Malignant Phyllodes Tumor of the Breast: a Practice Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
C O N F E R E N C E 22 27 April 2016
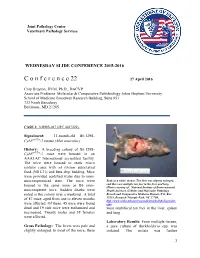
Joint Pathology Center Veterinary Pathology Services WEDNESDAY SLIDE CONFERENCE 2015-2016 C o n f e r e n c e 22 27 April 2016 Cory Brayton, DVM, Ph.D., DACVP Associate Professor, Molecular & Comparative Pathobiology Johns Hopkins University School of Medicine Broadway Research Building, Suite 851 733 North Broadway Baltimore, MD 21205 CASE I: NIEHS-087 (JPC 4017222). Signalment: 11-month-old B6.129S- Cybbtm1Din/J mouse (Mus musculus) History: A breeding colony of B6.129S- Cybbtm1Din/J mice were housed in an AAALAC International accredited facility. The mice were housed in static micro isolator cases with ad libitum autoclaved food (NIH-31) and beta chip bedding. Mice were provided acidified water due to imm- unocompromised state. The mice were Body as a while, mouse. The liver was slightly enlarged, housed in the same room as B6 imm- and there are multiple tan foci in the liver and lung. (Photo courtesy of: National Institute of Environmental unocompetent mice. Sudden deaths were Health Sciences, Cellular and Molecular Pathology noted in the colony over a weekend. A total Branch and Comparative Medicine Branch, P.O. Box of 87 mice, aged from one to eleven months 12233, Research Triangle Park, NC 27709, http://www.niehs.nih.gov/research/atniehs/labs/lep/index. were affected. Of these, 45 mice were found cfm) dead and 19 sick mice were euthanized and were multifocal tan foci in the liver, spleen necropsied. Twenty males and 38 females and lung. were affected. Laboratory Results: From multiple tissues, Gross Pathology: The livers were pale and a pure culture of Burkholderia spp. -

Understanding Your Pathology Report: Benign Breast Conditions
cancer.org | 1.800.227.2345 Understanding Your Pathology Report: Benign Breast Conditions When your breast was biopsied, the samples taken were studied under the microscope by a specialized doctor with many years of training called a pathologist. The pathologist sends your doctor a report that gives a diagnosis for each sample taken. Information in this report will be used to help manage your care. The questions and answers that follow are meant to help you understand medical language you might find in the pathology report from a breast biopsy1, such as a needle biopsy or an excision biopsy. In a needle biopsy, a hollow needle is used to remove a sample of an abnormal area. An excision biopsy removes the entire abnormal area, often with some of the surrounding normal tissue. An excision biopsy is much like a type of breast-conserving surgery2 called a lumpectomy. What does it mean if my report uses any of the following terms: adenosis, sclerosing adenosis, apocrine metaplasia, cysts, columnar cell change, columnar cell hyperplasia, collagenous spherulosis, duct ectasia, columnar alteration with prominent apical snouts and secretions (CAPSS), papillomatosis, or fibrocystic changes? All of these are terms that describe benign (non-cancerous) changes that the pathologist might see under the microscope. They do not need to be treated. They are of no concern when found along with cancer. More information about many of these can be found in Non-Cancerous Breast Conditions3. What does it mean if my report says fat necrosis? Fat necrosis is a benign condition that is not linked to cancer risk. -

Bilateral Giant Juvenile Fibroadenomas of Breasts: a Case Report
SAGE-Hindawi Access to Research Pathology Research International Volume 2011, Article ID 482046, 4 pages doi:10.4061/2011/482046 Case Report Bilateral Giant Juvenile Fibroadenomas of Breasts: A Case Report D. B. Nikumbh, S. R. Desai, P. S. Madan, N. J. Patil, and J. V. Wader Department of Pathology, Krishna Institute of Medical Sciences, Karad, District Satara, Maharashtra 415110, India Correspondence should be addressed to D. B. Nikumbh, drdhirajnikumbh@rediffmail.com Received 9 October 2010; Revised 4 April 2011; Accepted 7 April 2011 Academic Editor: Elizabeth Wiley Copyright © 2011 D. B. Nikumbh et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Juvenile fibroadenoma constitutes only 4% of the total fibroadenomas. The incidence of giant juvenile fibroadenomas is found to be only 0.5% of all the fibroadenomas. Bilateral giant juvenile fibroadenomas are extremely rare, and only four cases have been reported in the literature. Tothe best of our knowledge, we are presenting the fifth case of bilateral giant juvenile fibroadenomas in a 12-year-old prepubertal girl. The diagnosis was made on fine-needle aspiration cytology which was confirmed on histopathology. In this paper, we present this rare case to illustrate the diagnosis and management of this tumour and to emphasize that these tumours are almost always benign and should be treated with breast-conserving surgery to provide a healthy physical and social life to the patient. 1. Introduction both the breasts were seen, which were firm in consistency. -

Diagnostic Approach to Soft Tissue Tumour of the Breast and Phyllodes Tumour in Ilorin, North Central with Review of Institutional Experience
World Journal of Medical Case Reports 2021; 2(3): 29-34 http://www.sciencepublishinggroup.com/j/wjmcr doi: 10.11648/j.wjmcr.20210203.11 Diagnostic Approach to Soft Tissue Tumour of the Breast and Phyllodes Tumour in Ilorin, North Central with Review of Institutional Experience Rasheed Mumini Wemimo 1, *, Afolayan Enoch Abiodun 1, Adegboye Adeyemi Taiwo 2 1Department of Pathology, University of Ilorin Teaching Hospital, Ilorin, Nigeria 2Mojitaiwo Data Services and Data Management Executives, Ilorin, Nigeria Email address: *Corresponding author To cite this article: Rasheed Mumini Wemimo, Afolayan Enoch Abiodun, Adegboye Adeyemi Taiwo. Diagnostic Approach to Soft Tissue Tumour of the Breast and Phyllodes Tumour in Ilorin, North Central with review of Institutional Experience. World Journal of Medical Case Reports. Vol. 2, No. 3, 2021, pp. 29-34. doi: 10.11648/j.wjmcr.20210203.11 Received : May 13, 2021; Accepted : June 7, 2021; Published : July 9, 2021 Abstract: Background: Primary soft tissue tumour (primary mesenchymal tumour) of the breast comprised of spectrum of neoplasm that arise from mammary stroma with comparable tumour biology of primary mesenchymal tumour at other sites. There are palpable diagnostic challenges which can be resolved by considering histomorphologic analysis that characterized each tumour entity regardless of the site and the use immunohistochemical markers. Methodology: This is an analytical hospital based retrospective study of patients with primary breast mesenchymal tumour and phyllodes diagnosed during 2014– 2019 at the Department of Pathology, University of Ilorin Teaching Hospital. The histopathological diagnosis of primary mesenchymal tumour of the breast and phyllodes tumours with documented age and other inclusion criteria were used for the study but excluded patients with incomplete information. -

Primary Breast Leiomyosarcoma and Synchronous Homolateral Lung Cancer: a Case Report
1059 Case Report Primary breast leiomyosarcoma and synchronous homolateral lung cancer: a case report Alberto Testori1, Stefano Meroni2, Emanuele Voulaz1, Marco Alloisio1, Rita De Sanctis3,4, Paola Bossi5, Umberto Cariboni1, Matilde De Simone6, Ugo Cioffi6 1General and Thoracic Surgery, Humanitas Research Hospital, Rozzano (Milan), Italy; 2Division of Breast Radiology, European Institute of Oncology, Milan, Italy; 3Department of Medical Oncology and Hematology, Humanitas Research Hospital, Rozzano (Milan), Italy; 4Molecular and Cellular Networks Lab, Department of Anatomy, Histology, Forensic Medicine and Orthopaedics, 'Sapienza' University, Rome, Italy; 5Department of Anatomo-Pathology, Humanitas Research Hospital, Rozzano (Milan), Italy; 6Department of Surgery, University of Milan, Milan, Italy Correspondence to: Alberto Testori, MD. General and Thoracic Surgery, Humanitas Research Hospital, Via Manzoni, 56, 20089 Rozzano (Milan), Italy. Email: [email protected]. Abstract: Radiological and histological features of breast leiomyosarcoma can mimic a wide variety of other breast lesions, such as mesenchymal tumors, breast lymphomas, poorly differentiated carcinomas and metaplastic breast carcinomas. The authors present the case of a 62-year-old woman with a primary breast leiomyosarcoma with synchronous ipsilateral lung adenocarcinoma. The latter was an incidental finding during pre-surgical staging examinations. Clinicopathological, immunophenotypic and imaging features cancer are described. A brief review of the literature on imaging findings and management of breast leiomyosarcoma is presented. The authors discuss the differential diagnoses in breast imaging and of the extra-mammary incidental findings. Surgical resection remains the cornerstone of treatment, while radiation therapy and chemotherapy remain to be defined on a single-patient basis. Keywords: Breast leiomyosarcoma; lung cancer; synchronous tumors Submitted May 14, 2017. -

Phyllodes Tumor of the Vulva: Report of Two Cases Vulvanın Fillods Tümörü: İki Olgu Sunumu
Olgu Sunumu/Case Report doi: 10.5146/tjpath.2013.01153 Phyllodes Tumor of the Vulva: Report of Two Cases Vulvanın Fillods Tümörü: İki Olgu Sunumu İrem Hicran Özbudak1, Hampar Akkaya2, Bahar Akkaya1, Gülgün ERDOĞAN1, Hadice Elif PEŞTERElİ1, Fatma Şeyda Karavelİ1 1Department of Pathology, Akdeniz University, Faculty of Medicine, ANTALYA, TURKEY, 2Başkent University, Faculty of Medicine, Alanya Hospital, ANTALYA, TURKEY ABSTRACT ÖZ Ectopic breast tissue can occur anywhere along the primitive Ektopik meme dokusu ilkel embriyonik sütyolu boyunca herhangi bir embryonic milk line and can be the site of the same pathologic yerde ortaya çıkabilir ve normal memede izlenebilen aynı patolojik processes found in the normal breast. Phyllodes tumor is an durumlar ektopik meme dokusunda da görülebilir. Fillods tümör extremely rare fibroepithelial neoplasm that occurs in ectopic breast vulvadaki ektopik meme dokusunda oluşan nadir bir fibroepitelyal tissue of the vulva. To date, only 8 cases of phyllodes tumor in the neoplazidir. Literatürde bugüne kadar 8 olgu bildirilmiştir. Bu vulva have been reported in the literature. This paper presents two makalede literatüre ek olarak iki ayrı vulvar fillods tümör vakası additional case of benign phyllodes tumor in the vulva. The first sunulmuştur. İlk olgu, sol ön mons pubiste boyutu son üç ayda artış patient was a 43-year-old woman, presenting with a lesion on the gösteren bir lezyon ile kliniğe başvurmuş 43 yaşında kadın hastadır. left anterior mons pubis that had increased in size in the last three İkinci olgu 50 yaşında kadın hasta olup, iki aydır varolan sağ labium months. The second patient was a 50-year-old woman, presenting majusta kitle ile başvurmuştur. -

Giant Juvenile Fibroadenoma of Breast
Journal of Surgical Sciences (2013) Vol. 17 (2) : 99-102 © 2012 Society of Surgeons of Bangladesh JOURNAL OF SURGICAL SCIENCES Case Report GIANT JUVENILE FIBROADENOMA OF BREAST 2 2 3 5 KABM Taiful Alam1, Toufiqul Haque , Shamim Hossain , Kuntal Das , Tazul lslam4, Helena Ahmed Abstract: Giant juvenile fibroadenoma occurs in adolescent girls. These tumours become enormous in size and grow rapidly, though these tumours are mostly benign. These patients are almost always treated by breast conserving surgery. Here we present a case having unilateral giant juvenile fibroadenoma with bilateral multiple small fibroadenomas in an adolescent female aged 16years. The diagnosis of the patient was made on clinical examination, USG & FNAC. Confirmatory diagnosis was made by histopathology. We removed the giant one with "Swiss-Roll" procedure and others by simple enucleation. The aesthatic appearence of the breasts were preserved. Key words: Fibroadenoma, Giant fibroadenoma, Juvenile fibroadenoma, Swiss-roll operation. Introduction: can grow to immense proportions, compressing and Fibroadenoma is the most common benign tumour of displacing normal breast tissue and stretching the 4 female breast.It usually arises in the fully developed overlying skin and nipple areola complex . breast during the 15-25 years age period. They arise from hyperplasia of both fibrous & glandular tissue of Case report: a single lobule & usually grow upto 2-3 cm in size. A 16 year old girl presented with bilateral breast lumps Juvenile fibroadenoma is a benign tumour which occurs for 1 year. There were multiple lumps in the both during puberty1. It is a rare clinical condition and forms breasts among them one lump in the left breast was 4% of the total fibroadenomes--'. -

Investigations of Breast Tumors Withfluorine
10. Pacini F, Gasperi M, Fugazzola L, et al. Testicular thyroid cancer: potential risks and recommendations. dent: temporal correlation or casual relation? Br MedJ function in patients with differentiated thyroid carci Ear J Nuc! Med I993:20:192—194. 1994:309:158—162. noma treated with radioiodine. J Nucl Med 1994:35: 23. Dottorini ME, Lomuscio G, Mazzucchelli L, Vignati 34. Harjuletho T, Aro T, Rita H. Rytomaa T, SaxénL. The 1418 —1422. A, Colombo L. Assessment of female fertility and accident at Chernobyl and outcome of pregnancy in 11. Brincker H, Hansen HS, Andersen AP. Induction of carcinogenesis after iodine-I 3 1 therapy for differenti Finland. Br Med J I989:288:995—997. leukaemia by ‘@‘Itreatment ofthyroid carcinoma. BrJ ated thyroid carcinoma. J Nod Med 1995:36:21—27. 35. Bertollini R, Di Lallo D. Mastroiacovo P. Perucci CA. Cancer 1973:28:232—237. 24. Schlumberger M, Dc Vathaire F. Ceccarelli C, et al. Reduction of births in Italy after the Chemobyl acci 12. Hall P. HoIm LE, Lundell G. et al. Cancer risks in Exposure to radioactive iodine for scintigraphy or dent. Scandi Work Environ Health 1990:16:96—101. thyroid cancer patients. Br J Cancer 1991:64:159—163. therapy does not preclude pregnancy in thyroid cancer 36. Hawkins MM, Draper Gi, Winter DL. Cancer in the patients. J Nucl Med 1996:37:606—612. 13. Sobels FH. Estimation of the genetic risk resulting offspring of survivors of childhood leukemia and 25. Izembart M, Chavaudra J, Aubert B, ValléeG. Retro @ from the treatment of women with ‘I. -

Management of Fibroadenomas of the Breast
- Official Statement - Management of Fibroadenomas of the Breast Fibroadenoma of the breast is a common benign lesion affecting women during their reproductive years. Despite their benignity, fibroadenomas can cause physical deformity due to large size and may produce discomfort or emotional distress in affected individuals. The traditional management options available to women diagnosed with a fibroadenoma include observation or surgical excision. Two newer approaches, percutaneous excision and in situ cryoablation, have been developed and are less invasive than surgical excision. The purpose of this consensus statement is to put these four management options into perspective for our members and their patients. In most patients with fibroadenoma(s), the ideal approach is confirmation with percutaneous core biopsy and conservative follow-up. Because the malignant potential of fibroadenomas is extremely low, treatment is not required on an oncologic basis. This conservative approach is the least costly in terms of dollars and morbidity. A significant minority of fibroadenomas will disappear without treatment; with the remaining lesions either increasing in size or remaining unchanged. Because fibroadenomas can be bothersome to some patients, causing physical deformity, discomfort or emotional distress, most breast surgeons will respect an informed patient's preference for treatment. Traditional open excisional biopsy is effective treatment in such cases but it is the most costly option because of the operating room charges and time off from work. Open excision may still be the best option in some cases based on large size of the fibroadenoma or the judgment of the surgeon or patient preference. Studies have shown that ultrasound guided percutaneous excision of fibroadenomas is safe, effective and well tolerated by patients. -

Pleomorphic Liposarcoma of the Male Breast: Lessons from a Rare
Case report BMJ Case Rep: first published as 10.1136/bcr-2021-244056 on 20 July 2021. Downloaded from Pleomorphic liposarcoma of the male breast: lessons from a rare malignancy during COVID-19 pandemic Brijesh Kumar Singh ,1 Manjunath Maruti Pol ,1 Toshib G A,1 Adarsh Wamanrao Barwad2 1Surgery, All India Institute of SUMMARY mobility over the chest wall. The nipple, areola and Medical Sciences, New Delhi, A 52-year -old man presented with a recurrent right side overlying skin were not involved. The contralateral India breast examination was unremarkable. There was 2 breast lump. He had undergone excision of a lump on Department of Pathology, the right breast followed by adjuvant chemoradiotherapy no clinically palpable axillary and supraclavicular All India Institute of Medical 1 year ago for a diagnosis of pleomorphic liposarcoma. lymph nodes. Sciences, New Delhi, India Imaging revealed a 47×36 mm lesion on the right side of the chest wall involving the pectoralis muscle. The Correspondence to INVESTIGATIONS patient underwent right radical mastectomy. Histology of Dr Manjunath Maruti Pol; Biopsy of the lump yielded focal chronic inflamma- manjunath. pol@ gmail. com the specimen showed an undifferentiated pleomorphic tion with few foamy macrophages. In view of high sarcoma infiltrating into the underlying skeletal muscle. suspicion of recurrence, contrast- enhanced CT Accepted 21 June 2021 Therefore, he was planned for chemoradiotherapy. But of thorax and positron emission tomography and due to lockdown during the COVID-19 pandemic, he CT (PET- CT) were performed to stage the tumour was lost to follow-up and later presented with malignant and assess resectability. -

Non-Cancerous Breast Conditions Fibrosis and Simple Cysts in The
cancer.org | 1.800.227.2345 Non-cancerous Breast Conditions ● Fibrosis and Simple Cysts ● Ductal or Lobular Hyperplasia ● Lobular Carcinoma in Situ (LCIS) ● Adenosis ● Fibroadenomas ● Phyllodes Tumors ● Intraductal Papillomas ● Granular Cell Tumors ● Fat Necrosis and Oil Cysts ● Mastitis ● Duct Ectasia ● Other Non-cancerous Breast Conditions Fibrosis and Simple Cysts in the Breast Many breast lumps turn out to be caused by fibrosis and/or cysts, which are non- cancerous (benign) changes in breast tissue that many women get at some time in their lives. These changes are sometimes called fibrocystic changes, and used to be called fibrocystic disease. 1 ____________________________________________________________________________________American Cancer Society cancer.org | 1.800.227.2345 Fibrosis and cysts are most common in women of child-bearing age, but they can affect women of any age. They may be found in different parts of the breast and in both breasts at the same time. Fibrosis Fibrosis refers to a large amount of fibrous tissue, the same tissue that ligaments and scar tissue are made of. Areas of fibrosis feel rubbery, firm, or hard to the touch. Cysts Cysts are fluid-filled, round or oval sacs within the breasts. They are often felt as a round, movable lump, which might also be tender to the touch. They are most often found in women in their 40s, but they can occur in women of any age. Monthly hormone changes often cause cysts to get bigger and become painful and sometimes more noticeable just before the menstrual period. Cysts begin when fluid starts to build up inside the breast glands. Microcysts (tiny, microscopic cysts) are too small to feel and are found only when tissue is looked at under a microscope. -

Chapter 10 Gene Expression Signatures of Breast Phyllodes
Chapter 10 Gene expression signatures of breast phyllodes tumor and fibroadenoma A Kuijper E Korsching C Kersting E van der Wall H Bürger PJ van Diest Manuscript Chapter 10 Abstract Phyllodes tumor (PT) and fibroadenoma share morphological similarities but display different clinical behavior. In addition, fibroadenoma may progress to PT by monoclonal stromal expansion. We compared transcriptome-wide levels of gene expression of both tumors and normal breast tissue in order to gain insight into the molecular mechanisms driving development and progression of fibroepithelial tumors. We used the Affymetrix GeneChip HG-U133A 2.0, which contains more than 22000 probe-sets, to examine gene expression profiles of fibroadenomas (n=5) and phyllodes tumors (n=8). Profiles were compared to signatures of normal breast as well. Immunohistochemical validation of microarray data was performed for two genes, c-kit and CXCR4, on tissue microarrays (TMA) composed of 58 PTs and 167 fibroadenomas. We detected many novel genes with a possible role in the pathogenesis of fibroepithelial tumors. IGF-2 showed strong upregulation in fibroadenoma when compared to normal tissue. Among the genes displaying strongest downregulation in fibroadenoma were several genes involved in steroid binding and metabolism (SCGB1D2, SCGB2A2, SCGB2A1, SULT2B1) and galactose metabolism (LALBA). In comparison to the normal breast, PT showed downregulation of DNA repair genes (POLL, RECQL, TP73L), cell adhesion genes (PKP1, CX3CL1, FAT2, DSC1), transcription factors (ETV4, TP73L, SOX10, KLF5, BCL11B) and growth factors (TGFA, EGF, PDGFC). As compared to fibroadenoma, PT displayed upregulation of 26 genes and downregulation of 52 genes. Downregulation was found of genes involved in transcription (EGR1, ELF5, LZTS1), cell adhesion (JAM2, PCDH11X, CX3CL1), apoptosis (TNFSF8, PHLDA1) and Wnt signaling (FRZB, SFRP1).