Table of Contents
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Are There Effective Ultrasound Parameters in the Management of Lateral Elbow Tendinopathy? a Systematic Review of the Literature
hysical M f P ed l o ic a in n r e u & International Journal of o Stasinopoulos et al., Int J Phys Med Rehabil 2013, 1:3 R J l e a h n DOI: 10.4172/2329-9096.1000117 a o b i t i l a ISSN: 2329-9096i t a n r t i e o t Physical Medicine & Rehabilitation n n I Research Article Open Access Are there Effective Ultrasound Parameters in the Management of Lateral Elbow Tendinopathy? A Systematic Review of the Literature Stasinopoulos Dimitrios*, Cheimonidou Areti-Zoe and Chatzidamianos Theodoros Program of Physiotherapy, Department of Health Sciences, School of Sciences European University of Cyprus 6, Diogenes Str. Engomi, P. O. Box 22006, 1516, Nicosia, Cyprus Abstract Objective: Lateral elbow tendinopathy (LET) is a common clinical condition, and a wide array of physiotherapy treatments is used for treating LET. One of the most common physiotherapy modality is the ultrasound. Ultrasound is a dose response modality. The aim of the present article was to determine the effective ultrasound parameters in the management of (LET) and to provide recommendations based on this evidence. Methods: Randomized controlled trials (RCTs) identified by a search strategy in six databases were used in combination with reference checking. RCTs that included positive effects with ultrasound, description of ultrasound parameters in details, patients with LET, and at least one of the clinically relevant outcome measure were selected. The Pedro scale was used to analyse the results. Results: None RCTs fulfilled the criteria and therefore all the conducted trials were excluded in the review. -
Signal Processing Techniques for Phonocardiogram De-Noising and Analysis
-3C).1 CBME CeaEe for Bionedio¡l Bnginocdng Adelaide Univenity Signal Processing Techniques for Phonocardiogram De-noising and Analysis by Sheila R. Messer 8.S., Urriversity of the Pacific, Stockton, California, IJSA Thesis submitted for the degree of Master of Engineering Science ADELAIDE U N IVERSITY AUSTRALIA Adelaide University Adelaide, South Australia Department of Electrical and Electronic Faculty of Engineering, Computer and Mathematical Sciences July 2001 Contents Abstract vi Declaration vll Acknowledgement vul Publications lx List of Figures IX List of Tables xlx Glossary xxii I Introduction I 1.1 Introduction 2 t.2 Brief Description of the Heart 4 1.3 Heart Sounds 7 1.3.1 The First Heart Sound 8 1.3.2 The Second Heart Sound . 8 1.3.3 The Third and Fourth Heart Sounds I I.4 Electrical Activity of the Heart I 1.5 Literature Review 11 1.5.1 Time-Flequency and Time-Scale Decomposition Based De-noising 11 I CO]VTE]VTS I.5.2 Other De-noising Methods t4 1.5.3 Time-Flequency and Time-Scale Analysis . 15 t.5.4 Classification and Feature Extraction 18 1.6 Scope of Thesis and Justification of Research 23 2 Equipment and Data Acquisition 26 2.1 Introduction 26 2.2 History of Phonocardiography and Auscultation 26 2.2.L Limitations of the Hurnan Ear 26 2.2.2 Development of the Art of Auscultation and the Stethoscope 28 2.2.2.L From the Acoustic Stethoscope to the Electronic Stethoscope 29 2.2.3 The Introduction of Phonocardiography 30 2.2.4 Some Modern Phonocardiography Systems .32 2.3 Signal (ECG/PCG) Acquisition Process .34 2.3.1 Overview of the PCG-ECG System .34 2.3.2 Recording the PCG 34 2.3.2.I Pick-up devices 34 2.3.2.2 Areas of the Chest for PCG Recordings 37 2.3.2.2.I Left Ventricle Area (LVA) 37 2.3.2.2.2 Right Ventricular Area (RVA) 38 oaooe r^fr /T ce a.!,a.2.{ !v¡u Ãurlo¡^+-;^l ¡rr!o^-^^ \!/ ^^\r¡ r/ 2.3.2.2.4 Right Atrial Area (RAA) 38 2.3.2.2.5 Aortic Area (AA) 38 2.3.2.2.6 Pulmonary Area (PA) 39 ll CO]VTE]VTS 2.3.2.3 The Recording Process . -

An Integrated Framework for Cardiac Sounds Diagnosis
Western Michigan University ScholarWorks at WMU Master's Theses Graduate College 12-2015 An Integrated Framework for Cardiac Sounds Diagnosis Zichun Tong Follow this and additional works at: https://scholarworks.wmich.edu/masters_theses Part of the Computer Engineering Commons, and the Electrical and Computer Engineering Commons Recommended Citation Tong, Zichun, "An Integrated Framework for Cardiac Sounds Diagnosis" (2015). Master's Theses. 671. https://scholarworks.wmich.edu/masters_theses/671 This Masters Thesis-Open Access is brought to you for free and open access by the Graduate College at ScholarWorks at WMU. It has been accepted for inclusion in Master's Theses by an authorized administrator of ScholarWorks at WMU. For more information, please contact [email protected]. AN INTEGRATED FRAMEWORK FOR CARDIAC SOUNDS DIAGNOSIS by Zichun Tong A thesis submitted to the Graduate College in partial fulfillment of the requirements for a degree of Master of Science in Engineering Electrical and Computer Engineering Western Michigan University December 2015 Thesis Committee: Ikhlas Abdel-Qader, Ph.D., Chair Raghe Gejji, Ph.D. Azim Houshyar, Ph.D. AN INTEGRATED FRAMEWORK FOR CARDIAC SOUNDS DIAGNOSIS Zichun Tong, M.S.E. Western Michigan University, 2015 The Phonocardiogram (PCG) signal contains valuable information about the cardiac condition and is a useful tool in recognizing dysfunction and heart failure. By analyzing the PCG, early detection and diagnosis of heart diseases can be accomplished since many pathological conditions of the cardiovascular system cause murmurs or abnormal heart sounds. This thesis presents an algorithm to classify normal and abnormal heart sound signals using PCG. The proposed analysis is based on a framework composed of several statistical signal analysis techniques such as wavelet based de-noising, energy-based segmentation, Hilbert-Huang transform based feature extraction, and Support Vector Machine based classification. -

ICD~10~PCS Complete Code Set Procedural Coding System Sample
ICD~10~PCS Complete Code Set Procedural Coding System Sample Table.of.Contents Preface....................................................................................00 Mouth and Throat ............................................................................. 00 Introducton...........................................................................00 Gastrointestinal System .................................................................. 00 Hepatobiliary System and Pancreas ........................................... 00 What is ICD-10-PCS? ........................................................................ 00 Endocrine System ............................................................................. 00 ICD-10-PCS Code Structure ........................................................... 00 Skin and Breast .................................................................................. 00 ICD-10-PCS Design ........................................................................... 00 Subcutaneous Tissue and Fascia ................................................. 00 ICD-10-PCS Additional Characteristics ...................................... 00 Muscles ................................................................................................. 00 ICD-10-PCS Applications ................................................................ 00 Tendons ................................................................................................ 00 Understandng.Root.Operatons..........................................00 -
2019 State of the Field Report in Part Or Its Entirety
State of 20the Field 19 Focused Ultrasound The Focused Ultrasound Foundation encourages widespread No part of this report may be reproduced for commercial purposes in any written, distribution of the 2019 State of the Field Report in part or its entirety. electronic, recording, or photocopy form or stored in a retrieval system without the written permission of the Focused Ultrasound Foundation. Inquiries for reproduction can be directed to Emily White at The Focused Ultrasound Foundation strives to provide the most accurate information [email protected]. possible and therefore works proactively with the manufacturers and research sites to collect the most current data available in advance of the release of this publication. Date 8.6.0019 This report is based on data through December 31, 2018. The Focused Ultrasound © 2019 Focused Ultrasound Foundation. All rights reserved. Foundation assumes no responsibility for any errors or omissions as every precaution has been taken to verify the accuracy of the information contained herein. No liability is assumed for damages that may result from the use of information contained within. If you note something out of date or inaccurate, please submit the new information/updates to: [email protected]. 3 Focused Ultrasound Foundation | State of the Field 2019 CONTENTS 2 Introduction 59 Veterinary Medicine 2 Letter From the Chairman 59 FUS Veterinary Applications 3 Focused Ultrasound in Brief 60 State of Research by Indication 4 Overview 60 Developmental Landscape 4 State of Research and -

Chapter 2 Ballistocardiography
POLITECNICO DI TORINO Corso di Laurea Magistrale in Ingegneria Biomedica Tesi di Laurea Magistrale Ballistocardiographic heart and breathing rates detection Relatore: Candidato: Prof.ssa Gabriella Olmo Emanuela Stirparo ANNO ACCADEMICO 2018-2019 Acknowledgements A conclusione di questo lavoro di tesi vorrei ringraziare tutte le persone che mi hanno sostenuta ed accompagnata lungo questo percorso. Ringrazio la Professoressa Gabriella Olmo per avermi dato la possibilità di svolgere la tesi nell’azienda STMicroelectronics e per la disponibilità mostratami. Ringrazio l’intero team: Luigi, Stefano e in particolare Marco, Valeria ed Alessandro per avermi aiutato in questo percorso con suggerimenti e consigli. Grazie per essere sempre stati gentili e disponibili, sia in campo professionale che umano. Un ringraziamento lo devo anche a Giorgio, per avermi fornito tutte le informazioni e i dettagli tecnici in merito al sensore utilizzato. Vorrei ringraziare anche tutti i ragazzi che hanno condiviso con me questa esperienza ed hanno contribuito ad alleggerire le giornate lavorative in azienda. Ringrazio i miei amici e compagni di università: Ilaria e Maria, le amiche sulle quali posso sempre contare nonostante la distanza; Rocco, compagno di viaggio, per i consigli e per aver condiviso con me gioie così come l’ansia e le paure per gli esami; Valentina e Beatrice perché ci sono e ci sono sempre state; Rosy, compagna di studi ma anche di svago; Sara, collega diligente e sempre con una parola di supporto, grazie soprattuto per tutte le dritte di questo ultimo periodo. Il più grande ringraziamento va ai miei genitori, il mio punto di riferimento, il mio sostegno di questi anni. -

Extracorporeal Shockwave Therapy Versus Ultrasound Therapy For
medRxiv preprint doi: https://doi.org/10.1101/2020.09.20.20198168; this version posted September 22, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY-ND 4.0 International license . Extracorporeal Shockwave Therapy Versus Ultrasound Therapy for Plantar Fasciitis: Systematic Review and Meta-Analysis Zeyana Al-Siyabi1*, Mohammad Karam2*, Ethar Al-Hajri1, Abdulmalik Alsaif2 1 Podiatry BSc (Hons), University of Huddersfield, Huddersfield, United Kingdom. 2 Department of Medicine, University of Leeds, Leeds, United Kingdom. * Z.A. and M.K. contributed equally as first co-authors. Corresponding Author: Mohammad Karam Address: Al-Firdous, Block 4, Street 1, Avenue 6, Al-Farwaniyah, State of Kuwait. Phone: +965 9916272, +44 7480644489 Email: [email protected] NOTE: This preprint reports new research that has not been certified by peer review and should not be used to guide clinical practice. 1 medRxiv preprint doi: https://doi.org/10.1101/2020.09.20.20198168; this version posted September 22, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY-ND 4.0 International license . Abstract Objective To compare the outcomes of Extracorporeal Shockwave Therapy (ESWT) versus Ultrasound Therapy (UST) in plantar fasciitis. Methods A systematic review and meta-analysis were performed. An electronic search identifying studies comparing ESWT and UST for plantar fasciitis was conducted. -

Letter to the Editor: Malignant Meningiomas
J Neurosurg 122:1511–1519, 2015 Letters to the Editor NEUROSURGICAL FORUM Predictors of outcome for gunshot gunshot wounds, particularly if non-neurosurgeons in the emergency department triage the patients. It provides wounds rapid and accurate early information for patients and their families. TO THE EDITOR: I have read with great interest the I was intrigued by the fact that in our study, 39% of article by Gressot et al.1 (Gressot LV, Chamoun RB, Pa- patients achieved a functional survival status compared to tel AJ, et al: Predictors of outcome in civilians with gun- 19% in the authors’ study. The extent of injury caused by shot wounds to the head upon presentation. J Neurosurg a bullet is determined to the greatest degree at the time 121:645–652, September 2014). The authors concluded of impact and is dependent on bullet mass and exit muz- that several factors, including patient age, Glasgow Coma zle velocity squared. Passage of the bullet through brain Scale score, nonreactive pupils, and the path of the bullet tissue creates waves of massive increases in intracranial and its fragments on CT scans, have predictive value for pressure in the wake of the bullet. Based on the above for- patient survival, and they created a scoring system based mula, the damage is greater with a greater bullet mass and on these parameters. In their series of 119 patients 19% greater muzzle exit velocity such as that seen in military had good functional survival. We published an article in grade weapons. Thus, the degree of neurological deficit 2 1979 dealing with the same issues. -

The Proceedings of the World Neurosurgery Webinar Conference 2020
The Proceedings of the World Neurosurgery Webinar Conference 2020 Editor G Narenthiran FRCS(SN) Neurosurgery Research Listserv The Proceedings of the World Neurosurgery Webinar Conference Abstract 1 [Poster] Xanthogranuloma in the suprasellar region: a case report Mechergui H, Kermani N, Jemel N, Slimen A, Abdelrahmen K, Kallel J Neurosurgical department, National Institute of Neurology of Tunis Contact: [email protected]; Tunisia Conict of interests: none Objective: Xanthogranuloma, also known as cholesterol granuloma, is extremely rare. It represents approximately 1.9% of tumours in the sellar and parasellar region with 83 cases recognised in the literature. The preoperative diagnosis is dicult due to the lack of clinical and radiological specicities. Through this work, we report the third case of xanthogranuloma in the sellar region described in Tunisia. The Proceedings of the World Neurosurgery Webinar Conference Page 1 The Proceedings of the World Neurosurgery Webinar Conference Method: We report the case of 29-year-old girl who was followed up since 2012 for delayed puberty. The patient presented with a 1-year history of decreased visual acuity on the right side. On ophthalmological examination her visual acuity was rated 1/10 with right optic atrophy. Biochemical studies revealed ante-pituitary insuciency. The MRI demonstrated a sellar and suprasellar lesion with solid and cystic components associated with calcication evoking in the rst instance a craniopharyngioma. She underwent a total resection of the tumour by a pterional approach. Result: The anatomopathological examination concluded the lesion to be an intrasellar Xanthogranuloma. Conclusion: Sellar xanthogranuloma is a rare entity that is dicult to diagnose preoperatively due to its similarities with other cystic lesions of the sellar region, especially craniopharyngioma. -

Introduction
RIMS, IMPHAL ANNUAL REPORT 2014-15 INTRODUCTION 1. DESCRIPTION : The Regional Institute of Medical Sciences (RIMS), Imphal was established in the year 1972. It is an institution of regional importance catering to the needs of the North Eastern Region in the field of imparting undergraduate and post graduate medical education.The Institution brings together educational facilities for the training of personnel in all important branches of medical specialities including Dental and Nursing education in one place. The Institute is affiliated to the Manipur University, Canchipur, Imphal. 2. MANAGEMENT : The Institute was transferred to the Ministry of Health & Family Welfare, Government of India from North Eastern Council, Shillong (under Ministry of DoNER, Government of India) w.e.f. 1st April, 2007. Under the existing administrative set-up, the highest decision making body is the Board of Governors headed by the Union Minister of Health & Family Welfare as the President and the Director of the Institute as the Secretary. The Executive Council is responsible for the management of the Institute. The Secretary, Ministry of Health & Family Welfare, Government of India is the Chairman of the Executive Council while the head of the Institute remains as Secretary. Thus, the institute is managed at two levels, namely the Board of Governors and the Executive Council. A. Board of Governors : 1. Hon’ble Union Minister, - President Health & Family Welfare, Government of India. 2. Hon’ble Chief Minister, Manipur. - Vice-President 3. A Representative of the Planning Commission, - Member Government of India. 4. Health Ministers of the Beneficiary States - Member 5. Secretary, Ministry of Health & Family Welfare, - Member Government of India. -
IVUS Imaging Catheters Reference Guide
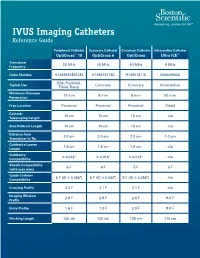
IVUS Imaging Catheters Reference Guide Peripheral Catheter Coronary Catheter Coronary Catheter Intracardiac Catheter OptiCross™ 18 OptiCross 6 OptiCross Ultra ICE™ Transducer 30 MHz 40 MHz 40 MHz 9 MHz Frequency Order Number H7493932800180 H7495181160 H749518110 M00499000 SFA, Popliteal, Typical Use Coronary Coronary Intracardiac Tibial, Renal Maximum Diameter 12 mm 6 mm 6 mm 50 mm Penetration Prep Location Proximal Proximal Proximal Distal Catheter 15 cm 15 cm 15 cm n/a Telescoping Length Sled Pullback Length 10 cm 10 cm 10 cm n/a Distance from 2.0 cm 2.0 cm 2.0 cm 1.0 cm Transducer to Tip Guidewire Lumen 1.6 cm 1.6 cm 1.6 cm n/a Length Guidewire ≤ 0.018" ≤ 0.014" ≤ 0.014" n/a Compatibility Sheath Compatibility 6 F 6 F 5 F 9 F (with max wire) Guide Catheter 6 F (ID ≥ 0.068") 6 F (ID ≥ 0.064") 5 F (ID ≥ 0.058") n/a Compatibility Crossing Profile 3.5 F 3.1 F 3.1 F n/a Imaging Window 2.9 F 2.9 F 2.6 F 9.0 F Profile Entry Profile 1.6 F 1.3 F 2.0 F 9.0 F Working Length 135 cm 135 cm 135 cm 110 cm OPTICROSS™ 18 CATHETER AND MDU5 PLUS BAG OPTICROSS 6 40 MHZ CORONARY IMAGING CATHETER CAUTION Federal law (USA) restricts this device to sale by or on the order of a physician. Rx only. Prior to use, please see the CAUTION: Federal law (USA) restricts this device to sale by or on the order of a physician. -

Subtemporal Transparahippocampal Amygdalohippocampectomy for Surgical Treatment of Mesial Temporal Lobe Epilepsy Technical Note
Subtemporal transparahippocampal amygdalohippocampectomy for surgical treatment of mesial temporal lobe epilepsy Technical note T. S. Park, M.D., Blaise F. D. Bourgeois, M.D., Daniel L. Silbergeld, M.D., and W. Edwin Dodson, M.D. Department of Neurology and Neurological Surgery, Washington University School of Medicine, and St. Louis Children's Hospital, St. Louis, Missouri Amygdalohippocampectomy (AH) is an accepted surgical option for treatment of medically refractory mesial temporal lobe epilepsy. Operative approaches to the amygdala and hippocampus that previously have been reported include: the sylvian fissure, the superior temporal sulcus, the middle temporal gyrus, and the fusiform gyrus. Regardless of the approach, AH permits not only extirpation of an epileptogenic focus in the amygdala and anterior hippocampus, but interruption of pathways of seizure spread via the entorhinal cortex and the parahippocampal gyrus. The authors report a modification of a surgical technique for AH via the parahippocampal gyrus, in which excision is limited to the anterior hippocampus, amygdala and parahippocampal gyrus while preserving the fusiform gyrus and the rest of the temporal lobe. Because transparahippocampal AH avoids injury to the fusiform gyrus and the lateral temporal lobe, it can be performed without intracarotid sodium amobarbital testing of language dominance and language mapping. Thus the operation would be particularly suitable for pediatric patients in whom intraoperative language mapping before resection is difficult. Key Words * amygdalohippocampectomy * complex partial seizure * parahippocampal gyrus * subtemporal approach Currently several different variations of temporal lobe resections are used for medically intractable complex partial seizures.[4,6,8,18,21,30,34] Among these operations is amygdalohippocampectomy (AH), first described in 1958 by Niemeyer,[16] who approached the amygdala and hippocampus through an incision on the middle temporal gyrus.