Recovery of Survivors of Improvised Explosive Devices and Explosive Remnants of War in Northeast Syria
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Carnivores of Syria 229 Doi: 10.3897/Zookeys.31.170 RESEARCH ARTICLE Launched to Accelerate Biodiversity Research
A peer-reviewed open-access journal ZooKeys 31: 229–252 (2009) Carnivores of Syria 229 doi: 10.3897/zookeys.31.170 RESEARCH ARTICLE www.pensoftonline.net/zookeys Launched to accelerate biodiversity research Carnivores of Syria Marco Masseti Department of Evolutionistic Biology “Leo Pardi” of the University of Florence, Italy Corresponding author: Marco Masseti (marco.masseti@unifi .it) Academic editors: E. Neubert, Z. Amr | Received 14 April 2009 | Accepted 29 July 2009 | Published 28 December 2009 Citation: Masseti, M (2009) Carnivores of Syria. In: Neubert E, Amr Z, Taiti S, Gümüs B (Eds) Animal Biodiversity in the Middle East. Proceedings of the First Middle Eastern Biodiversity Congress, Aqaba, Jordan, 20–23 October 2008. ZooKeys 31: 229–252. doi: 10.3897/zookeys.31.170 Abstract Th e aim of this research is to outline the local occurrence and recent distribution of carnivores in Syria (Syrian Arab Republic) in order to off er a starting point for future studies. The species of large dimensions, such as the Asiatic lion, the Caspian tiger, the Asiatic cheetah, and the Syrian brown bear, became extinct in historical times, the last leopard being reputed to have been killed in 1963 on the Alauwit Mountains (Al Nusyriain Mountains). Th e checklist of the extant Syrian carnivores amounts to 15 species, which are essentially referable to 4 canids, 5 mustelids, 4 felids – the sand cat having been reported only recently for the fi rst time – one hyaenid, and one herpestid. Th e occurrence of the Blandford fox has yet to be con- fi rmed. Th is paper is almost entirely the result of a series of fi eld surveys carried out by the author mainly between 1989 and 1995, integrated by data from several subsequent reports and sightings by other authors. -

Deir Ez-Zor: Dozens Arbitrarily Arrested During SDF's “Deterrence
Deir ez-Zor: Dozens Arbitrarily Arrested during SDF’s “Deterrence of Terrorism” Campaign www.stj-sy.org Deir ez-Zor: Dozens Arbitrarily Arrested during SDF’s “Deterrence of Terrorism” Campaign This joint report is brought by Justice For Life (JFL) and Syrians for Truth and Justice (STJ) Page | 2 Deir ez-Zor: Dozens Arbitrarily Arrested during SDF’s “Deterrence of Terrorism” Campaign www.stj-sy.org 1. Executive Summary The Syrian Democratic Forces (SDF) embarked on numerous raids and arrested dozens of people in its control areas in Deir ez-Zor province, located east of the Euphrates River, during the “Deterrence of Terrorism” campaign it first launched on 4 June 2020 against the cells of the Islamic State (IS), aka Daesh. The reported raids and arrests were spearheaded by the security services of the Autonomous Administration and the SDF, particularly by the Anti-Terror Forces, known as the HAT.1 Some of these raids were covered by helicopters of the US-led coalition, eyewitnesses claimed. In the wake of the campaign’s first stage, the SDF announced that it arrested and detained 110 persons on the charge of belonging to IS, in a statement made on 10 June 2020,2 adding that it also swept large-scale areas in the suburbs of Deir ez-Zor and al-Hasakah provinces. It also arrested and detained other 31 persons during the campaign’s second stage, according to the corresponding statement made on 21 July 2020 that reported the outcomes of the 4- day operation in rural Deir ez-Zor.3 “At the end of the [campaign’s] second stage, the participant forces managed to achieve the planned goals,” the SDF said, pointing out that it arrested 31 terrorists and suspects, one of whom it described as a high-ranking IS commander. -

S/2019/321 Security Council
United Nations S/2019/321 Security Council Distr.: General 16 April 2019 Original: English Implementation of Security Council resolutions 2139 (2014), 2165 (2014), 2191 (2014), 2258 (2015), 2332 (2016), 2393 (2017), 2401 (2018) and 2449 (2018) Report of the Secretary-General I. Introduction 1. The present report is the sixtieth submitted pursuant to paragraph 17 of Security Council resolution 2139 (2014), paragraph 10 of resolution 2165 (2014), paragraph 5 of resolution 2191 (2014), paragraph 5 of resolution 2258 (2015), paragraph 5 of resolution 2332 (2016), paragraph 6 of resolution 2393 (2017),paragraph 12 of resolution 2401 (2018) and paragraph 6 of resolution 2449 (2018), in the last of which the Council requested the Secretary-General to provide a report at least every 60 days, on the implementation of the resolutions by all parties to the conflict in the Syrian Arab Republic. 2. The information contained herein is based on data available to agencies of the United Nations system and obtained from the Government of the Syrian Arab Republic and other relevant sources. Data from agencies of the United Nations system on their humanitarian deliveries have been reported for February and March 2019. II. Major developments Box 1 Key points: February and March 2019 1. Large numbers of civilians were reportedly killed and injured in Baghuz and surrounding areas in south-eastern Dayr al-Zawr Governorate as a result of air strikes and intense fighting between the Syrian Democratic Forces and Islamic State in Iraq and the Levant. From 4 December 2018 through the end of March 2019, more than 63,500 people were displaced out of the area to the Hawl camp in Hasakah Governorate. -

Week 46, 10 – 16 November 2017
Week 46, 10 – 16 November 2017 General developments & political & security situation • US-led Coalition’s air force killed civilians and some paramedics in Tal Ash-Shayer area of Al-Duaiji village in rural Deir Ez-Zor, on the Syrian-Iraqi border. • Russian and US Presidents affirmed their commitment to Syria’s sovereignty, independence and territorial integrity; stressing that political settlement of the crisis would take place within framework of the Geneva process - in a joint statement issued on sidelines of the APEC summit in Vietnam. • Trump says U.S. deal with Russia on Syria will save many lives. • Moscow: Conclusions of the report of the UN-OPCW Joint Investigative Mission (JIM) on allegations of Syrian government's use of sarin gas had no basis. • Russian Defense: Russian experts are contributing to clearance of mines, left behind by ISIS, in Abu Kamal. • Zakharova: Syria's national dialogue conference is under preparation. • Algerian Prime Minister stressed that some countries in the region spent $ 130 billion to destroy Syria, Libya and Yemen. • Chinese Ambassador in Damascus stressed that a Syrian-Syrian dialogue, that guaranteed political solution, was the only way to end the crisis. • The United States has no plans to carry out military patrolling in Syria's de-escalation zones, US Defense Secretary Jim Mattis said. • The Syrian army, with support from the Russian Aerospace Forces, has recently retaken the city of Abu Kemal, the last ISIS stronghold in the eastern Syrian governorate of Deir Ezzor. • ISIS militants regained control of Abu Kemal, their last stronghold in Syria, after Iranian-backed militias who claimed to have captured the city a few days earlier. -

UNHCR's Operational Update: January-March 2019, English
OPERATIONAL UPDATE Syria January -March 2019 As of end of March, UNHCR In February, UNHCR participated in Since December a major emergency concluded its winterization the largest ever humanitarian in North East Syria led to thousands of programme with the distribution convoy providing life-saving people fleeing Hajin to Al-Hol camp. of 1,553,188 winterized humanitarian assistance to some UNHCR is providing core relief items to 1,163,494 individuals/ 40,000 displaced people at the items, shelter and protection 241,870 families in 13 governorates in Rukban ‘makeshift’ settlement in support for the current population Syria. south-eastern Syria, on the border which exceeds 73,000 individuals. with Jordan. HUMANITARIAN SNAPSHOT 11.7 million FUNDING (AS OF 16 APRIL 2019) people in need of humanitarian assistance USD 624.4 million requested for the Syria Operation 13.2 million Funded 14% people in need of protection interventions 87.4 million 11.3 million people in need of health assistance 4.7 million people in need of shelter Unfunded 86% 4.4 million 537 million people in need of core relief items POPULATION OF CONCERN Internally Displaced Persons Internally displaced persons 6.2 million Returnees Syrian displaced returnees 2018 1.4 million* Syrian refugee returnees 2018 56,047** Syrian refugee returnees 2019 21,575*** Refugees and Asylum seekers Current population 32,289**** Total urban refugees 17,832 Total asylum seekers 14,457 Camp population 30,529***** High Commissioner meets with families in Souran in Rural * OCHA, December 2018 Hama that have returned to their homes and received shelter ** UNHCR, December 2018 *** UNHCR, March 2019 assistance from UNHCR. -
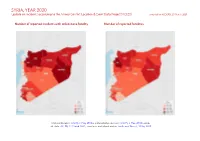
SYRIA, YEAR 2020: Update on Incidents According to the Armed Conflict Location & Event Data Project (ACLED) Compiled by ACCORD, 25 March 2021
SYRIA, YEAR 2020: Update on incidents according to the Armed Conflict Location & Event Data Project (ACLED) compiled by ACCORD, 25 March 2021 Number of reported incidents with at least one fatality Number of reported fatalities National borders: GADM, 6 May 2018a; administrative divisions: GADM, 6 May 2018b; incid- ent data: ACLED, 12 March 2021; coastlines and inland waters: Smith and Wessel, 1 May 2015 SYRIA, YEAR 2020: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 25 MARCH 2021 Contents Conflict incidents by category Number of Number of reported fatalities 1 Number of Number of Category incidents with at incidents fatalities Number of reported incidents with at least one fatality 1 least one fatality Explosions / Remote Conflict incidents by category 2 6187 930 2751 violence Development of conflict incidents from 2017 to 2020 2 Battles 2465 1111 4206 Strategic developments 1517 2 2 Methodology 3 Violence against civilians 1389 760 997 Conflict incidents per province 4 Protests 449 2 4 Riots 55 4 15 Localization of conflict incidents 4 Total 12062 2809 7975 Disclaimer 9 This table is based on data from ACLED (datasets used: ACLED, 12 March 2021). Development of conflict incidents from 2017 to 2020 This graph is based on data from ACLED (datasets used: ACLED, 12 March 2021). 2 SYRIA, YEAR 2020: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 25 MARCH 2021 Methodology GADM. Incidents that could not be located are ignored. The numbers included in this overview might therefore differ from the original ACLED data. -

Spotlight on Global Jihad (February 27 – March 4, 2020)
( רמה כ ז מל ו תשר מה ו ד י ע י ן ( למ מ"ל ןיעידומ כרמ ז מה י עד מל ו ד י ע י ן ו רטל ו ר ט ןיעידומ ע ה ר Spotlight on Global Jihad February 27 – March 4, 2020 Highlights of the events This week, high-intensity battles took place in the Idlib region between the Syrian army and the forces supporting it (including the Lebanese Hezbollah) and the Headquarters for the Liberation of Al-Sham and the other rebel organizations. The battles centered on two areas. In the northeastern Idlib region, the rebel organizations managed to retake the city of Saraqeb (the most significant achievement to date). However, three days later, the Syrian army retook the city and the surrounding rural area (relatively easily) and regained control of the M-5 highway (the Damascus-Aleppo highway). At the same time, battles took place in the southern Idlib region. Both sides recorded local successes, but the general trend is to continue “gnawing away” at the areas controlled by the rebel organizations. Against the backdrop of the intensive fighting in the Idlib region, clashes between the Syrian army and the Turkish army escalated this week. On February 27, 2020, 33 Turkish soldiers were killed in a Syrian airstrike. In response, the Turkish army carried out extensive attacks against Syrian targets. Following the killing of the Turkish soldiers, the Turkish defense minister announced the start of Operation Spring Shield, a military operation against the Syrian army. Turkish President Erdoğan stressed that the operation was directed against targets of the Syrian regime and that Turkey was not targeting Russia and Iran. -

Spotlight on Global Jihad (May 6-12, 2021)
( רמה כ ז מל ו תשר מה ו ד י ע י ן ( למ מ"ל ןיעידומ ש ל מ כרמ ז מה י עד מל ו ד י ע י ן ו רטל ו ר ט ןיעידומ ע ה ר ( רמה כ ז מל ו תשר מה ו ד י ע י ן ( למ מ"ל ןיעידומ ש ל מ כרמ ז מה י עד מל ו ד י ע י ן ו רטל ו ר ט ןיעידומ ע ה ר Spotlight on Global Jihad May 6-12, 2021 Main events of the past week The fourth week of Ramadan was also marked by a relatively high number of attacks, mainly in Iraq and Africa. Syria: An IED was activated against a Syrian army ATV in the desert region (Al-Badia). The vehicle was destroyed and the passengers were killed or wounded. ISIS’s activity against the Kurdish SDF forces continued in the Deir ez-Zor-Al-Mayadeen region and in the Al-Raqqah region, where there was an increase in activity this week. Southern Syria: ISIS continued its activity against the Syrian army. This week, a soldier was targeted by gunfire in Naba al- Fawar, west of Daraa. He was killed. Iraq: The week, ISIS concentrated its activity mainly in the Kirkuk Province, where its operatives carried out several attacks against camps of the Iraqi security forces. ISIS operatives also blew up two oil wells in the area of Bai Hassan, northwest of Kirkuk, as part of the its so-called economic war. Africa: There appears to have been a slight decrease in ISIS’s activity this week. -

Annual Report on Civilian Casualties in Connection with United States Military Operations in 2019
UNCLASSIFIED Department of Defense Annual Report on Civilian Casualties In Connection With United States Military Operations in 2019 Submitted pursuant to Section 1057 of the National Defense Authorization Act for Fiscal Year 2018 (Public Law 115-91), as amended The estimated cost of this report for the Department of Defense is approximately $20,000 for the 2020 Fiscal Year. This includes $25 in expenses and $20,000 in DoD labor. Generated on 2020April22 A-60DF323 1 UNCLASSIFIED Section 1057 of the National Defense Authorization Act for Fiscal Year 2018 (Public Law 115- 91), as amended, states the following: Annual Report on Civilian Casualties in Connection With United States Military Operations (a) ANNUAL REPORT REQUIRED.—Not later than May 1 each year, the Secretary of Defense shall submit to the congressional defense committees a report on civilian casualties caused as a result of United States military operations during the preceding year. (b) ELEMENTS.—Each report under subsection (a) shall set forth the following: (1) A list of all the United States military operations, including each specific mission, strike, engagement, raid, or incident, during the year covered by such report that were confirmed, or reasonably suspected, to have resulted in civilian casualties. (2) For each military operation listed pursuant to paragraph (1), each of the following: (A) The date. (B) The location. (C) An identification of whether the operation occurred inside or outside of a declared theater of active armed conflict. (D) The type of operation. (E) An assessment of the number of civilian and enemy combatant casualties, including a differentiation between those killed and those injured. -

Deir Ezzor … Detention and Extortion of Civilians, and Oil Smuggling
Deir Ezzor … Detention and Extortion of Civilians, and Oil Smuggling Brief Report on Latest Updates in Some Deir Ezzor Areas Justice for Life Organization April 2019 Despite the control of Syrian government forces and Syria Democratic Forces over the entire province of Deir Ezzor after driving ISIS out, yet the civilians are still suffering from multiple problems as these forces are still committing violations against the civilians including detention, torture, and humiliation. The province is divided into two parts in terms of controlling power; the Syria government forces, supporting and affiliated militias along with foreign forces are controlling the cities, towns, and villages that are located in the south of Euphrates River, whereas the Syria Democratic Forces, with support of the US-led international coalition, control the areas located in the north of the river. This present report covers the latest developments in the two parts of Deir Ezzor in terms of the existing military powers, most prominent violations, fears of civilians, returning of IDPs, and the provided services. This report focuses on the cities of Deir Ezzor and Al Mayadin, in the south of the river, along with Al Kasra sub-district, the villages of Gharaneej, Al Kishkia, and Abu Hamam, in the north of the river. First: Syrian Government Forces Held Areas: 1- Deir Ezzor City It became a densely population city following the returning of hundreds of families towards the not destroyed neighborhoods such as Al Joura, Al Qusour, and Harabesh. The major reasons behind their returning to the city were the expensive rents, extortion practiced either by government forces, SDF, or opposition groups, and lack of humanitarian aid provided to them. -

Deir-Ez-Zor: Situation Overview and Sub-District Profiles Syria, June 2018
Deir-ez-Zor: Situation Overview and Sub-district Profiles Syria, June 2018 Background Methodology Since mid-2017, ongoing conflict has led to displacement from and within Overall, 112 locations in Deir-ez-Zor governorate were assessed between 4 and 11 Deir-ez-Zor governorate, totalling an estimated 230,000 persons from July to mid- June 2018 through remote Key Informant (KI) interviews, with a minimum of three December.1 While there had been de-escalation in some parts of the governorate KIs per assessed community and one KI per informal site. Different tools were in early 2018, renewed sustained conflict and related violence between Syrian used to assess communities and informal sites to identify population estimates Democratic Forces (SDF) and the group known as Islamic State of Iraq and the and multi-sectoral needs. Levant (ISIL) as well as sporadic clashes between SDF and Government of Syria Whilst efforts were made to cover as many locations as possible, assessed sites (GoS) are precipitating further displacement and exacerbating already-severe and communities were selected on the basis of their accessibility and should humanitarian conditions. Following previous assessments in February and April not be considered as a fully comprehensive list. Information should only be 2018, REACH recently conducted another rapid needs assessment to address considered as relevant to the time of data collection, given the dynamic situation information gaps and to provide an overview of the location and humanitarian in the governorate. Findings are not statistically representative and should be situation of different population groups. Assessed locations are clustered along considered as indicative only, particularly as they are aggregated across locations three main transects of the Euphrates and Khabour river (see Map 1). -

S/PV.8715 the Situation in the Middle East 06/02/2020
United Nations S/ PV.8715 Security Council Provisional Seventy-fifth year 8715th meeting Thursday, 6 February 2020, 3 p.m. New York President: Mr. Pecsteen de Buytswerve ....................... (Belgium) Members: China ......................................... Mr. Wu Haitao Dominican Republic ............................. Mr. Singer Weisinger Estonia ........................................ Mr. Jürgenson France ........................................ Mr. De Rivière Germany ...................................... Mr. Heusgen Indonesia. Mr. Soemirat Niger ......................................... Mr. Aougi Russian Federation ............................... Mr. Nebenzia Saint Vincent and the Grenadines ................... Ms. King South Africa ................................... Mr. Van Shalkwyk Tunisia ........................................ Mr. Zenati United Kingdom of Great Britain and Northern Ireland .. Ms. Pierce United States of America .......................... Mrs. Craft Viet Nam ...................................... Mr. Pham Agenda The situation in the Middle East This record contains the text of speeches delivered in English and of the translation of speeches delivered in other languages. The final text will be printed in the Official Records of the Security Council. Corrections should be submitted to the original languages only. They should be incorporated in a copy of the record and sent under the signature of a member of the delegation concerned to the Chief of the Verbatim Reporting Service, room U-0506 ([email protected]). Corrected records will be reissued electronically on the Official Document System of the United Nations (http://documents.un.org). 20-03035 (E) *2003035* S/PV.8715 The situation in the Middle East 06/02/2020 The meeting was called to order at 3.05 p.m. whose population has fled from earlier attacks. Maarat Al-Numan lies on the strategic M5 highway. Pro- Adoption of the agenda Government forces have continued to push north, reaching the city of Saraqib, the junction of the M4 and The agenda was adopted.