Selections: (none) Supporting Definitions: (none) Seq. #: 2010 Name: First Name Coding Instructions: Indicate the patient's first name. Target Value: The value on arrival at this facility Selections: (none) Supporting Definitions: (none) Seq. #: 2020 Name: Middle Name Coding Instructions: Indicate the patient's middle name. Note(s): It is acceptable to specify the patient's middle initial. If the patient does not have a middle name, leave field blank. If the patient has multiple middle names, enter all of the middle names sequentially. Target Value: The value on arrival at this facility Selections: (none) Supporting Definitions: (none) Seq. #: 2030 Name: SSN Coding Instructions: Indicate the patient's United States Social Security Number (SSN). Note(s): If the patient does not have a US Social Security Number (SSN), leave blank and check 'SSN NA'. Target Value: The value on arrival at this facility Selections: (none) Supporting Definitions: (none) Seq. #: 2031 Name: SSN N/A Coding Instructions: Indicate if the patient does not have a United States Social Security Number(SSN). Target Value: The value on arrival at this facility Selections: Selection Text Definition No Yes Supporting Definitions: (none) Effective for Patient Discharges April 1, 2011 © 2008, American College of Cardiology Foundation 1/5/2011 3:12:46 PM Page 1 of 82 NCDR® CathPCI Registry® v4.4 Coder's Data Dictionary A. -
Provider Guide
Physician-Related Services/ Health Care Professional Services Provider Guide July 1, 2014 Physician-Related Services/Health Care Professional Services About this guide* This publication takes effect July 1, 2014, and supersedes earlier guides to this program. Washington Apple Health means the public health insurance programs for eligible Washington residents. Washington Apple Health is the name used in Washington State for Medicaid, the children's health insurance program (CHIP), and state- only funded health care programs. Washington Apple Health is administered by the Washington State Health Care Authority. What has changed? Reason for Subject Change Change Allowable conditions of the Changed “Acute” in title to “Allowable” and added More accurately fits lower extremities by diagnosis code 703.8 the list of diagnosis diagnosis codes Antepartum visits - Removed diagnosis codes. Providers must bill Clarification Additional monitoring for with a primary diagnosis that identifies that the high risk conditions high risk condition is pregnancy related and which is within the provider’s scope of practice. Developmental screening Added “per client, per provider” to the limitation Clarified limitation for CPT code 96111. Expedited Prior Assigned an EPA number to Q4116 Alloderm and This procedure Authorization Criteria added it to the EPA list requires EPA Coding List Expedited Prior Added diagnosis code V74.1 to EPA# 1325 Clarified allowable Authorization Criteria diagnosis codes Coding List Facet neurotomy Updated policy. Removed erroneous -

ACC/AHA Guidelines for Coronary Angiography
Journal of the American College of Cardiology Vol. 33, No. 6, 1999 © 1999 by the American College of Cardiology and the American Heart Association, Inc. ISSN 0735-1097/99/$20.00 Published by Elsevier Science Inc. PII S0735-1097(99)00126-6 ACC/AHA PRACTICE GUIDELINES ACC/AHA Guidelines for Coronary Angiography A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Coronary Angiography) Developed in collaboration with the Society for Cardiac Angiography and Interventions COMMITTEE MEMBERS PATRICK J. SCANLON, MD, FACC, Co-Chair and DAVID P. FAXON, MD, FACC, Co-Chair ANNE-MARIE AUDET, MD, MSC, SM, FACP DONALD F. LEON, MD, FACC BLASE CARABELLO, MD, FACC JOHN A. MURRAY, MD, FACC GREGORY J. DEHMER, MD, FACC STEVEN E. NISSEN, MD, FACC KIM A. EAGLE, MD, FACC CARL J. PEPINE, MD, FACC RONALD D. LEGAKO, MD, FAAFP RITA M. WATSON, MD, FACC TASK FORCE MEMBERS JAMES L. RITCHIE, MD, FACC, Chair and RAYMOND J. GIBBONS, MD, FACC, Vice Chair MELVIN D. CHEITLIN, MD, FACC RICHARD O. RUSSELL, JR, MD, FACC KIM A. EAGLE, MD, FACC THOMAS J. RYAN, MD, FACC TIMOTHY J. GARDNER, MD, FACC SIDNEY C. SMITH, JR, MD, FACC ARTHUR GARSON, JR, MD, MPH, FACC TABLE OF CONTENTS II. General Considerations Regarding Coronary Angiography..............................................................................1759 Preamble .............................................................................................1757 A. Definitions ..........................................................................1759 -

PBA Thrombo-Embolectomy
Vascular Surgery PBA: Thrombo-Embolectomy Trainee: Assessor: Date: Assessor's Position*: Email (institutional): GMC No: Duration of procedure (mins): Duration of assessment period (mins): Hospital: Operation more difficult than usual? Yes / No (If yes, state [ ] Tick this box if this PBA was performed in a Simulated reason) setting. [ ]Basic (e.g. straightforward brachial embolectomy) Complexity (tick which applies, if any) [ ]Intermediate (e.g. thrombolyis for residual thrombo-embolus) [ ]Advanced (e.g. popliteal embolectomy and vein patch repair) [ ]Involved vessel: (circle one) Femoral - Popliteal - Brachial - Subtype (tick which applies, if any) Other * Assessors are normally consultants (senior trainees may be assessors depending upon their training level and the complexity of the procedure) IMPORTANT: The trainee should explain what he/she intends to do throughout the procedure. The Assessor should provide verbal prompts if required, and intervene if patient safety is at risk. Rating: N = Not observed or not appropriate D = Development required S = Satisfactory standard for CCT (no prompting or intervention required) Rating Competencies and Definitions Comments N/D/S I. Consent Demonstrates sound knowledge of indications and contraindications including C1 alternatives to surgery Demonstrates awareness of sequelae of operative or non operative C2 management C3 Demonstrates sound knowledge of complications of surgery Explains the procedure to the patient / relatives / carers and checks C4 understanding C5 Explains likely outcome and time to recovery and checks understanding II. Pre operation planning Demonstrates recognition of anatomical and pathological abnormalities (and PL1 relevant co-morbidities) and selects appropriate operative strategies / techniques to deal with these Demonstrates ability to make reasoned choice of appropriate equipment, PL2 materials or devices (if any) taking into account appropriate investigations e.g.