Automobile Liability (Including Pollution Coverage) Application
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mail and Reproduction Management Division
MAIL AND REPRODUCTION MANAGEMENT DIVISION USERS GUIDE TO SERVICES This guidebook is provided to all user agencies throughout the USDA Washington Headquarters complex as a quick desk reference for all major services that are regularly made available by the Mail and Reproduction Management Division (MRMD) of the Office of Operations. A telephone number is listed for each service. For assistance in using any service, please call the indicated number. The Mail and Reproduction Management Division constantly strives to meet customer expectations and to improve basic service for all of its users. We welcome all suggestions on the improvement or expansion of our services. SECTION 1 – MAIL SERVICES REQUIRED MAILING PRACTICES……………………………………………………1 COST SAVING MAILING TIPS………...………………………………………………3 MAIL DISTRIBUTION………………………………………………………………...3-4 Services include door-to-door, late, bulk mail pick-up services, mail drop updates. U.S. POSTAL SERVICE SPECIAL SERVICES………………………………………5-7 Express Mail Certified Mail Registered Mail Return Receipts Delivery Confirmation Insured Special Delivery DEPARTMENTAL MAILING LIST SECTION…………………………………………8 Printing of mailing labels, correction of addresses, and creation of new lists. In addition, use of a high-speed laser printer to receive reports from NFC. COURIER SERVICE UNIT…………………………………………………………..9-10 Pick-up and delivery of packages within the Washington Metropolitan area. MAIL PREPARATION UNIT…………………………………………………………..11 Preparation of mail, including labeling, inserting, sealing, and bulk wrapping. MAIL STOP -
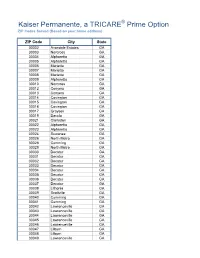
KP-TRICARE-Zip-Codes.Pdf
Kaiser Permanente, a TRICARE® Prime Option ZIP Codes Served (Based on your home address) ZIP Code City State 30002 Avondale Estates GA 30003 Norcross GA 30004 Alpharetta GA 30005 Alpharetta GA 30006 Marietta GA 30007 Marietta GA 30008 Marietta GA 30009 Alpharetta GA 30010 Norcross GA 30012 Conyers GA 30013 Conyers GA 30014 Covington GA 30015 Covington GA 30016 Covington GA 30017 Grayson GA 30019 Dacula GA 30021 Clarkston GA 30022 Alpharetta GA 30023 Alpharetta GA 30024 Suwanee GA 30026 North Metro GA 30028 Cumming GA 30029 North Metro GA 30030 Decatur GA 30031 Decatur GA 30032 Decatur GA 30033 Decatur GA 30034 Decatur GA 30035 Decatur GA 30036 Decatur GA 30037 Decatur GA 30038 Lithonia GA 30039 Snellville GA 30040 Cumming GA 30041 Cumming GA 30042 Lawrenceville GA 30043 Lawrenceville GA 30044 Lawrenceville GA 30045 Lawrenceville GA 30046 Lawrenceville GA 30047 Lilburn GA 30048 Lilburn GA 30049 Lawrenceville GA Kaiser Permanente, a TRICARE® Prime Option ZIP Codes Served (Based on your home address) ZIP Code City State 30054 Oxford GA 30058 Lithonia GA 30060 Marietta GA 30061 Marietta GA 30062 Marietta GA 30063 Marietta GA 30064 Marietta GA 30065 Marietta GA 30066 Marietta GA 30067 Marietta GA 30068 Marietta GA 30069 Marietta GA 30070 Porterdale GA 30071 Norcross GA 30072 Pine Lake GA 30074 Redan GA 30075 Roswell GA 30076 Roswell GA 30077 Roswell GA 30078 Snellville GA 30079 Scottdale GA 30080 Smyrna GA 30081 Smyrna GA 30082 Smyrna GA 30083 Stone Mountain GA 30084 Tucker GA 30085 Tucker GA 30086 Stone Mountain GA 30087 Stone Mountain GA -
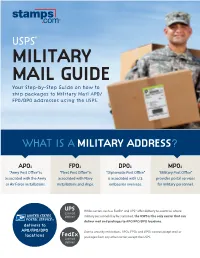
Your Step-By-Step Guide on How to Ship Packages to Military Mail APO/ FPO/DPO Addresses Using the USPS
USPS® MILITARY MAIL GUIDE Your Step-by-Step Guide on how to ship packages to Military Mail APO/ FPO/DPO addresses using the USPS. WHAT IS A MILITARY ADDRESS? APO: FPO: DPO: MPO: “Army Post Office” is “Fleet Post Office” is “Diplomatic Post Office” “Military Post Office” associated with the Army associated with Navy is associated with U.S. provides postal services or Air Force installations. installations and ships. embassies overseas. for military personnel. UPS While carriers such as FedEx® and UPS® offer delivery to countries where cannot deliver military personnel may be stationed, the USPS is the only carrier that can deliver mail and packages to APO/FPO/DPO locations. delivers to APO/FPO/DPO Due to security restrictions, APOs, FPOs and DPOs cannot accept mail or locations FedEx cannot packages from any other carrier, except the USPS. deliver HOW TO ADDRESS A SHIPPING LABEL FOR AN APO/FPO/DPO PACKAGE 2 INCLUDE THE UNIT AND BOX NUMBER Army: Unit [Number] Box [Number] Air Force: PSC* [Number] Box [Number] 1 NAME OF THE RECIPIENT Rank/grade/rating is optional Navy: Ship [Number] Hull [Number] for APO or FPO. Do not include 5 ZIP CODE recipient’s title for DPO. Embassy: Unit [Number] Box [Number] 3 CITY 4 STATE APO, FPO or DPO AA (Armed Forces Americas) AE (Armed Forces Europe) AP (Armed Forces Pacific) 1 Enter the full name of the addressee. Mail addressed to ‘Any Service Member’ or similar wording such as ‘Any CORRECT FORMAT WRONG FORMAT Soldier, Sailor, Airman or Marine’ is prohibited. Mail must CPT John Doe CPT John Doe be addressed to an individual name or job title, such as Unit 45013 Box 2666 USAG J Box 2666 ‘Sergeant’ or ‘Private First Class.’ USAG J APO AP 96338 APO AP 96338 2 Enter the unit or Post Office box number. -

Post Office Department Records MORE DESCRIPTIONS ADDED
National Archives Across the Nation Post Office Department Records MORE DESCRIPTIONS ADDED by Claire Prechtel-Kluskens AS A PART OF THE NATIONAL ARCHIVES AND RECORDS ADMINISTRATION’S (NARA) ongoing mission to provide greater access to the records in its custody, staff at the National Archives Building in Washington, DC, continue to add descriptions for record series in Record Group 28, Records of the Post Office Department, to the online National Archives Catalog at http://www.archives.gov/research/catalog/. Listed below are 133 newly described re- • Construction and Engineering Project Lists, 6/16/1958–2/11/1959. NAID cord series from this record group (RG). Re- Files, 1965–1968. NAID 12021476. 12021601. searchers can learn more information about • Copies of Letters Sent Regarding • General Orders and Pay Summary these records by searching for the title or Closed Railway Mail Service Cases, Forms for Boston, Massachusetts, 1882– the National Archives Identifier (NAID). 1924–1929. NAID 16411671. 1887. NAID 16608021. Researchers interested in postal history, lo- • Correspondence Files Relating to • General Research Project 10 Regional cal history, governmental operations, and International Postal Matters, 1917–1961. Final Reports, 1/1956–4/1956. NAID genealogy may find these records useful. NAID 16562999. 12021534. • Administrative Manual and Related • Correspondence of Winton M. Blount, • Highway Post Office Discontinuance Records, 1950–1955. NAID 12021493. 1969–1970. NAID 12012278. Case Files, 1961–1967. NAID 12021640. • Advertisements and Proposals for Mail • Correspondence Regarding the • Indexes and Lists Concerning Mail Contracts, 1808–1961. NAID 12023189. Bituminous Coal Conservation Act of Depredations, 1845–1848. NAID 12019914. • Agreements with Railroad Companies, 1935, 1935–1937. -

Maryland Zip Code
(! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! !( (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! ! (! ( ! ! ( (! ( !( (! (! (! ! (! ! ( (! ( (! ! ! (! ( (! ( (! ! (! ( (! (! (! (! (! (! (! ! (! ( (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! ! ! ( ( ! (! ( (! ! (! (! ( (! (! ! (! (! ( ! (! ! ( (! (! ( (! ! (! (! ( (! (! (! (! (! ! (! ( ! (! ( ! ! (! ( ( (! (! (! (! ! (! ( (! ! ( (! (! (! (! (! !( ! (! ( ! ! ( (! ( (! (! (! (! (! ! ( (! ! ( (! (! (! (! (! (! (! ! (! ( (! (! (! (! (! (! (! ! (! ( (! (! ! ( ! ! (! ( ( (! (! ! ( (! ! (! (! ( (! ! ! ( (! ( (! (! (! (! (! (! (! (! (! (! !( ! ! ( ( (! (! (! ! (! (! ( (! ! (! (! ( (! (! !( (! (! !( (! !( (! (! (! (! ! ! !( ( ( (! (! ! (! ( ! (! ! ( (! (! ( (! (! (! (! (! (! !( ! (! ! ( (! (! (! ! ( (! (! ( (! (! (! ! ! (! ( ( ! ! (! ( ( (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! ! ! (! (! (! (! ( (! ( ! ! ( ! (! ( (! ! ( (! ( ! (! ( (! (! ! ( (! (! ! (! (! ( (! ! (! ( ! (! ! (! ( ! ( ! ( ! ( ( ! ! (! (! ( ( (! (! ! ( (! (! (! !( ! ! ! ( ! (! ( (! !( (! ( (! ( ! (! ( (! (! ! !( ( (! (! ! (! (! ( (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! (! ! (! !( (! (! ! ! ( ! ( ( (! (! !( (! (! ( (! ! ( (! (! (! (! (! !( (! (! (! (! (! (! (! ! ! ( ! ( ! ( (! ( (! (! ! (! ( ! (! (! (! ( (! ! (! (! (! ( (! ! (! ! !( ( (! ( ! ! ! !( (! ( (! ! ( ( !( (! (! ( ! (! (! -

Massachussets
Massachussets City State Zip Code City State Zip Code Amherst MA 01002 Gloucester MA 01930 Barre MA 01005 Gloucester MA 01931 Belchertown MA 01007 Hamilton MA 01936 Bondsville MA 01009 Hathorne MA 01937 Brimfield MA 01010 Ipswich MA 01938 Easthampton MA 01027 Lynnfield MA 01940 East Longmeadow MA 01028 Manchester MA 01944 Gilbertville MA 01031 Marblehead MA 01945 Goshen MA 01032 Middleton MA 01949 Granby MA 01033 Newburyport MA 01950 Hampden MA 01036 Newbury MA 01951 Hardwick MA 01037 Salisbury MA 01952 Haydenville MA 01039 Peabody MA 01960 Leeds MA 01053 Peabody MA 01961 Leverett MA 01054 Prides Crossing MA 01965 Ludlow MA 01056 Rockport MA 01966 Monson MA 01057 Rowley MA 01969 Northampton MA 01060 Salem MA 01970 Florence MA 01062 Salem MA 01971 Northampton MA 01063 South Hamilton MA 01982 Oakham MA 01068 Topsfield MA 01983 Palmer MA 01069 Wenham MA 01984 Shutesbury MA 01072 West Newbury MA 01985 South Barre MA 01074 Accord MA 02018 South Hadley MA 01075 Bellingham MA 02019 Thorndike MA 01079 Cohasset MA 02025 Three Rivers MA 01080 Foxboro MA 02035 Wales MA 01081 Franklin MA 02038 Ware MA 01082 Greenbush MA 02040 Warren MA 01083 Hingham MA 02043 West Warren MA 01092 Hingham MA 02044 Wheelwright MA 01094 Hull MA 02045 Wilbraham MA 01095 Mansfield MA 02048 Williamsburg MA 01096 Norfolk MA 02056 Longmeadow MA 01106 Norwell MA 02061 Springfield MA 01119 Norwood MA 02062 Pittsfield MA 01201 Scituate MA 02066 Adams MA 01220 Sharon MA 02067 Ashley Falls MA 01222 Sheldonville MA 02070 Becket MA 01223 Stoughton MA 02072 Cheshire MA 01225 Walpole -
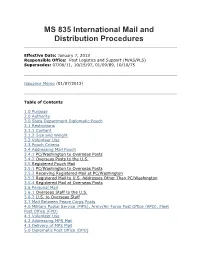
MS 835 International Mail and Distribution Procedures
MS 835 International Mail and Distribution Procedures Effective Date: January 7, 2013 Responsible Office: Post Logistics and Support (M/AS/PLS) Supersedes: 07/06/11, 10/15/97, 01/09/89, 10/10/75 Issuance Memo (01/07/2013) Table of Contents 1.0 Purpose 2.0 Authority 3.0 State Department Diplomatic Pouch 3.1 Restrictions 3.1.1 Content 3.1.2 Size and Weight 3.2 Volunteer Use 3.3 Pouch Criteria 3.4 Addressing Mail Pouch 3.4.1 PC/Washington to Overseas Posts 3.4.2 Overseas Posts to the U.S. 3.5 Registered Pouch Mail 3.5.1 PC/Washington to Overseas Posts 3.5.2 Receiving Registered Mail at PC/Washington 3.5.3 Registered Mail to U.S. Addresses Other Than PC/Washington 3.5.4 Registered Mail at Overseas Posts 3.6 Personal Mail 3.6.1 Overseas Staff to the U.S. 3.6.2 U.S. to Overseas Staff 3.7 Mail Between Peace Corps Posts 4.0 Military Postal Service (MPS), Army/Air Force Post Office (APO), Fleet Post Office (FPO) 4.1 Volunteer Use 4.2 Addressing MPS Mail 4.3 Delivery of MPS Mail 5.0 Diplomatic Post Office (DPO) 6.0 Expedited Mail Service 6.1 Preparation of Shipment 6.2 Delivery 7.0 International Postal Service (Air Mail) and Air Freight Service 7.1 Weight Restrictions 7.2 International Postal Service (Air Mail) and Air Freight Service from PC/Washington to Overseas Posts 7.2.1 Air Mail 7.2.2 Air Freight 7.3 International Postal Service (Air Mail) and Air Freight Service from Overseas Posts to PC/Washington 7.4 Mailing Government Checks 7.5 World Wise Schools (WWS) Mail 7.6 Delivery 8.0 Distribution Procedures from PC/Washington 8.1 Inter-Agency (Internal) Distribution 8.1.1 Distribution Requests to the Mail Center 8.1.2 Distribution Requests to the Mailing Services Contractor 8.2 Outgoing (External) Distribution) 1.0 Purpose This Procedural Guide sets forth Peace Corps guidance regarding international mail and pouch services. -
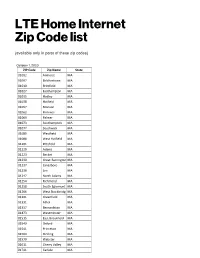
LTE Home Internet Zip Code List
LTE Home Internet Zip Code list (available only in parts of these zip codes) October 1, 2020 ZIP Code Zip Name State 01002 Amherst MA 01007 Belchertown MA 01010 Brimfield MA 01027 Easthampton MA 01035 Hadley MA 01038 Hatfield MA 01057 Monson MA 01062 Florence MA 01069 Palmer MA 01073 Southampton MA 01077 Southwick MA 01085 Westfield MA 01088 West Hatfield MA 01201 Pittsfield MA 01220 Adams MA 01223 Becket MA 01230 Great Barrington MA 01237 Lanesboro MA 01238 Lee MA 01247 North Adams MA 01254 Richmond MA 01258 South Egremont MA 01266 West Stockbridg MA 01301 Greenfield MA 01331 Athol MA 01337 Bernardston MA 01473 Westminster MA 01515 East Brookfield MA 01540 Oxford MA 01541 Princeton MA 01564 Sterling MA 01570 Webster MA 01611 Cherry Valley MA 01741 Carlisle MA 01944 Manchester MA 01951 Newbury MA 01952 Salisbury MA 01966 Rockport MA 02059 02324 Bridgewater MA 02338 Halifax MA 02379 West Bridgewate MA 02534 02536 East Falmouth MA 02537 East Sandwich MA 02539 Edgartown MA 02540 Falmouth MA 02542 Buzzards Bay MA 02554 Nantucket MA 02556 North Falmouth MA 02557 Oak Bluffs MA 02559 Pocasset MA 02563 Sandwich MA 02568 Vineyard Haven MA 02631 Brewster MA 02633 Chatham MA 02642 Eastham MA 02644 Forestdale MA 02645 Harwich MA 02650 North Chatham MA 02653 Orleans MA 02657 Provincetown MA 02662 02666 Truro MA 02667 Wellfleet MA 02668 West Barnstable MA 02670 West Dennis MA 02715 Dighton MA 02720 Fall River MA 02726 Somerset MA 02745 New Bedford MA 02746 New Bedford MA 02748 South Dartmout MA 02769 Rehoboth MA 02777 Swansea MA 02790 Westport MA 02807 -

Changing Postal ZIP Code Boundaries
Order Code RL33488 CRS Report for Congress Received through the CRS Web Changing Postal ZIP Code Boundaries June 23, 2006 Nye Stevens Specialist in American National Government Government and Finance Division Congressional Research Service ˜ The Library of Congress Changing Postal ZIP Code Boundaries Summary Ever since the ZIP Code system for identifying address locations was devised in the 1960s, some citizens have wanted to change the ZIP Code to which their addresses are assigned. Because ZIP Codes are often not aligned with municipal boundaries, millions of Americans have mailing addresses in neighboring jurisdictions. This can cause higher insurance rates, confusion in voter registration, misdirected property and sales tax revenues for municipalities, and property value effects. Some communities that lack a delivery post office complain that the need to use mailing addresses of adjacent areas robs them of a community identity. Because the ZIP Code is the cornerstone for the U.S. Postal Service’s (USPS’s) mail distribution system, USPS long resisted changing ZIP Codes for any reason other than to improve the efficiency of delivery. Frustrated citizens frequently have turned to Members of Congress for assistance in altering ZIP Code boundaries. In the 101st Congress, a House subcommittee heard testimony from Members, city officials, and the Government Accountability Office (GAO) that USPS routinely denied local requests for adjusting ZIP Code boundaries in a peremptory manner. It considered three bills that would allow local governments to determine mailing addresses for their jurisdictions. Since then, USPS has developed a “ZIP Code Boundary Review Process” that promises “every reasonable effort” to consider and if possible accommodate municipal requests to modify the last lines of an acceptable address and/or ZIP Code boundaries. -

Handbook AS-503, June 17, 2010
Contents How To Use This Handbook General Numbering System Reference Symbols Acronyms and Abbreviations Introduction 0-1 Policy Statement 0-2 Overview 0-3 Facility Types & Programs 0-4 Deviation Policy 0-5 Retail Design Review Policy 0-6 Directory Structure 0-7 USPS Reference Documents Appendices Appendix A Feedback Form Appendix B Deviation Request Form Appendix C Headquarters Design Review Form Module 1: General Criteria Chapter 1 Civil Chapter 2 Architectural Chapter 3 Structural Chapter 4 Mechanical Chapter 5 Electrical Standard Design Criteria Contents 1 Handbook AS-503, June 17, 2010 Module 2: Specific Criteria 2A Mail Processing Facilities Note that the criteria related to the facility type known as Mail Processing Facilities has been extracted and compiled in a separate folder named “MPF” (Mail Processing Facilities) in the Building Design Standards. 2B Medium Standard Building Designs (MSBD) Chapter 1 Civil (Not used, refer to Module 1, Chapter 1) Chapter 2 Architectural Chapter 3 Structural (Not used, refer to Module 1, Chapter 3) Chapter 4 Mechanical Chapter 5 Electrical 2C Small Standard Building Designs (SSBD) Chapter 1 Civil (Not used, refer to Module 1, Chapter 1) Chapter 2 Architectural Chapter 3 Structural (Not used, refer to Module 1, Chapter 3) Chapter 4 Mechanical (Not used, refer to Module 1, Chapter 4) Chapter 5 Electrical Standard Design Criteria Contents 2 Handbook AS-503, June 17, 2010 Module 3: Special Facility Types 3A Vehicle Maintenance Facilities (VMF) [See new MPF folder] 3B Modular Post Offices 3C Storage -

L601 Network Distribution Centers (Ndcs)
Labeling Lists: NDCs L601 L601 Network Distribution Centers (NDCs) [11-29-09] [10-5-09] [8-3-09] [6-1-09] L601 describes the service area by individual 3-digit ZIP Code prefix for sorting mail to NDC destinations. Use this list for: a. Standard Mail parcels and NFMs except ASF mail (other than mail for the Buffalo ASF service area) prepared and claimed at DNDC prices. Parcels and NFMs for the Buffalo ASF service area prepared and claimed at DNDC prices must be sorted to the Pittsburgh NDC. b. Standard Mail bundles, letter trays, or sacks on pallets. c. Bound Printed Matter machinable parcels except ASF mail (other than mail for the Buffalo ASF service area) prepared and claimed at DNDC prices. Machinable parcels for the Buffalo ASF service area prepared and claimed at DNDC prices must be sorted to the Pittsburgh NDC. d. Bound Printed Matter bundles or sacks on pallets. e. Parcel Post except for ASF mail (other than mail for the Buffalo ASF service area) prepared and claimed at DNDC prices and nonmachinable NDC Presort or ONDC Presort mail. Machinable parcels for the Buffalo ASF service area prepared and claimed at DNDC prices must be sorted to the Pittsburgh NDC. Nonmachinable parcels for the Buffalo ASF service area claimed at DNDC prices may be sorted to the Pittsburgh NDC if bedloaded and presented with machinable parcels. f. Presorted Media Mail and Presorted Library Mail to NDC destinations. For labeling mixed NDC sacks and pallets, mailers must add "MXD" before the Column B information of the NDC serving the 3-digit ZIP Code prefix of the Post Office at which the mail is entered. -

USPS Letterhead for HEADQUARTERS Users
December 16, 2014 Dear Retail Partners: Subject: Dangerous Goods and Export Compliance Awareness Training In 2012 the International Civil Aviation Organization (ICAO) required the U.S. Postal Service® to obtain certification from the Federal Aviation Administration (FAA) for the international air transport of mailable dangerous goods. In order for the Postal Service to maintain our certification, our employees and retail partners must complete a refresher training every two years. This training effort assures the safety of all employees and the air transportation network upon which the Postal Service relies. The enclosed Dangerous Goods and Export Compliance Awareness course is required for all Retail Partners and can be completed in less than 30 minutes. Upon completion of the training and test of knowledge, please complete and return the attached certification document to your Host Administrative Office (HAO). Documentation of the training must be completed by January 31, 2015. In addition to the training course, we are providing additional materials, Hazmat Acceptance Transactions FAQ and Poster 138, Keep the Mail Safe, which are intended as point of sale references. Any questions regarding this training or for more details on the international mail acceptance policy, please consult with your HAO. Thank you for continuing to work with us to provide the best possible international mail service. Sincerely, Sheila Marano Manager, Retail Operations (A) Training Compliance Certification Retail Name: ___________________________________________________________