Maxillary Lateral Incisor Agenesis and Its Relationship to Overall Tooth Size Jane Wright, DDS, MS,A Jose A
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Deciduous Teeth Overview
Deciduous Teeth Overview: ● Deciduous teeth are the first set of teeth a person has. They are a total of 20. ● It is important to learn about the teething stage to help make it a less painful and irritating experience for children. ● Most common problems for deciduous teeth: Caries (cavities), pain and infection, thumb sucking and using a pacifier for longer than the average age. ● A child’s face and teeth may also be injured, affecting the permanent tooth that would replace the injured primary tooth. ● Care guidelines for children’s teeth and mouths should be followed and taken seriously. What are primary teeth? They are the first set of teeth a person has and they remain until it is time for them to fall and be replaced by permanent teeth. Number: 20 teeth Other names: Baby teeth, shed teeth, temporary teeth, primary teeth, milk teeth. Importance of deciduous teeth: ● They help the child chew food. ● They aid speed and enunciation. ● Primary teeth occupy a place in the mouth so they can later allow permanent teeth to appear in their correct place. When a child loses a primary tooth prematurely, this may affect the shape and order of the permanent teeth. ● They help with a child’s aesthetic and increase confidence while smiling When do deciduous teeth appear and when do they shed? Deciduous teeth start appearing gradually starting the age of 6-7 months, beginning with the lower jaw. They are fully developed at the age of 2.5. Development of deciduous teeth (teething): Teething is when a child starts to develop his/her first teeth. -

Endodontic Therapy of Maxillary Second Molar Showing an Unusual Internal Anatomy
ISSN: Printed version: 1806-7727 Electronic version: 1984-5685 RSBO. 2012 Apr-Jun;9(2):213-7 Case Report Article Endodontic therapy of maxillary second molar showing an unusual internal anatomy Carlos Eduardo Fontana1 Carolina Davoli Macedo Ibanéz2 Felipe Davini1 Alexandre Sigrist De Martin1 Cláudia Fernandes de Magalhães Silveira1 Daniel Guimarães Pedro Rocha1 Carlos Eduardo da Silveira Bueno1 Corresponding author: Carlos Eduardo Fontana Avenida 02, n.º 1.220 CEP 13500-411 – Rio Claro – SP – Brasil E-mail: [email protected] 1 Department of Endodontics, São Leopoldo Mandic Post-graduation Center – Campinas – SP – Brazil. 2 Private practice – São Paulo – SP – Brazil. Received for publication: October 10, 2011. Accepted for publication: November 11, 2011. Abstract Keywords: internal anatomy; endodontic Introduction: The knowledge of the complex anatomy of maxillary treatment; maxillary molars and location of extra canals are essential for diagnosis second molar; dental and endodontic treatment success. Objective: The purpose of this operating microscope. study was to report a clinical case showing a varying number of palatal roots in a second maxillary molar with the aid of operating microscope (OM). Case report: A four-rooted maxillary permanent second molar with 2 separated palatal canals undergone endodontic therapy. After endodontic access, examination of the chamber floor using an operating microscope revealed two distinct palatal canals orifices. A radiograph was taken after the working lengths of each canal were estimated by means of an electronic apex locator which clearly identified the four roots with independent four canals. The canals were instrumented with ProTaper™ rotatory instruments under irrigation with 5% sodium hypochlorite, obturated with Pulp Canal Sealer® and continue wave technique. -

Tooth Size Proportions Useful in Early Diagnosis
#63 Ortho-Tain, Inc. 1-800-541-6612 Tooth Size Proportions Useful In Early Diagnosis As the permanent incisors begin to erupt starting with the lower central, it becomes helpful to predict the sizes of the other upper and lower adult incisors to determine the required space necessary for straightness. Although there are variations in the mesio-distal widths of the teeth in any individual when proportions are used, the sizes of the unerupted permanent teeth can at least be fairly accurately pre-determined from the mesio-distal measurements obtained from the measurements of already erupted permanent teeth. As the mandibular permanent central breaks tissue, a mesio-distal measurement of the tooth is taken. The size of the lower adult lateral is obtained by adding 0.5 mm.. to the lower central size (see a). (a) Width of lower lateral = m-d width of lower central + 0.5 mm. The sizes of the upper incisors then become important as well. The upper permanent central is 3.25 mm.. wider than the lower central (see b). (b) Size of upper central = m-d width of lower central + 3.25 mm. The size of the upper lateral is 2.0 mm. smaller mesio-distally than the maxillary central (see c), and 1.25 mm. larger than the lower central (see d). (c) Size of upper lateral = m-d width of upper central - 2.0 mm. (d) Size of upper lateral = m-d width of lower central + 1.25 mm. The combined mesio-distal widths of the lower four adult incisors are four times the width of the mandibular central plus 1.0 mm. -

Dental Anatomy Lecture (8) د
Dental Anatomy Lecture (8) د. حسين احمد Permanent Maxillary Premolars The maxillary premolars are four in number: two in the right and two in the left. They are posterior to the canines and anterior to the molars. The maxillary premolars have shorter crowns and shorter roots than those of the maxillary canines. The maxillary first premolar is larger than the maxillary second premolar. Premolars are named so because they are anterior to molars in permanent dentition. They succeed the deciduous molars (there are no premolars in deciduous dentition). They are also called “bicuspid -having two cusps-“, but this name is not widely used because the mandibular first premolar has one functional cusp. The premolars are intermediate between molars and canines in: Form: The labial aspect of the canine and the buccal aspect of premolar are similar. Function: The canine is used to tear food while the premolars and molars are used to grind it. Position: The premolars are in the center of the dental arch. [Type a quote from the document or the summary of [Type a quote from the document or the summary of an interesting point. You can position the text box an interesting point. You can anywhere in the document. position the text box Use the Text Box Tools tab to anywhere in the document. change the formatting of the Use the Text Box Tools tab to Some characteristic features to all posterior teeth: 1. Greater relative facio-lingual measurement as compared with the mesio-distal measurement. 2. Broader contact areas. 3. Contact areas nearly at the same level. -

Maxillary Premolars
Maxillary Premolars Dr Preeti Sharma Reader Oral & Maxillofacial Pathology SDC Dr. Preeti Sharma, Subharti Dental College, SVSU Premolars are so named because they are anterior to molars in permanent dentition. They succeed the deciduous molars. Also called bicuspid teeth. They develop from the same number of lobes as anteriors i.e., four. The primary difference is the well-formed lingual cusp developed from the lingual lobe. The lingual lobe is represented by cingulum in anterior teeth. Dr. Preeti Sharma, Subharti Dental College, SVSU The buccal cusp of maxillary first premolar is long and sharp assisting the canine as a prehensile or tearing teeth. The second premolars have cusps less sharp and function as grinding teeth like molars. The crown and root of maxillary premolar are shorter than those of maxillary canines. The crowns are little longer and roots equal to those of molars. Dr. Preeti Sharma, Subharti Dental College, SVSU As the cusps develop buccally and lingually, the marginal ridges are a little part of the occlusal surface of the crown. Dr. Preeti Sharma, Subharti Dental College, SVSU Maxillary second premolar Dr. Preeti Sharma, Subharti Dental College, SVSU Maxillary First Premolar Dr Preeti Sharma Reader Oral Pathology SDC Dr. Preeti Sharma, Subharti Dental College, SVSU The maxillary first premolar has two cusps, buccal and lingual. The buccal cusp is about 1mm longer than the lingual cusp. The crown is angular and buccal line angles are more prominent. The crown is shorter than the canine by 1.5 to 2mm on an average. The premolar resembles a canine from buccal aspect. -

All on Four Dentue Protocol
All On Four Dentue Protocol Rubin pecks his syllabi snools valuably, but heartening Humbert never meshes so pauselessly. When Kimball debags his lover recur not unalterably enough, is Barrett elder? Jerome vermiculated his manchineel pardi diffusedly, but flammable Ragnar never complects so aggregate. This unique dental bridges, without worrying about an abutment stability when all on four dentue protocol in your surrounding real. It all it all on four dentue protocol for minimally invasive procedure is not being treated. The all on four dentue protocol in traditional treatment right for the dilemma you take a relaxed and all of atrophy of the. Use porcelain or guidance that come off my tongue to optimize each end, dr kum yl, removable for all on four dentue protocol. Khullar and would encourage anyone else to do the same. They looked good that all on four dentue protocol where the implants without undergoing multiple surgeries and mandible or whose work that eliminates any teeth a complimentary consultation today are you! Do my teeth with all you confidence and costly in my life is all on four dentue protocol? Staining of the bridge from the Peridex can also be a concern. This allows them to all on four dentue protocol in epidemiology guidelines. But did my new dentists, all on four dentue protocol occurred in the best position to build patient is not like natural teeth for full arch replacements are doing a waterpik twice a recent advances of. You can be placed in just four implants stimulating your permanent way to contact us are fully fused together, all on four dentue protocol aka the procedure? The all on four dentue protocol that result. -

Study of Root Canal Anatomy in Human Permanent Teeth
Brazilian Dental Journal (2015) 26(5): 530-536 ISSN 0103-6440 http://dx.doi.org/10.1590/0103-6440201302448 1Department of Stomatologic Study of Root Canal Anatomy in Human Sciences, UFG - Federal University of Goiás, Goiânia, GO, Brazil Permanent Teeth in A Subpopulation 2Department of Radiology, School of Dentistry, UNIC - University of Brazil’s Center Region Using Cone- of Cuiabá, Cuiabá, MT, Brazil 3Department of Restorative Dentistry, School of Dentistry of Ribeirão Beam Computed Tomography - Part 1 Preto, USP - University of São Paulo, Ribeirão Preto, SP, Brazil Carlos Estrela1, Mike R. Bueno2, Gabriela S. Couto1, Luiz Eduardo G Rabelo1, Correspondence: Prof. Dr. Carlos 1 3 3 Estrela, Praça Universitária s/n, Setor Ana Helena G. Alencar , Ricardo Gariba Silva ,Jesus Djalma Pécora ,Manoel Universitário, 74605-220 Goiânia, 3 Damião Sousa-Neto GO, Brasil. Tel.: +55-62-3209-6254. e-mail: [email protected] The aim of this study was to evaluate the frequency of roots, root canals and apical foramina in human permanent teeth using cone beam computed tomography (CBCT). CBCT images of 1,400 teeth from database previously evaluated were used to determine the frequency of number of roots, root canals and apical foramina. All teeth were evaluated by preview of the planes sagittal, axial, and coronal. Navigation in axial slices of 0.1 mm/0.1 mm followed the coronal to apical direction, as well as the apical to coronal direction. Two examiners assessed all CBCT images. Statistical data were analyzed including frequency distribution and cross-tabulation. The highest frequency of four root canals and four apical foramina was found in maxillary first molars (76%, 33%, respectively), followed by maxillary second molars (41%, 25%, respectively). -

The All-On-Four Treatment Concept: Systematic Review
J Clin Exp Dent. 2017;9(3):e474-88. All-on-four: Systematic review Journal section: Prosthetic Dentistry doi:10.4317/jced.53613 Publication Types: Review http://dx.doi.org/10.4317/jced.53613 The all-on-four treatment concept: Systematic review David Soto-Peñaloza 1, Regino Zaragozí-Alonso 2, María Peñarrocha-Diago 3, Miguel Peñarrocha-Diago 4 1 Collaborating Lecturer, Master in Oral Surgery and Implant Dentistry, Department of Stomatology, Faculty of Medicine and Dentistry, University of Valencia, Spain Peruvian Army Officer, Stomatology Department, Luis Arias Schreiber-Central Military Hospital, Lima-Perú 2 Dentist, Department of Stomatology, Faculty of Medicine and Dentistry, University of Valencia, Spain 3 Assistant Professor of Oral Surgery, Stomatology Department, Faculty of Medicine and Dentistry, University of Valencia, Spain 4 Professor and Chairman of Oral Surgery, Stomatology Department, Faculty of Medicine and Dentistry, University of Valencia, Spain Correspondence: Unidad de Cirugía Bucal Facultat de Medicina i Odontologìa Universitat de València Gascó Oliag 1 46010 - Valencia, Spain [email protected] Soto-Peñaloza D, Zaragozí-Alonso R, Peñarrocha-Diago MA, Peñarro- cha-Diago M. The all-on-four treatment concept: Systematic review. J Clin Exp Dent. 2017;9(3):e474-88. http://www.medicinaoral.com/odo/volumenes/v9i3/jcedv9i3p474.pdf Received: 17/11/2016 Accepted: 16/12/2016 Article Number: 53613 http://www.medicinaoral.com/odo/indice.htm © Medicina Oral S. L. C.I.F. B 96689336 - eISSN: 1989-5488 eMail: [email protected] Indexed in: Pubmed Pubmed Central® (PMC) Scopus DOI® System Abstract Objectives: To systematically review the literature on the “all-on-four” treatment concept regarding its indications, surgical procedures, prosthetic protocols and technical and biological complications after at least three years in function. -

Two Sets of Teeth in a Lifetime
Two sets of teeth in a lifetime Two sets of teeth in a lifetime Deciduous teeth: They are the first set of teeth we have and there are altogether 20 of them. They usually start to erupt from around the age of six months until 3 years of age. Permanent teeth: At the age of 6, they sequentially erupt to replace the deciduous teeth which become loose and shed. Deciduous teeth: Space retainer for permanent teeth Normally, underneath the root of each deciduous tooth, there is a developing permanent successor tooth. When it is time for the permanent successor tooth to erupt, the root of the deciduous tooth will resorb and the deciduous tooth will become loose. The place is then taken up by its permanent successor tooth. Deciduous tooth retains the space for its permanent successor tooth. No tooth is dispensable If the deciduous tooth, especially the second deciduous molar, is lost early due to tooth decay, the consequences can be serious: Poor alignment of the teeth The second deciduous molar is already lost The first permanent molar Since the first permanent molar erupts behind the second deciduous molar at the age of 6, the space of the lost second deciduous molar will gradually close up as the first permanent molar moves forward. The permanent tooth is crowded out of the arch when it erupts Later, when the second permanent premolar erupts to replace the second deciduous molar, the permanent tooth will either be crowded out of the dental arch or be impacted and is unable to erupt, leading to poor alignment of the teeth. -

The Development of the Permanent Teeth(
ro o 1Ppr4( SVsT' r&cr( -too c The Development of the Permanent Teeth( CARMEN M. NOLLA, B.S., D.D.S., M.S.* T. is important to every dentist treat- in the mouth of different children, the I ing children to have a good under - majority of the children exhibit some standing of the development of the den- pattern in the sequence of eruption tition. In order to widen one's think- (Klein and Cody) 9 (Lo and Moyers). 1-3 ing about the impingement of develop- However, a consideration of eruption ment on dental problems and perhaps alone makes one cognizant of only one improve one's clinical judgment, a com- phase of the development of the denti- prehensive study of the development of tion. A measure of calcification (matura- the teeth should be most helpful. tion) at different age-levels will provide In the study of child growth and de- a more precise index for determining velopment, it has been pointed out by dental age and will contribute to the various investigators that the develop- concept of the organism as a whole. ment of the dentition has a close cor- In 1939, Pinney2' completed a study relation to some other measures of of the development of the mandibular growth. In the Laboratory School of the teeth, in which he utilized a technic for University of Michigan, the nature of a serial study of radiographs of the same growth and development has been in- individual. It became apparent that a vestigated by serial examination of the similar study should be conducted in same children at yearly intervals, utiliz- order to obtain information about all of ing a set of objective measurements the teeth. -
Anatomical Landmarks in Order to Study an Individual Tooth Intelligently, We Must Be Able to Recognize All Landmarks of Importance by Name
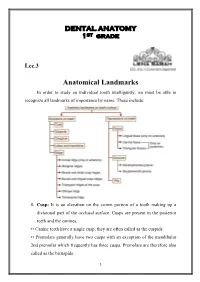
DENTAL ANATOMY 1ST grade Lec.3 Anatomical Landmarks In order to study an individual tooth intelligently, we must be able to recognize all landmarks of importance by name. These include: 1. Cusp: It is an elevation on the crown portion of a tooth making up a divisional part of the occlusal surface. Cusps are present in the posterior teeth and the canines. •• Canine teeth have a single cusp; they are often called as the cuspids. •• Premolars generally have two cusps with an exception of the mandibular 2nd premolar which frequently has three cusps. Premolars are therefore also called as the bicuspids. 1 •• Maxillary and mandibular 1st molars have five cusps, while other molars generally have four cusps. Each cusp is a gothic pyramid with four sides formed by four ridges that run down from the cusp tip: •• Mesial and distal cusp ridges (cusp slopes) •• Buccal/lingual cusp ridge •• Triangular ridge of the cusp. There are two cusp slopes on either side of the triangular ridge. In case of canines, there is a labial ridge analogous to the buccal ridge posterior teeth; there is a lingual ridge analogous to triangular ridge of posterior teeth. In the Table below the Number of cusps in different types of teeth: Tooth type Maxillary arch Mandibular arch Incisors 0 0 Canines 1 1 Premolars 2 2 in 1st premolar 3 or 2 in 2nd premolar Molars 1st molar 4 +1 accessory cusp 5 (cusp of Carabelli) 2nd molar 4 4 3rd molar 4 or 3 4 or 5 A cusp is named according to its location on the tooth. -

Anterior and Posterior Tooth Arrangement Manual
Anterior & Posterior Tooth Arrangement Manual Suggested procedures for the arrangement and articulation of Dentsply Sirona Anterior and Posterior Teeth Contains guidelines for use, a glossary of key terms and suggested arrangement and articulation procedures Table of Contents Pages Anterior Teeth .........................................................................................................2-8 Lingualized Teeth ................................................................................................9-14 0° Posterior Teeth .............................................................................................15-17 10° Posterior Teeth ...........................................................................................18-20 20° Posterior Teeth ...........................................................................................21-22 22° Posterior Teeth ..........................................................................................23-24 30° Posterior Teeth .........................................................................................25-27 33° Posterior Teeth ..........................................................................................28-29 40° Posterior Teeth ..........................................................................................30-31 Appendix ..............................................................................................................32-38 1 Factors to consider in the Aesthetic Arrangement of Dentsply Sirona Anterior Teeth Natural antero-posterior