Access Opening and Canal Location
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
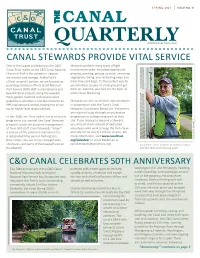
Spring 2021 | Issue No
SPRING 2021 | ISSUE NO. 31 THE CANAL QUARTERLYwww.CanalTrust.org CANAL STEWARDS PROVIDE VITAL SERVICE One of the largest contributions the C&O Stewards perform many types of light Canal Trust makes to the C&O Canal National maintenance tasks, including lopping and Historical Park is the volunteer support pruning, painting, picking up trash, removing we marshal and manage. As the Park's vegetation, raking, and restocking maps and official nonprofit partner, we are focused on trash-free park bags. It's the perfect way for providing volunteer efforts to aid National an individual, couple, or small group to get Park Service (NPS) staff in maintenance and fresh air, exercise, and care for the Park, all beautification projects along the towpath. while social distancing. Every garden mulched and invasive plant pulled by a volunteer is one less chore for an Stewards are able to set their own schedules NPS maintenance worker, freeing him or her in cooperation with the Trust's Canal up for higher-level responsibilities. Stewards Coordinator Becka Lee. Volunteers are required to go through an orientation In late 2020, the Trust added a new volunteer program prior to beginning work at their program to our arsenal, the Canal Stewards site. If you choose to become a Steward, program, which we assumed management you will join the hundreds of dedicated of from NPS staff. Canal Stewards "adopt" volunteers who work to keep the Park clean a section of the canal and maintain it for and safe for its nearly 5 million visitors. For a designated time period. Parking lots, more information, visit www.canaltrust. -

Glossary of Dental Terms
1 GLOSSARY OF DENTAL TERMS A PATIENT’S DENTAL PRIMER Amalgam - Silver filling. Bonding - Method of adhering a filling ( amalgam or composite ) to a tooth. Uses a white light to harden the material. Bridge - A cemented structure used to replace missing teeth. Composed of several caps soldered together using a pontic to replace the missing tooth. Calculus -Tartar, a hard substance that forms on the teeth. Once formed, it must be professionally removed. Composite - White filling used in front or back teeth. Crown - 1. Same thing as a cap. Can be all metal ( either gold or a combination of other met- als) or a combination of metal and an esthetic material such as porcelain. 2. The part of the tooth that is visible in the mouth. Denture - A Removable Prosthesis - can be either a full or partial ( replaces a few or several teeth) denture. Sometimes called a ' plate '. Should not be confused with a bridge. Endodontist - A dentist that specializes in performing root canal therapy. Explorer - The pointed instrument used during the examination. Frenum - The little piece of tissue which goes from the inside of your lip to the gum tissue just above your front teeth. There is also a frenum which goes from the under surfac your tongue to the bottom of your mouth. Frenum are not essential structures and very often need to be removed if they are causing physical or esthetic problems. Gingiva - Gum tissue. Inflammation - Red, sore, puffy bleeding gums tissue. Due to the accumulation of bacteria and lack of required home care. Inlay/Onlay - A type of restoration that replaces a part of the tooth. -

Flood Pulse Effects on Benthic Invertebrate Assemblages in the Hypolacustric Interstitial Zone of Lake Constance
Ann. Limnol. - Int. J. Lim. 48 (2012) 267–277 Available online at: Ó EDP Sciences, 2012 www.limnology-journal.org DOI: 10.1051/limn/2012008 Flood pulse effects on benthic invertebrate assemblages in the hypolacustric interstitial zone of Lake Constance Shannon J. O’Leary1 and Karl M. Wantzen2* 1 School of Marine and Atmospheric Sciences, Stony Brook University, Stony Brook, NY 11733, USA 2 CNRS UMR 6371 CITERES/IPAPE, De´partement des Sciences, Universite´Franc¸ois Rabelais, Parc Grandmont, 37200 Tours, France Abstract – In contrast to rivers, the effects of water level fluctuations on the biota are severely understudied in lakes. Lake Constance has a naturally pulsing hydrograph with average amplitudes of 1.4 m between winter drought and summer flood seasons (annual flood pulse (AFP)). Additionally, heavy rainstorms in summer have the potential to create short-term summer flood pulses (SFP). The flood pulse concept for lakes predicts that littoral organisms should be adapted to the regularly occurring AFP, i.e. taking advantage of benefits such as an influx of food sources and low predator pressure, though these organisms will not possess adapta- tions for the SFP. To test this hypothesis, we studied the aquatic invertebrate assemblages colonizing the gravel sediments of Lake Constance, the AFP in spring and a dramatic SFP event consisting of a one meter rise of water level in 24 h. Here, we introduce the term ‘hypolacustric interstitial’ for lakes analog to the hyporheic zone of running water ecosystems. Our results confirm the hypothesis of contrasting effects of a regular AFP and a random SFP indicating that the AFP enhances the productivity and biodiversity of the littoral zone with benthic invertebrates displaying an array of adaptations enabling them to survive. -

Material Selection and Shade Matching for a Single Central Incisor
CLINICAL SCIENCE KAHNG Material Selection and Shade Matching for a Single Central Incisor INTRODUCTION With regard to esthetics, the single central incisor poses the greatest re- by storative challenge for the clinician; not surprisingly, it can also be the most Luke S. Kahng, C.D.T. difficult tooth for the dental technician to match. Selecting the shade of the restoration depends in part on the material used for the understructure, and Mr. Kahng is the founder and owner of there is a wide assortment available from which to choose. The following are Capital Dental Technology Laboratory, among the most common: Inc., in Naperville, Illinois. The labora- tory specializes in all fixed restorations and its LSK 121 division provides per- An experienced technician can mask the underlying dark tooth color using sonalized custom cosmetic work. A porcelains with detailed color-masking techniques. strong proponent of collaborative den- tistry, Mr. Kahng stresses education, communication, and a team approach to patient care. A member of the AACD, UNDERSTRUCTURE MATERIAL his training has included extensive study with Russell DeVreugd, C.D.T., Dr. • Zirconia (e.g., Procera® [Nobel Biocare; Yorba Linda, CA], Lava™ [3M Frank Spear, Dr. Peter Dawson, and ESPE, St. Paul, MN], Cercon® [Dentsply Int., York, PA], Everest™ [KaVo others. America Corp.; Lake Zurich, IL], In-Ceram® [Vident; Brea, CA]) Mr. Kahng is the official clinician for --Flexural strength: approximately 1,200 MPa GC America, Bisco, and Captek. He is --Translucency: very low a frequent lecturer and program facili- tator for dentists and dental technicians, --Opacity: high and has published articles in Practical • Alumina core or glass-infiltrated alumina (e.g., Procera, In-Ceram) Procedures and Aesthetic Dentistry --Flexural strength: 450 to 700 MPa and Dental Dialogue. -

Intrusion of Incisors to Facilitate Restoration: the Impact on the Periodontium
Note: This is a sample Eoster. Your EPoster does not need to use the same format style. For example your title slide does not need to have the title of your EPoster in a box surrounded with a pink border. Intrusion of Incisors to Facilitate Restoration: The Impact on the Periodontium Names of Investigators Date Background and Purpose This 60 year old male had severe attrition of his maxillary and mandibular incisors due to a protrusive bruxing habit. The patient’s restorative dentist could not restore the mandibular incisors without significant crown lengthening. However, with orthodontic intrusion of the incisors, the restorative dentist was able to restore these teeth without further incisal edge reduction, crown lengthening, or endodontic treatment. When teeth are intruded in adults, what is the impact on the periodontium? The purpose of this study was to determine the effect of adult incisor intrusion on the alveolar bone level and on root length. Materials and Methods We collected the orthodontic records of 43 consecutively treated adult patients (aged > 19 years) from four orthodontic practices. This project was approved by the IRB at our university. Records were selected based upon the following criteria: • incisor intrusion attempted to create interocclusal space for restorative treatment or correction of excessive anterior overbite • pre- and posttreatment periapical and cephalometric radiographs were available • no incisor extraction or restorative procedures affecting the cementoenamel junction during the treatment period pretreatment pretreatment Materials and Methods We used cephalometric and periapical radiographs to measure incisor intrusion. The radiographs were imported and the digital images were analyzed with Image J, a public-domain Java image processing program developed at the US National Institutes of Health. -

Maxillary Lateral Incisor Agenesis and Its Relationship to Overall Tooth Size Jane Wright, DDS, MS,A Jose A
RESEARCH AND EDUCATION Maxillary lateral incisor agenesis and its relationship to overall tooth size Jane Wright, DDS, MS,a Jose A. Bosio, BDS, MS,b Jang-Ching Chou, DDS, MS,c and Shuying S. Jiang, MSd Prosthodontists, orthodontists, ABSTRACT and general dentists frequently fi Statement of problem. Agenesis of the maxillary lateral incisor has been linked to differences in encounter dif culties when the size of the remaining teeth. Thus, the mesiodistal space required for definitive esthetic resto- attempting to restore the oc- ration in patients with missing maxillary lateral incisors may be reduced. clusion if unilateral or bilateral Purpose. The purpose of this study was to determine whether a tooth size discrepancy exists in maxillary lateral incisors are orthodontic patients with agenesis of one or both maxillary lateral incisors. congenitally missing. Restora- tion of the missing lateral Material and methods. Forty sets of dental casts from orthodontic patients (19 men and 21 women; mean 15.9 years of age; all of European origin) were collected. All casts had agenesis of one incisor using an implant- or both maxillary lateral incisors. Teeth were measured with a digital caliper at their greatest supported crown, a partial mesiodistal width and then compared with those of a control group matched for ethnicity, age, and fi xed dental prosthesis, or sex. Four-factor ANOVA with repeated measures of 2 factors was used for statistical analysis (a=.05). mesial movement of the Results. Orthodontic patients with agenesis of one or both maxillary lateral incisors exhibited canine are treatment options. smaller than normal tooth size compared with the control group. -

Tooth Size Proportions Useful in Early Diagnosis
#63 Ortho-Tain, Inc. 1-800-541-6612 Tooth Size Proportions Useful In Early Diagnosis As the permanent incisors begin to erupt starting with the lower central, it becomes helpful to predict the sizes of the other upper and lower adult incisors to determine the required space necessary for straightness. Although there are variations in the mesio-distal widths of the teeth in any individual when proportions are used, the sizes of the unerupted permanent teeth can at least be fairly accurately pre-determined from the mesio-distal measurements obtained from the measurements of already erupted permanent teeth. As the mandibular permanent central breaks tissue, a mesio-distal measurement of the tooth is taken. The size of the lower adult lateral is obtained by adding 0.5 mm.. to the lower central size (see a). (a) Width of lower lateral = m-d width of lower central + 0.5 mm. The sizes of the upper incisors then become important as well. The upper permanent central is 3.25 mm.. wider than the lower central (see b). (b) Size of upper central = m-d width of lower central + 3.25 mm. The size of the upper lateral is 2.0 mm. smaller mesio-distally than the maxillary central (see c), and 1.25 mm. larger than the lower central (see d). (c) Size of upper lateral = m-d width of upper central - 2.0 mm. (d) Size of upper lateral = m-d width of lower central + 1.25 mm. The combined mesio-distal widths of the lower four adult incisors are four times the width of the mandibular central plus 1.0 mm. -

External Root Resorption of Young Premolar Teeth in Dentition With
10.5005/jp-journals-10015-1236 KapilaORIGINAL Arambawatta RESEARCH et al External Root Resorption of Young Premolar Teeth in Dentition with Crowding Kapila Arambawatta, Roshan Peiris, Dhammika Ihalagedara, Anushka Abeysundara, Deepthi Nanayakkara ABSTRACT least understood type of root resorption, characterized by its The present study was conducted to investigate the prevalence FHUYLFDOORFDWLRQDQGLQYDVLYHQDWXUH7KLVUHVRUSWLYHSURFHVV of external cervical resorption (ECR) in different tooth surfaces which leads to prRJUHVVLYHDQGXVXDOO\GHVWUXFWLYHORVVRI RIPD[LOODU\¿UVWSUHPRODUVLQD6UL/DQNDQSRSXODWLRQ tooth structure has been a source of interest to clinicians A sample of 59 (15 males, 44 females) permanent maxillary 2-5 ¿UVWSUHPRODUV DJHUDQJH\HDUV ZHUHXVHG7KHWHHWK DQGUHVHDUFKHUVIRURYHUDFHQWXU\ 7KHH[DFWFDXVHRI had been extracted for orthodontic reasons and were stored (&5LVSRRUO\XQGHUVWRRG$OWKRXJKWKHHWLRORJ\DQG LQIRUPDOLQ0RUSKRORJLFDOO\VRXQGWHHWKZHUHVHOHFWHG SDWKRJHQHVLVUHPDLQREVFXUHVHYHUDOSRWHQWLDOSUHGLVSRVLQJ IRUWKHVWXG\7KHWHHWKZHUHVWDLQHGZLWKFDUEROIXFKVLQ7KH IDFWRUVKDYHEHHQSXWIRUZDUGDQGRIWKHVHWKHLQWUDFRURQDO cervical regions of the stained teeth were observed under 10× 6 PDJQL¿FDWLRQV XVLQJ D GLVVHFWLQJ PLFURVFRSH 2O\PSXV 6= bleaching has been the most widely documented factor. In WRLGHQWLI\DQ\UHVRUSWLRQDUHDV7KHUHVRUSWLRQDUHDVSUHVHQW addition, dental trauma, orthodontic treatment, periodontal on buccal, lingual, mesial and distal aspects of all teeth were WUHDWPHQWVXUJHU\LQYROYLQJWKHFHPHQWRHQDPHOMXQFWLRQ UHFRUGHG DQGLGLRSDWKLFHWLRORJ\KDYHDOVREHHQGHVFULEHG2,7-11 -
The Cementoenamel Junction: Gap, Overlay and Edge to Edge Relationships
University of Tennessee, Knoxville TRACE: Tennessee Research and Creative Exchange Masters Theses Graduate School 8-1996 The Cementoenamel Junction: Gap, Overlay and Edge to Edge Relationships Elizabeth A. Gilb University of Tennessee, Knoxville Follow this and additional works at: https://trace.tennessee.edu/utk_gradthes Part of the Anthropology Commons Recommended Citation Gilb, Elizabeth A., "The Cementoenamel Junction: Gap, Overlay and Edge to Edge Relationships. " Master's Thesis, University of Tennessee, 1996. https://trace.tennessee.edu/utk_gradthes/4128 This Thesis is brought to you for free and open access by the Graduate School at TRACE: Tennessee Research and Creative Exchange. It has been accepted for inclusion in Masters Theses by an authorized administrator of TRACE: Tennessee Research and Creative Exchange. For more information, please contact [email protected]. To the Graduate Council: I am submitting herewith a thesis written by Elizabeth A. Gilb entitled "The Cementoenamel Junction: Gap, Overlay and Edge to Edge Relationships." I have examined the final electronic copy of this thesis for form and content and recommend that it be accepted in partial fulfillment of the requirements for the degree of Master of Arts, with a major in Anthropology. Murray Marks, Major Professor We have read this thesis and recommend its acceptance: Richard Jantz, William M. Bass, David Gerard Accepted for the Council: Carolyn R. Hodges Vice Provost and Dean of the Graduate School (Original signatures are on file with official studentecor r ds.) To the Graduate Council: I am submitting herewith a thesis written by Elizabeth A. Gilb entitled "The Cementoenamel Junction: Gap, Overlay and Edge to Edge Relationships." I have examined the finalcopy of this thesis forform and content and recommend that it be accepted in partial fulfillmentof the requirements forthe degree of Master of Arts, with a major in Anthropology. -
Teeth What Do I Need to Know?
Teeth What do I Need to Know? Enamel Enamel is a semitranslucent, highly mineralized crystalline solid which covers the crowns of teeth and acts as a barrier to protect the teeth. Dentin Dentin is less mineralized than enamel, but more mineralized than bone; it acts as a cushion for the enamel and a further barrier to the pulp. Pulp Questions? The pulp is the area in the middle of the tooth containing the blood vessels and nerves for that tooth. If you would like more Pulp Horns information or have any The projections of the pulp underneath the taller parts of the tooth, or the “cusps.” specific questions, contact*: These are the areas of the pulp which are closest to the functional (or “occlusal”) part of the tooth which is used to chew food. Leslie Blackburn Cementum XLH [email protected] Protects the dentin and pulp of the roots the and way enamel protects it in the crown. or [email protected] My Teeth XLH Network contact: Raghbir Kaur, DMD; [email protected] Scientific Advisory Board *Please include XLH in the subject line of the email. Challenges Yale-New Haven Pediatric Dental Center 1 Long Wharf Dr, Suite 403, New Haven, CT 06510 Suggestions http://www.ynhh.org/medical-services/dental_pediatric.aspx What is the Most Important Thing to Know? It is not your fault. People with XLH have unique dental challenges. Sometimes even when you are doing everything right you may still have dental problems. While it is important to do everything you can to keep your mouth healthy, it is also important to remember that you some things about your oral health are out of your control. -

TOOTH SUPPORTED CROWN a Tooth Supported Crown Is a Dental Restoration That Covers up Or Caps a Tooth
TOOTH SUPPORTED CROWN A tooth supported crown is a dental restoration that covers up or caps a tooth. It is cemented into place and cannot be taken out. Frequently Asked Questions 1. What materials are in a Tooth Supported Crown? Crowns are made of three types of materials: • Porcelain - most like a natural tooth in color • Gold Alloy - strongest and most conservative in its preparation • Porcelain fused to an inner core of gold alloy (Porcelain Fused to Metal or “PFM”) - combines strength and aesthetics 2. What are the benefits of having a Tooth Supported Crown? Crowns restore a tooth to its natural size, shape and—if using porce lain—color. They improve the strength, function and appearance of a broken down tooth that may otherwise be lost. They may also be designed to decrease the risk of root decay. 3. What are the risks of having a Tooth Supported Crown? In having a crown, some inherent risks exist both to the tooth and to the crown Porcelain crowns build back smile itself. The risks to the tooth are: • Preparation for a crown weakens tooth structure and permanently alters the tooth underneath the crown • Preparing for and placing a crown can irritate the tooth and cause “post- operative” sensitivity, which may last up to 3 months • The tooth underneath the crown may need a root canal treatment about 6% of the time during the lifetime of the tooth • If the cement seal at the edge of the crown is lost, decay may form at the juncture of the crown and tooth The risks to the crown are: • Porcelain may chip and metal may wear over time • If the tooth needs a root canal treatment after the crown is permanently cemented, the procedure may fracture the crown and the crown may need to be replaced. -

Pulpotomy Treatment for Primary Teeth
2010 National Primary Oral Health Conference October 24-27 Gaylord Palm, Orlando, Florida Pulpotomy treatment for primary teeth Enrique Bimstein Professor of Pediatric Dentistry University of Florida College of Dentistry. Pulpotomy treatment for primary teeth Goal The participants will become familiar with the basic knowledge and procedures required for the performance of the pulpotomy treatment in primary teeth. Pulpotomy treatment for primary teeth Topics Introduction Definition and rationale. Indications and contraindications. Materials and techniques. Pulpotomy technique (clinical procedures). Pulpotomy follow up. Summary and conclusions. Pulpotomy treatment for primary teeth Topics Introduction Definition and rationale. Indications and contraindications. Materials and techniques. Pulpotomy technique (clinical procedures). Pulpotomy follow up. Summary and conclusions. Preservation of the primary teeth until their time of exfoliation is required to: a. Maintain arch length, masticatory function and esthetics. Preservation of the primary teeth until their time of exfoliation is required to: a. Maintain arch length, masticatory function and esthetics. Preservation of the primary teeth until their time of exfoliation is required to: a. Maintain arch length, masticatory function and esthetics. b. Eliminate pain, inflammation and infection. Preservation of the primary teeth until their time of exfoliation is required to: a. Maintain arch length, masticatory function and esthetics. b. Eliminate pain, inflammation and infection. c. Prevent any additional pain or damage to the oral tissues. Despite all the prevention strategies, childhood caries is still a fact that we confront every day in the clinic. The retention of pulpally involved primary teeth until the time of normal exfoliation remains to be a challenge. Primary teeth with cariously exposed vital pulps should be treated with pulp therapies that allow for the normal exfoliation process.