RPH 2015-2016 Business Plan ( We Do/Business Plan)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

3Rd Lower Hutt Boy Scouts
1 2 DEDICATION This book is dedicated to future members of Laings Road Methodist Church. May their faith and action be relevant to the needs of the people of this city and may they pause to consider and record the history of which they are a part. LIMITED EDITION Published by the Laings Road Methodist Church, Lower Hutt in association with Methodist Publishing, Box 931, Christchurch. On our way: the first 150 years of the Methodist Church in Lower Hutt/authors, Tolla Williment. [et al.I. [Lower Hutt, N.Z.]: Laings Road Methodist Church in association with Methodist Publishing, [1989] 1 v. “New Zealand 1990 official project.” ISBN 0-908803-00-1 1. Laings Road Methodist Church (Lower Hutt, N.Z.) 2. Methodist Church — New Zealand — Lower Hutt — History. I. Williment, T. M. I. (Tolla Margaretta I.) 287. 19342 Printed by Wright & Carman. Typesetting by Artspec. Text by Jennifer Jones. Cover Design & Layout by Barrie Eady. 3 ‘On Our Way” is the story of Methodism in the Hutt Valley seen against a background of social change which has continuously affected the past 150 years. The book starts in pre-European times and traces the arrival of various waves of settlers and their attempts to set up churches in their new home. The eleven authors have researched widely over the past two years and provided an insight often lacking in chronological works. Generously illustrated and indexed, this book is a worthwhile addition to the historical records of the people of Lower Hutt. Pitt Henrich, designer and maker of the Pulpit Fall depicted on the cover of I this book, speaks of her work in this way — “This church wanted me to show how their work as Methodists with a tradition of social concern could go out from the church in the Hutt Valley to people everywhere. -
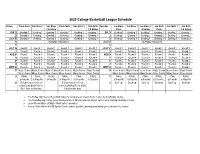
2020 CSW Basketball Handbook
2020 College Basketball League Schedule Friday Prem Boys Sen Boys 1 Sen Boys Prem Girls Sen Girls 1 Sen Girls Tuesday Jun Boys Jun Boys 1 Jun Boys 2 Jun Girls Jun Girls 1 Jun Girls 2 & below 2 & below Prem & below Prem 2 & below JUN 19 Grading 1 Grading 1 Grading 1 Grading 1 Grading 1 Grading 1 JUN 16 Grading 1 Grading 1 Grading 1 Grading 1 Grading 1 Grading 1 26 Grading 2 Grading 2 Grading 2 Grading 2 Grading 2 Grading 2 23 Grading 2 Grading 2 Grading 2 Grading 2 Grading 2 Grading 2 JULY 03 Grading 3 Grading 3 Grading 3 Grading 3 Grading 3 Grading 3 30 Grading 3 Grading 3 Grading 3 Grading 3 Grading 3 Grading 3 10 SCHOOL HOLIDAYS JULY 07 SCHOOL HOLIDAYS 17 14 JULY 24 Round 1 Round 1 Round 1 Round 1 Round 1 Round 1 JULY 21 Round 1 Round 1 Round 1 Round 1 Round 1 Round 1 31 Round 2 Round 2 Round 2 Round 2 Round 2 Round 2 28 Round 2 Round 2 Round 2 Round 2 Round 2 Round 2 AUG 07 Round 3 Round 3 Round 3 Round 3 Round 3 Round 3 AUG 04 Round 3 Round 3 Round 3 Round 3 Round 3 Round 3 14 Round 4 Round 4 Round 4 Round 4 Round 4 Round 4 11 Round 4 Round 4 Round 4 Round 4 Round 4 Round 4 21 Round 5 Round 5 Round 5 Round 5 Round 5 Round 5 18 Round 5 Round 5 Round 5 Round 5 Round 5 Round 5 28 Round 6 Round 6 Round 6 Round 6 Round 6 Round 6 25 Round 6 Round 6 Round 6 Round 6 Round 6 Round 6 SEPT 04 Round 7 Round 7 Round 7 Round 7 Round 7 Round 7 SEPT 01 Round 7 Round 7 Round 7 Round 7 Round 7 Round 7 11 Major Semis Major Semis Major Semis Major Semis Major Semis Major Semis 08 Major Semis Major Semis Major Semis Major Semis Major Semis Major Semis -

PUBLIC AGENDA V.2 Held on Wednesday 3 March Location: Hutt Hospital, Level 1, Clock Tower Building, Auditorium Room Zoom: 876 5068 1844 Time: 9.30Am MEETING
3 March PUBLIC Concurrent Board Meeting - Agenda PUBLIC AGENDA v.2 Held on Wednesday 3 March Location: Hutt Hospital, Level 1, Clock Tower Building, Auditorium Room Zoom: 876 5068 1844 Time: 9.30am MEETING Item Action Presenter Min Time Pg 1 PROCEDURAL BUSINESS 1.1 Karakia All members 1.2 Apologies ACCEPT Chair Public Participation 1.3 VERBAL Public - Nil Continuous Disclosure 1.4 1.4.1 Combined Board Interest Register ACCEPT Chair 1.4.2 Combined ELT Interest Register 15 9:30am 1.5 Minutes of Previous Concurrent Meeting ACCEPT Chair Matters Arising from Previous Concurrent 1.6 NOTE Chair Meetings 1.7 Chair’s Report and Correspondence NOTE Chair 1.8 Chief Executive’s Report NOTE Chief Executive Board Work Plan 2021 1.9 DISCUSS Chair 20 9:45am 1.9.1 Detailed Work Plan 2 DHB Performance and Accountability 2.1 HVDHB October 2020 Financial and NOTE Chief Financial Officer 10 10.05am Operational Performance Report Director Provider Services 2.1.1 Report 2.2 CCDHB October 2020 Financial and NOTE Chief Financial Officer Operational Performance Report Director Provider Services 2.2.1 Report 3 Updates 3.1 HSC Update and Items for Approval NOTE Chair of HSC 20 10.15am 4 OTHER 4.1 General Business NOTE Chair 5 10.35am 4.2 Resolution to Exclude the Public ACCEPT Chair 11:00 am - MORNING TEA – 15 min DATE OF NEXT FULL BOARD MEETING: 7 April 2021, Zoom: 876 5068 1844, Location: Wellington Regional Hospital, Level 11 Boardroom Grace Neil Block Hutt Valley and Capital & Coast District Health Boards Page 1 December 2020 1 3 March PUBLIC Concurrent Board -

2020 Futsal College Regionals | Senior Draw
COLLEGE SPORT WELLINGTON & CAPITAL FOOTBALL | 2020 FUTSAL COLLEGE REGIONALS | SENIOR DRAW Court 5/6 Court 7/8 Court 9/10 Court 11/12 Home Away Home Away Home Away Home Away 9:00 Wellington College Tawa College Aotea College Onslow College St Patrick's Town Naenae College Heretaunga College Hutt International 9:25 Rongotai College Wainuiomata High Hutt Valley High Kapiti College Scots College St Bernard's Upper Hutt St Pat's Silverstream 9:50 Wellington East Girls' Onslow College Queen Margaret HVHS Black Wellington Girls' HVHS White St Catherine's Sacred Heart 10:15 Onslow College Wellington College Tawa College Aotea College Hutt International St Patrick's Town Naenae College Heretaunga College 10:40 Kapiti College Rongotai College Wainuiomata High Hutt Valley High St Pat's Silverstream Scots College St Bernard's Upper Hutt 11:05 Queen Margaret Wellington East Girls' HVHS Black Onslow College St Catherine's Wellington Girls' Sacred Heart HVHS White 11:30 Tawa College Onslow College Wellington College Aotea College Naenae College Hutt International St Patrick's Town Heretaunga College 11:55 Wainuiomata High Kapiti College Rongotai College Hutt Valley High St Bernard's St Pat's Silverstream Scots College Upper Hutt 12:20 Onslow College Queen Margaret Wellington East Girls' HVHS Black HVHS White St Catherine's Wellington Girls' Sacred Heart 13:10 Boys Cup Quarter Final 1 (1st PA v 2nd PD) Boys Cup Quarter Final 2 (1st PB v 2nd PC) Boys Cup Quarter Final 3 (1st PC v 2nd PB) Boys Cup Quarter Final 4 (1st PD v 2nd PA) 13:35 Boys Plate Quarter -
2015 Sunday Festival Report and Survey Results
2015 Sunday Festival Report and Survey Results CONTENTS 1.0 INTRODUCTION ..................................................................................................................... 3 2.0 BACKGROUND ....................................................................................................................... 3 3.0 PURPOSE ................................................................................................................................ 3 4.0 FESTIVAL PROFILE .................................................................................................................. 4 5.0 SURVEY METHODOLOGY ..................................................................................................... 11 6.0 FINDINGS ............................................................................................................................. 12 Who came to Te Rā? ...................................................................................................... 12 Where did people at Te Rā festival come from? ............................................................ 13 How did people hear about Te Rā? ................................................................................ 14 What the Te Rā festival means for those who came...................................................... 14 What did people think of Te Rā 2015? ........................................................................... 16 Entertainment, hauora and mātauranga tents and the youth zone .............................. 17 Stalls food -

Ministry of Health Contracted Adolescent Dental Providers
Ministry of Health Contracted Adolescent Dental Providers Wellington Capital Dental Whai Oranga Newtown 125-129 Riddiford Street Dental - Cuc Dang 7 The Strand, Wainuiomata Angela McKeefry Level 3, The Dominion 389 8880 564 6966 473 7802 Bldg, 78 Victoria Street Newtown Newtown Dental Jaideep Ben Catherwood Surgery Vijayasenan 1st Level 90 The Terrace 100 Riddiford Street 11 Queen Street, 472 3510 **(existing patients 389 3808 Wainuiomata Capital Dental The only) Ground Floor, Montreaux Adrian Tong Raine Street Dental, 4 Wellington CityWellington Terrace 939 9917 Building, 164 The Terrace 476 7295 Raine Street 499 9360 Karori Lumino Dental 180 Stokes Valley Road, Karori Dental 939 1818 Stokes Valley Dental Awareness Level 1, 9 Marion Street Centre 146 Karori Road 385 4386 Ashwin Magan 476 6451 Level 3, 84-90 Main Street Earle Kirton Harbour City Tower, 29 527 7914 Singleton Dental 473 7632 Brandon Street 294A Karori Road Christopher Allan 476 6252 U UUUU 22 Royal Street Irina Kvatch Central Dental Surgery, 139 Upper Hutt 528 5302 CODE Dental 220 Main Road 472 6306 Featherston Street Art of Dentistry 10 Royal Street 232 8001 Tawa 527 9437 Joanna Ora Toa Medical Hodgkinson Level 1, 90 The Terrace Michael Walton Centre 178 Bedford Street 22 Royal Street 472 3510 528 5302 237 5152 Navin Vithal Tennyson Dental Centre, Porirua Lumino Silverstream Village Shop The Dental Centre 801 6228 32 Lorne Street, Te Aro Silverstream 14/Cnr Whitemans Rd & Porirua 4 Lydney Place Peter Scott 528 3984 Kiln St 29 Brandon Street 237 6148 473 7632 Walter Szeto -

School Boy Vandalism in the Hutt Valley
SCHOOL BOY VANDALISM IN THE HUTT VALLEY PRELIMINARY ANALYSIS Occasional Papers in Criminology No. 8 ISSN 0110-1773 Michael Stace Institute of Criminology Victoria University of Wellington ' CON'l':t:N'l'8 Page Foreword L The Research Project Planning 1 Summary R 2. Preliminary Analysis A. Introduction 10 B. The Most Frequently Admitted Acts 12 C. Seriousness 18 D. Police Youth Aid Statistics 20 E • Summary 2 2 References 24 Appendix A 25 Appendix B 28 .FOREWORD An earlier Occasional Paper, namely Noc 6, February 1978, was written by Mr Michael Stace of this Institute on the subject of Vandalism and Self RepoEt Studies : A Review of the Literature. ':rhe present paper by Mr Stace gives some of the results from a questionnaire administered in four New Zealand post-primary schools, namely, the Hutt Valley High School, the Hutt Valley Memorial Technical College, Naenae College, and Taita College. We are 1m'.!eLted to Mr W. RAnwick, Director-General of Education tor the help and encouragement he and his senior officers 1;:rave to the launching of the project. We thank Mr E. Flaws, the Principal of Tawa College and Mr A. McLean, School Counsellor, for their helpful reception and adoption of the proposal that a pilot scheme be administered at Tawa College. We are also appreciative of the reception and support later given by the following principals of the four post-primary schools in the Hutt Valley and also the school counsellors as set out below;- School Principal Guidance Counsellor Hutt Valley High School M.r I. R. McLean Mr B.C. -

Hutt/Girls Zone Athletics
Newtown Park Stadium - Site License Hy-Tek's MEET MANAGER 6:14 AM 12/03/2021 Page 1 Hutt & Girls Zone Combined Athletics 2021 - 11/03/2021 Newtown Park Stadium, Wellimgton Results Event 114 Boys 100 Meter Run Junior Hutt Record: 11.28 2006 J Smith, Hutt International Name Age Team Finals Wind H# Finals 1 Austin-Aschebrock, Kaan Hutt Valley High School 12.91 -0.2 2 2 Foley, Lynkon Taita College 13.05 -0.2 2 3 Montgomery, Teina St Bernard's College 13.08 -0.2 2 4 Toluono, Lawrence St Bernard's College 13.44 -0.9 1 5 Reddy, Dishab Hutt Valley High School 13.47 -0.9 1 6 Zaballa, Inaki Hutt Valley High School 13.50 -0.9 1 7 Gonzalez Delgado, Jerson Naenae College 13.85 -0.2 2 8 Maligi-Masoe, Leo Naenae College 13.88 -0.9 1 9 West, Noah Hutt International Boys' 14.05 -0.2 2 10 Sheterline, Hamish Upper Hutt College 14.11 -0.2 2 11 Jacobs, James Hutt Valley High School 14.12 -0.9 1 12 Hickson, Oliver Hutt International Boys' 14.74 -0.9 1 Event 116 Boys 100 Meter Run Intermediate Hutt Record: 11.13 1991 R Morrell, Upper Hutt Name Age Team Finals Wind H# Finals 1 Moody, Tyrus Naenae College 12.14 1.1 3 2 Maluschnig, Ben St Bernard's College 12.16 1.1 2 3 Ranginui, Tamihana St Bernard's College 12.36 -0.9 1 4 Samuelu, Sam Naenae College 12.44 1.1 2 5 Urwin, Eli Heretaunga College 12.55 1.1 2 6 Foaese, Petonio Taita College 12.60 1.1 2 7 Haines, Rhone Heretaunga College 12.65 1.1 3 8 Baker, Matenga Naenae College 12.66 -0.9 1 9 Holden, Monty Hutt International Boys' 12.72 1.1 2 10 Bissielo, Eden Upper Hutt College 12.80 1.1 3 11 Armstrong, Luke Hutt -

Hutt Zone Athletics 2017 - 10/03/2017 Newtown Stadium Results
Newtown Park, Wellington - Site License Hy-Tek's MEET MANAGER 4:44 PM 10/03/2017 Page 1 Hutt Zone Athletics 2017 - 10/03/2017 Newtown Stadium Results Girls 100 Metre Run Junior Record: 12.50 R S Garden, Parkway Name Age Team Seed Finals Wind H# Points Finals 1 Foley, Stani Taita College 14.30 -0.7 3 5 2 Masson, Naomi Heretaunga College 14.34 -0.7 3 4 3 Vole, Ebony-Shavaugh Wainuiomata High School 14.78 -0.7 3 3 4 De Silva, Imali Hutt Valley High School 14.94 -1.6 1 2 5 McPartlin, Mikayla Heretaunga College 15.06 -2.1 2 1 6 Morresey, Camryn Hutt Valley High School 15.09 -0.7 3 7 McKean, Brooklyn Naenae College 15.39 -2.1 2 8 McQueen, Zoe Hutt Valley High School 15.44 -2.1 2 9 Jeffries-Rua, Jamiee Upper Hutt College 15.50 -2.1 2 10 Carter, Shanti Hutt Valley High School 15.66 -1.6 1 11 Pepere, Tiari Upper Hutt College 15.69 -0.7 3 12 Holland, Naomi Wa Ora Montessori School 15.98 -0.7 3 13 Leuila, Teila Taita College 16.07 -1.6 1 14 Arunkumar, Neha Wa Ora Montessori School 16.48 -2.1 2 15 Strickland, Una Wa Ora Montessori School 16.65 -1.6 1 Girls 200 Metre Run Junior Record: 26.50 R 1990 T Ioata, Naenae Name Age Team Seed Finals Wind H# Points Finals 1 Toa, Tamzin Wainuiomata High School 30.42 0.3 2 5 2 De Silva, Imali Hutt Valley High School 30.82 0.2 1 4 3 Keating, Hannah Hutt Valley High School 30.83 0.2 1 3 4 Vole, Ebony-Shavaugh Wainuiomata High School 30.94 1.0 3 2 5 Greville, Iona Heretaunga College 31.49 1.0 3 1 6 Morresey, Camryn Hutt Valley High School 31.78 1.0 3 7 Ioata, Destiny Naenae College 31.97 1.0 3 8 Esbach, Shaa-iqah -
Spaces for Hire
SPACES FOR HIRE A LIST OF SPACES FOR HIRE IN LOWER HUTT SPACES FOR HIRE CONTENTS ALICETOWN ........................................................................................................................................... 5 Transition Towns Community Centre ........................................................................................................... 5 AVALON.................................................................................................................................................. 5 Avalon Pavilion ............................................................................................................................................. 5 Avalon Public Hall ........................................................................................................................................ 6 Hutt Bridge Club ........................................................................................................................................... 6 St. John’s Avalon Uniting Church ................................................................................................................. 7 Ricoh Sports Centre ..................................................................................................................................... 7 BELMONT ............................................................................................................................................... 8 Belmont Memorial Hall (Belmont Domain) .................................................................................................. -

Regional Community Profile
Regional community profile: Wellington Community Trust October 2020 Contents 1. Summary of Findings 3 2. Background 5 2.1 Indicator data 6 2.2 Interpreting the indicator data tables in this report 7 3. Indicator Data 8 3.1 Population 8 3.2 Socio-economic deprivation 13 3.3 Employment and income 16 3.4 Education 17 3.5 Housing 19 3.6 Children and young people 21 3.7 Community wellbeing 23 3.8 Environment 25 References 26 Centre for Social Impact | Wellington Community Trust – Community Profile September 2020 | Page 2 1. Summary of Findings Population and projections (2018 Census) ● Population: The WCT region is home to around 469,047 people, or 9.8% of New Zealand’s population. It has five territorial authority areas. Two thirds of the people in the WCT region reside in two of these five areas – Wellington City (45%) and Lower Hutt City (22%). Porirua has 12% of the WCT population, followed by 11% in Kapiti Coast District and 9% in Upper Hutt City. ● Population projection: The WCT region’s population will increase by 11% by 2038. Projected population growth in the region is lower than the projected New Zealand average (20%). This means that by 2038, the WCT region is projected to represent a slightly reduced 9.0% of New Zealand’s population. ● Ethnicity: Porirua (22%) and Lower Hutt (10%) have populations with the highest proportion of Pacific Peoples in the WCT region. Both areas also have the populations with the highest proportion of Māori (18% and 16% respectively). Population projections show that Māori and Pacific communities will grow further in proportion in these two areas by 2038. -

Wellington Region
FRUIT & VEGE CO-OP WELLINGTON REGION Wellington Region Fruit & Vege Co-ops Kapiti: Paraparaumu, Raumati Newtown: Miramar, Berhampore, Strathmore, Hataitai Kapiti Fruit and Vege Co-op Newtown Fruit and Vege Co-op St Paul’s Kapiti Anglican Coordinator: Christine 027 354 0125 St Aidan’s Church Coordinator: Meri 027 396 9943 [email protected] [email protected] Salvation Army Kapiti Office: 04 297 1436 Raukawa Community Centre Coordinator: Fiona 022 506 2288 [email protected] [email protected] Raumati Uniting Church Office: 04 902 5809 Granville Flats [email protected] Centennial Flats Rintoul Street Flats Naenae: Taita, Pomare, Stokes Valley, Kelson Coordinator: Bruce 027 275 6041 [email protected] Naenae Fruit and Vege Co-op St David’s Church Hall Haitaitai Community House Coordinator: Eliza 027 278 1176 [email protected] [email protected] Salvation Army Worship and Community Centre St Mattew’s Anglican Church Hall Coordinator: Turi 04 389 0594 Coordinator: Anna 022 060 9533 [email protected] [email protected] Petone Pomare Taita Community Trust Coordinator: Jasmine 04 939 8345 Petone Fruit and Vege Co-op [email protected] Petone Baptist Church Coordinator: Emma 027 305 7002 St Phillip’s Stone Church [email protected] Coordinator: Adrienne 021 136 1890 [email protected] Discovery Elim Christian Centre Coordinator: Rachel 021 802 761 [email protected] Porirua: