Citalopram Improves Metabolic Risk Factors Among High Hostile Adults: Results of a Placebo-Controlled Intervention
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

To the City. to the World. from the Classroom
From the Classroom. To the City. To the World. Ranked among the nation’s best business schools, Pitt Business will take you From the Classroom, To the City, To the World. This journey is a transformational experience. You will forge your own path by taking courses that are globally focused and grounded in experience-based learning. You will develop a professional network to advance your career opportunities. And, you will have the confidence to succeed because of the exceptional support that you will receive from our outstanding faculty and professional staff. From the Ranking of Public Business Schools Best Business School Classroom #12 – Poets & Quants Business School in PA Business Schools by Recruiters #1 – Poets & Quants #4 – Bloomberg Businessweek “Getting Grads the Jobs They Want” Career Advising #1 – Poets & Quants #6 – Poets & Quants for Student Diversity TOP of Public Business Schools #2 – Poets & Quants – U.S. News & World Report & Bloomberg Businessweek Academic Advising 20 #3 – Poets & Quants Explore Your Options Academic Excellence Learn From Two Kinds of Teachers: Business Majors Acclaimed Faculty and Real-World Experience Strong academics are the foundation of Pitt Business. While studying for the Bachelor of Accounting Business Information Systems Science in Business Administration degree, you have endless options to customize your education to fit your ideal career path. You can double major in business and complete cross-disciplinary business certificates. You Finance Global Management can also enroll in our accelerated degree programs — including an MS in Accounting, MS in Information Systems, and an MBA — which allow you to earn both your bachelor’s and master’s degrees in around four years. -

Asian Studies (Mar/Aas)
44th ANNUAL CONFERENCE MID-ATLANTIC REGION ASSOCIATION FOR ASIAN STUDIES (MAR/AAS) ASIACONFLICT AND COOPERATION OCTOBER 9-11, 2015 UNIVERSITY OF PITTSBURGH ASIAN STUDIES CENTER UNIVERSITY CENTER FOR INTERNATIONAL STUDIES maraas.org | http://www.ucis.pitt.edu/asc/ UNIVERSITY OF PITTSBURGH | 1 CONTENTS Message from the MAR/AAS President......................................4 Welcome from ARIEL ARMONY................................................6 Senior Director of International Programs Director, University Center for International Studies Conference Overview...............................................................7 Guest Speakers.........................................................................8 Friday Guest Speaker: WILLIAM TSUTSUI Annual Luncheon Keynote: DAYONG NIU Distinguished Asianist: FRANK L. CHANCE Teaching Asia Workshop...........................................................11 Cultural Performances..............................................................12 Conference Program Session A.......................................................................15 Session B.......................................................................18 Session C.......................................................................20 Session D.......................................................................24 Session E........................................................................27 Session F........................................................................30 Conference Credits...................................................................32 -

Residential Handbook 2015–16 WELCOME
Residential Handbook 2015–16 WELCOME Welcome to University of Pittsburgh on-campus housing! Whether you are living in a residence hall, apartment-style accommodation, or fraternity complex, you are one of over 7,900 undergraduate students residing on campus, and your comfort and satisfaction are very important to us. It is our priority to ensure that your time in on-campus housing is one of many positive and rewarding experiences here at Pitt. The purpose of this Handbook is not only to provide you with a comprehensive reference for living on campus, but also to advise you of the policies for residing in University housing. This Handbook is not, and does not, create a contract. Upon electronically signing your Housing and Dining Services Contract (Contract), you agreed to, among other things, abide by the policies, rules, and regulations set forth in this Handbook and any other official University publications, including, but not limited to, the Student Code of Conduct and Judicial Procedures. Communal campus living can be a great college experience, but with your decision to do so comes a responsibility to abide by the rules necessary for the safety and enjoyment of all. With your cooperation, this goal will be met. This Handbook is divided into two sections. The first section (Everyday Living) addresses matters specifically related to your occupancy of University housing. The second section (Resources and Services) provides other useful information pertaining to the University. Each section has been organized alphabetically for easy reference. If you have any questions or need any additional assistance, please feel free to contact Panther Central at 412-648-1100, [email protected], or www.pc.pitt.edu. -
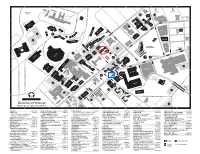
Campus Map 2006–07(09-2006) UPSB
A I B I C I D I E I F I G BRA N E . CKENRIDGE BAPS . T B X CATHO MELWD ATHLETIC T ELLEF E FIELDS P P SP Y DRIV R IS T U AUL D CHDEV E S BELLT LKS I T F K E P AR ELD WEBSR E FA ARKM IN N R AW 1 VA E CR 1 R NUE R T E LEVT C A H AV T Y FIFT S RUSK U E G V S MP A O N N E MUSIC SOUTH CRAIG STREE T N B N LA N A UNIVERSIT R N Y U COS P A W O P S E P VE SO I UCT P LO O . S S U L P HENRY ST T U H E Y N A D L UTD N . Q T C U I L G FR E N T A CRAI S. MELLI L BIG TH B O Y V L C I AT I A N E O BELLEFIELD E CHVR . UE EBER E V HOLD R P MP V A N D I I OP ST. V WINTHR R R IT E M E D D C VE V PANTH N A FRAT I AT ALU H R Y Y U FR T R I T SRC CRGSQ D U S E TH T N I R I Z BELLH V E ID S F S M B P R AW D IG FI HEIN . O L E TH G FILMORE ST L N PAHL V EH UN I ET O SOSA E A E IL A N E F I LO R VE L U PA R S 2 A TR T 2 R RSI W A T N T C LRDC VNGR S CATHEDRAL . -
Pitt Campus Map 2002
A I B I C I D I E I F I G BRACKENRIDGE N. BAPST ➮ ➮ . BELLEFIELDCATHO MELWD T ATHLETIC X FIELDS P P SPAUL E RUSKIN AVENUEIS ➮ PAR T CHDEV T BELL E E FALKS ARD KMA WF 1 E VA V CR 1 I R TENNYSONCRA RUSKN FIFTH AVENUE T R N AVE. MP MUSIC SOUTH S D LANGY N COST Y P UCTR SOUTH O LYTTON AVENUE SUTHD T HENRY ST. S I UTD S CLAPP N MELLI CRAIG I F S. R R AVE. BIGELOW BOULEV CRAIG III III B A I T E V CHVRN O I EBERL E HOLDY BELLEFIELD P MP N V U DITHRIDGE ST. R I WINTHROP R VENUE T D FRAT ALUM FRA Y T SRCC CRGSQ I BELLH STREET S M ST. P R A BIGELOW BOULEV E HEINZ THAW UNIVERSITY S FIFTH A FILMORE ST. V O I EH S N ILLO U PAA 2 AR 2 ST. C VNGRF STREET CATHEDRAL LRDC AVE. JUC OF LEARNING PBE FCRG MINRL ALLEN P LUC THACKERAGSCC CL TREES PLACE HARA P O' THACK UCLUB S C ENGUD LA U P ARD A STREET U T S TEPH LOGCB H H M PRES PCNTR D D YST. E T MP R N MP FHOUS N. BOUQUETE STREET E L B N U A DE E N AV D AMOS SO WPU E S T FRICK B ALLEQUIPP -D R E MP O R T F I E O STRE MCCOR V BOOK CARNG E R T SCAIF PUBHL S BRUCE P S DARRAGH HOLLD P C D E RS SALK ET BRACK H U C B 3 A 3 R TOW E N R C O A N S R PRESB HLMAN E L B E T WRN E I P LA I N T CHILD Y BSTWR S H STREET DR. -

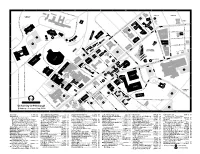
Pitt Campus Map 2005-06
A I B I C I D I E I F I G BRACKENRIDGE N BAPST . ➮ ➮ . BELLEFIELDCATHO MELWD T ATHLETIC X FIELDS P P SPAUL E ➮ RUSKIN IS P CHDEV T ARKMA BELLT T E FALKS WEBSR E 1 E CR 1 VA E VENUE R CRAWF R TENNYSON A FIFTH A T RUSKN T N MP S VENUE MUSIC SOUTH S LANGY A BOULEVARD LANGY UNIVERSITY DRIVE A VE. P N COST P P I UCTR SOUTH DITHRIDGE ST. O SUTHD LYTTON AVENUE HENRY ST. U S UTDC Q CLAPP N FRAT E CLAPP MELLI CRAIG I L AVE. S. BELLEFIELD AVE. L BIGELOW CRAIG STR III III B A E CHVRN O V EBERL E HOLDY P MP I V R I WINTHROP ST. R R VENUE E T D D FRAT I V Y ALUM FRA I T Y SRCC R U R S I T BELLH CRGSQ D N I V E S ST P RESIDENCE HALL R BIGELOW D E HEINZ UNDER PAHLL V THAW UNIVER FIFTH A FILMORE ST. N I OEH SOSAM CONSTRUCTION N EET A U PAA 2 L 2 SITY CARRILLO R LRDC VNGRF STREET CATHEDRAL JUC E OF LEARNING PBE ALLEN FBCRG P BOULEV H TH GSCC CL TREES STREET PLACE T HARA A LUC A U P O' C THACK UCLUB S KE P ENGUD ARD R LAC A UP STEPH LOGCB PCNTR YST.PRES TDH MP N. BO MP FHOUS BENDM AVENUE ALLEQUIPP DESOTO AMOS U WPU FORBES T QUET FRICK MP EE MCCOR BOOK CARNG STREET STREET STR SCAIF PUBHL BRUCE P DARRAGH HOLLD SCHENLEY D PLAZA E SCHENLEY SALK BRACK U C B 3 OWRS UNDER 3 R T N RA C CONSTRUCTION O A S R PRESB E HLMAN B E T WRN I P LA I N T CHILD MP BSTWR S H STREET LOTHP D O MDAR R. -

University of Pittsburgh Sustainable Energy Efforts
2/3/2020 University of Pittsburgh Sustainable Energy Efforts Dr. Aurora Sharrard Director of Sustainability 1-30-20 for Sustainable Pittsburgh, Energy Smart Operations 1 Snapshot 1) Pitt Context 2) Pitt Sustainability Background 3) Goals & Progress • Energy Use • Design Standards • GHG Emissions • Renewables • Electrifying Fleet 2 2 1 2/3/2020 Pitt Fast Facts • Founded in 1787 • 28,400 students • 13,200 faculty and staff • 518 degree & certificate programs • 3.2 miles East of Downtown • 131 buildings • 146 Acres • 13.8M gross square feet • + 4 regional campuses 3 3 Pitt Definition of “Sustainability” EQUITY The University of Pittsburgh defines "sustainability" as balancing equity, Livable Reasonable environment, & economics so Sustainable current & future ENIVIRONMENT ECONOMICS generations can thrive. Viable 4 4 2 2/3/2020 5 Market Central The Perch at Sutherland 6 3 2/3/2020 Copyright © 2017, Green Building Alliance 7 7 Institutional Master Plan 8 8 4 2/3/2020 Pitt Capital Budget • FY17 = $ 110.0 million • FY19 = $ 339.5 million • FY18 = $ 251.7 million • FY20 = $ 641.0 million 9 9 10 10 5 2/3/2020 Pitt Sustainability Plan Goals: ! ! ! "! " # !$ 11 11 %& '! (!! 12 6 2/3/2020 %& '! (!! 13 14 14 7 2/3/2020 Pitt Sustainability Plan Goal: ! ! ! 15 15 Energy & Water Conservation Project PHASE 1 PHASE 2 1) 3343 Forbes Avenue 1) Allen Hall 2) Benedum Hall 2) Alumni Hall 3) Biomedical Science Tower 3 3) Barco Law Building 4) Center for Bioengineering 4) Cathedral of Learning 5) Chevron Science Center 5) Mervis Hall 6) Computer Center (RIDC) 6) Music Building 7) Eberly Hall 7) Old Engineering Hall 8) Langley Hall 8) Petersen Events Center 9) Life Sciences Annex 9) Plum Borough Research Facility 10) McGowan Institute for Regenerative Medicine 10) Sennott Square 11) Space Research Coordination Center 11) Thaw Hall 12) Stephen Foster Memorial 12) Victoria Hall 13) Trees Hall 13) Wesley W. -
Curriculum Vitae Do Not Use for Proposals Biographical
CURRICULUM VITAE DO NOT USE FOR PROPOSALS BIOGRAPHICAL Name: Wendy M. Troxel, Ph.D. Business Address RAND Corporation E-Mail Address: [email protected] (as of September 24, 4570 Fifth Avenue 2012): Suite 600 Pittsburgh, PA 15213 Business Phone: (412) 683-2300 X 4427 Business Fax: (412) 683-2800 EDUCATION AND TRAINING UNDERGRADUATE: September 1991- Bucknell University Bachelor of Arts with Psychology and Theatre August 1995 Lewisburg, PA High Distinction 1995 September 1993 - University of Pittsburgh Semester at Sea December 1993 Pittsburgh, Pennsylvania GRADUATE: September 1999 – University of Pittsburgh Master of Science, 2001 Clinical and Biological March 2001 Pittsburgh, Pennsylvania and Health Psychology April 2001 – University of Pittsburgh Doctorate, 2006 Clinical and Biological April 2006 Pittsburgh, Pennsylvania and Health Psychology September 2005- Western Psychiatric Predoctoral Clinical Paul Pilkonis, Ph.D. and September 2006 Institute and Clinic Psychology Internship Marsha Marcus, Ph.D. 3811 O’Hara Street Pittsburgh, PA 1999-2004 University of Pittsburgh Predoctoral Fellowship in Pittsburgh, Pennsylvania Cardiovascular Behavior Medicine September 2004 – University of Pittsburgh Mellon Predoctoral May 2005 Pittsburgh, Pennsylvania Fellowship POSTGRADUATE: September 2006- Western Psychiatric Postdoctoral Scholar, Daniel J. Buysse, M.D., September 2008 Institute & Clinic University of Pittsburgh Karen A. Matthews, 3811 O’Hara Street Ph.D., and Martica Hall, Pittsburgh, PA Ph.D. September 2006- University of Pittsburgh NIMH Postdoctoral Daniel J. Buysse, M.D., April 2008 Pittsburgh, Pennsylvania Fellowship in Psychiatry Karen A. Matthews, MH016804 Ph.D., and Martica Hall, Ph.D. April 2008 – University of Pittsburgh NHLBI Postdoctoral Daniel J. Buysse, M.D., September 2008 Pittsburgh, Pennsylvania Fellowship in Sleep Karen A. Matthews, Medicine Ph.D. -
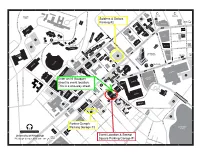
Pittcampusmap W Details 20190924.Pdf
. A T 1 X E T ATHLETI E E FIELDS R C I T S N O S B N I COST B O 2 R C A R R ILL O S T I BRA TREES P CKENRIDGE P C S VA U TH D FRAT M AT P FR I 3 T D D R I V E Q U I P P A STR EE N A LL E L A E T R E E P E H ANTH R T T ALKS R FHOUS S F U Y D R I V OB A H I T E S N U D S P D IP I U N O S N Q LE AL U UNIVERSIT N S I P DA V FRAT TR I S E ARKM R TREET P E PCNTR AHL S I I V RR T E Y D R L 4 E T AG A SALK N EBERL E H A C VE CHVRN DSA CE STREET P TERRA LRD U N I V E R S I T Y D R . AIF I V E SC VNGRF DES C S TDH OEH I T BSTWR P C THAW SRCC R ALLEN H P O EE O 'H ARA S TRE E T AR D E BI G EL O W B OULEV T UN L BAPS S P T N O R 5 T Y T . T HA U GSCC E I BO T VE UCTR P B ST N E ES BENDM ENGUD F N F PR CRAW S T T SOSAM . -
1:30Pm 2010 Ethics Forum Hosted by the University of Pittsburgh
2010 Ethics Forum Hosted by the UniversityEthics Forum of Pittsburgh 2007 Friday, June 25, 2010 9:00am – 1:30pm 9:00 a.m. Registration & Continental Breakfast Location: University Club, Ballroom B 9:20 a.m. Welcome and Introduction to the Forum 9:45 a.m. – 11:45 a.m. Breakout Sessions 12 noon Lunch Location: University Club, Ballroom B 12:30 p.m. Plenary Session: Carl J. Benson Fellow Engineer Bettis Laboratory Avoiding Collisions: Setting an Ethical Course in Research and in Practice Student Alphabetical Roster and Room Locations for Ethics Forum 2010 Last Name First Name Group School/Orgranization Group # Session # Room Adeli Mona PTEI PTEI 2 7 Benedum 226 Aizpitarle Daniela PTEI PTEI 4 9 Allen 103 Akalegbere Ogechi HHMI University of Pittsburgh 2 1 Benedum G 28 Albring Michael BMG University of Pittsburgh 1 8 Benedum 227 Alhassan Jamil HHMI University of Pittsburgh 2 1 Benedum G 28 Arrico Alexander PHYSICS University of Pittsburgh 2 3 Benedum G 34 Avrunin Eleanor ASPIRE University of Pittsburgh 1 10 Allen 105 Barefoot Nathan DUQ Duquesne University 1 1 Benedum G 28 Bennett Holly DUQ Duquesne University 1 1 Benedum G 28 Bifano Shawn PTEI PTEI 1 6 Benedum 158 Bishop Sarah SURE University of Pittsburgh 2 4 Benedum G 36 Blackwell Tenisha PTEI PTEI 3 8 Benedum 227 Bouobda Georges PTEI PTEI 3 8 Benedum 227 Bowman Charlie PHAGE University of Pittsburgh 1 10 Allen 105 Brancho James DUQ Duquesne University 1 1 Benedum G 28 Bray Eric CNUP University of Pittsburgh 4 8 Benedum 227 Budram Michael PRE-PHD University of Pittsburgh 1 7 Benedum 226 -

Proposed Institutional Master Plan Update University of Pittsburgh
Proposed Institutional Master Plan Update University of Pittsburgh Mid Campus District (Updated and Revised) Lower Campus District FINAL DRAFT January 29, 2010 Preface The University of Pittsburgh, one of the Nation’s oldest and most distinguished institutions of higher education, reaffirms its academic mission with planned improvements to the University’s facilities. This Institutional Master Plan Update reiterates the guiding principles established in the University of Pittsburgh Facilities Plan (1998-2007) along with the priorities developed in the University of Pittsburgh Facilities Plan (2007-2018). The University Facilities Management Division assembled a planning committee to update their Institutional Master Plan (IMP) for the Oakland Campus with the help of MacLachlan, Cornelius & Filoni, Inc. For purposes of planning, the Oakland Campus is divided into twelve campus districts. This IMP updates the previously planned Mid Campus district and it addresses planning issues in the Lower Campus district. One of the main goals of the IMP Update is to develop zoning guidelines to be approved by the City of Pittsburgh in order to facilitate future development in these districts. Beginning in late 2009, the University of Pittsburgh presented the proposed concepts included in this document and invited feedback from the Oakland Community Council, Oakland Task Force, Schenley Farms Civic Association, Bellefield Area Citizens Association and Part of the Solution Community Groups. Representatives of the Department of City Planning were consulted in determining the requirements of this document. Paragraphs identified with the * symbol represent the University of Pittsburgh’s commitment to sustainability and green initiatives. Note: Base maps showing buildings, streets, zoning boundaries, and topography were provided by the Department of City Planning, City of Pittsburgh. -

Pittsburgh Campus Map 2003Ð04 AR
A I B I C I D I E I F I G BRACKENRIDGE N. BAPST ➮ ➮ . BELLEFIELDCATHO MELWD T ATHLETIC X FIELDS P P SPAU E ➮ RUSKIN AVENUEIS PARKM T CHDEV T BELL L E FALKS ARD WF 1 E VA CR 1 R TENNYSONCRA AVE. E A RUSKN FIFTH AVENUE T V N AVE. I MP MUSIC SOUTH S R LANGY D N COST P Y UCTR SOUTH O SUTHD T LYTTON AVENUE I HENRY ST. S S CLAPP U TD N R MELLI CRAIG I F S. R E BIGELOW BOULEV CRAIG C III III V B A I T N CHVRN O U EBERL E BELLEFIELD P MP V HOLDY DITHRIDGE ST. R I WINTHROP R VENUE T D FRAT ALUM FRA Y T SRCC CRGSQ I BELLH STREET S M ST. P R A BIGELOW BOULEV E THAW UNIVERSITY S FIFTH A HEINZ FILMORE ST. I V O N EH S ILLO U PAA 2 AR 2 C ST. LRDC VNGRF STREET CATHEDRAL AVE. JUC OF LEARNING PBE FCRG ALLEN THACKERA P CL LUC TREES GSCC PLACE HARA P O' THACK UCLUB S C P ENGUD A U L A STREET P ARD T U STEPH H H M PRES LOGCB E PCNTR D D YST. R T N MP N. BOUQUETE STREET MP E FHOUS L B U A D E N N ESO AV D AMOS S T FRICK WPU E ALLEQUIPP -D R B R E T MP FO I OS V E MCCOR CARNG E R BOOK T S SCAIF PUBHL BRUCE P TRE S HOLLD DARRAGH C P D E RS SALK E BRACK H U C B 3 A T 3 R TOW E N R C O A N S R PRESB HLMAN E L B E T WRN E I P LA I N T CHILD Y BSTWR S H STREET DR.