Effect of Nasal Balloon Autoinflation in Children with Otitis Media with Effusion in Primary Care: an Open Randomized Controlled Trial
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hearing Thresholds, Tinnitus, and Headphone Listening Habits in Nine-Year-Old Children
International Journal of Audiology ISSN: 1499-2027 (Print) 1708-8186 (Online) Journal homepage: http://www.tandfonline.com/loi/iija20 Hearing thresholds, tinnitus, and headphone listening habits in nine-year-old children Sara Båsjö, Claes Möller, Stephen Widén, Göran Jutengren & Kim Kähäri To cite this article: Sara Båsjö, Claes Möller, Stephen Widén, Göran Jutengren & Kim Kähäri (2016) Hearing thresholds, tinnitus, and headphone listening habits in nine-year-old children, International Journal of Audiology, 55:10, 587-596, DOI: 10.1080/14992027.2016.1190871 To link to this article: http://dx.doi.org/10.1080/14992027.2016.1190871 © 2016 The Author(s). Published by Informa UK Limited, trading as Taylor & Francis Group. Published online: 22 Jun 2016. Submit your article to this journal Article views: 456 View related articles View Crossmark data Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=iija20 Download by: [Linköping University Library] Date: 07 November 2016, At: 05:25 International Journal of Audiology 2016; 55: 587–596 Original Article Hearing thresholds, tinnitus, and headphone listening habits in nine-year-old children Sara Ba˚sjo¨1,2, Claes Mo¨ller1, Stephen Wide´n1,Go¨ran Jutengren3 & Kim Ka¨ha¨ri4 1Audiological Research Centre, School of Health and Medical Sciences / Swedish Institute for Disability Research, O¨ rebro University Hospital, O¨ rebro University, O¨ rebro, Sweden, 2HEAD Graduate School, Linko¨ping University, Linko¨ping, Sweden, 3School of Health Sciences, University of Bora˚s, Bora˚s, Sweden, and 4Division of Audiology, Sahlgrens’ Academy at Go¨teborg University, Go¨teborg, Sweden ABSTRACT Objective: Investigate hearing function and headphone listening habits in nine-year-old Swedish children. -
Introduction to Tympanometry
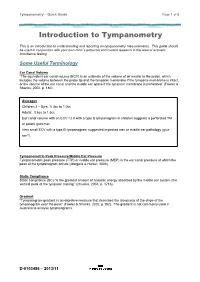
Tympanometry – Quick Guide Page 1 of 6 Introduction to Tympanometry This is an introduction to understanding and reporting on tympanometry measurements. This guide should be used in conjunction with your own clinic’s protocols and current research in the area of acoustic immittance testing. Some Useful Terminology Ear Canal Volume “The equivalent ear canal volume (ECV) is an estimate of the volume of air medial to the probe, which includes the volume between the probe tip and the tympanic membrane if the tympanic membrane is intact, or the volume of the ear canal and the middle ear space if the tympanic membrane is perforated” (Fowler & Shanks, 2002, p. 180). Averages Children 3 – 5yrs: 0.4cc to 1.0cc Adults: 0.6cc to 1.5cc Ear canal volume with an ECV >2.0 with a type B tympanogram in children suggests a perforated TM or patent grommet. Very small ECV with a type B tympanogram suggested impacted wax or middle ear pathology (glue ear?). Tympanometric Peak Pressure/Middle Ear Pressure Tympanometric peak pressure (TTP) or middle ear pressure (MEP) is the ear canal pressure at which the peak of the tympanogram occurs (Margolis & Hunter, 2000). Static Compliance Static compliance (SC) “is the greatest amount of acoustic energy absorbed by the middle ear system (the vertical peak of the tympanic tracing)” (Onusko, 2004, p. 1716). Gradient “Tympanogram gradient is an objective measure that describes the steepness of the slope of the tympanogram near the peak” (Fowler & Shanks, 2002, p.182). The gradient is not commonly used in Australia to analyse -

Radiographic Mastoid and Middle Ear Effusions in Intensive Care Unit Subjects
Radiographic Mastoid and Middle Ear Effusions in Intensive Care Unit Subjects Phillip Huyett MD, Yael Raz MD, Barry E Hirsch MD, and Andrew A McCall MD BACKGROUND: This study was conducted to determine the incidence of and risk factors associ- ated with the development of radiographic mastoid and middle ear effusions (ME/MEE) in ICU patients. METHODS: Head computed tomography or magnetic resonance images of 300 subjects admitted to the University of Pittsburgh Medical Center neurologic ICU from April 2013 through April 2014 were retrospectively reviewed. Images were reviewed for absent, partial, or complete opacification of the mastoid air cells and middle ear space. Exclusion criteria were temporal bone or facial fractures, transmastoid surgery, prior sinus or skull base surgery, history of sinonasal malignancy, ICU admission < 3 days or inadequate imaging. RESULTS: At the time of admission, of subjects subsequently (31 ؍ of subjects had radiographic evidence of ME/MEE; 10.3% (n 3.7% developed new or worsening ME/MEE during their ICU stay. ME/MEE was a late finding and was found to be most prevalent in subjects with a prolonged stay (P < .001). Variables associated with ME/MEE included younger age, the use of antibiotics, and development of radiographic sinus opacification. The proportion of subjects with ME/MEE was significantly higher in the presence of an endotracheal tube (22.7% vs 0.6%, P < .001) or a nasogastric tube (21.4% vs 0.6%, P < .001). CONCLUSIONS: Radiographic ME/MEE was identified in 10.3% of ICU subjects and should be considered especially in patients with prolonged stay, presence of an endotracheal tube or naso- gastric tube, and concomitant sinusitis. -

Strand B, Rapid Assessment of Other Health Technologies Such As Medical Devices, Surgical Interventions Or Diagnostics
333 EUnetHTA WP5 Joint Action 2 (2012-2015) Strand B, Rapid assessment of other health technologies such as medical devices, surgical interventions or diagnostics Pilot rapid assessment of other health technologies using the HTA Core Model® for Rapid Relative Effectiveness Assessment Balloon Eustachian tuboplasty for the treatment of Eustachian tube dysfunction Pilot ID: SB-13 Version 5.0, February, 2015 Final Version EUnetHTA JA2 Balloon Eustachian tuboplasty for the treatment of Eustachian tube dysfunction WP5B DOCUMENT HISTORY AND CONTRIBUTORS Version Date Description V1.0 26 August 2014 V1.0 = First draft V2.0 29 September 2014 Updated following review by dedicated reviewers V 3.0 13 November 2014 Updated version based on comments from external clinical experts, WP5 strand B members and manufacturers V 4.0 15 December 2014 Updated version based on the comments and corrections from medical editing V 5.0 3 February Updated version based on comments from LBI This assessment was produced by experts from the institutions listed below, and was reviewed by members of Work Package 5 (WP5) Joint Action 2 of the EUnetHTA network; the whole process was coordinated by the Ludwig Boltzmann Institute for Health Technology Assessment (LBI-HTA). Disclaimer The assessment represents a consolidated view of the EUnetHTA network members and is in no case the official opinion of the participating institutions or individuals. EUnetHTA Joint Action 2 is supported by a grant from the European Commission. The sole responsibility for the content of this document lies with the authors and neither the European Commission nor EUnetHTA are re- sponsible for any use that may be made of the information contained therein. -

Audiometric Test Procedures
Audiometric Test Procedures 101 This information is meant to help you better understand the various test procedures as well as some of the terms you might see on an audiometric report. By Larry Medwetsky individual could, in fact, exhibit nor- In the previous issue of Hearing mal hearing acuity across these three Loss Magazine, I provided an over- Anyone who has ever had their frequencies, yet, exhibit a significant view concerning hearing threshold hearing tested should know how hearing loss in the higher frequencies results as recorded on the audiogram to read the audiogram, but that’s (3000-8000 Hz). Thus, it is important and an explanation of the pure-tone easier said than done. Hopefully, to examine the SRT in the context of audiogram. In this article, I will after reading this article you will the other audiometric test findings. describe various test procedures have a greater understanding of the Speech Awareness Threshold that are typically administered in principles discussed and use your (SAT): an audiometric evaluation and what knowledge going forward—be it in Compound words are pre- information the tests provide. reviewing hearing test results you sented, the goal being to determine already have or when discussing your the softest level one can detect the Audiometric Test Procedures results at your next hearing test. presence of words. This test is often Pure-tone Audiometry: Tones of used when an individual’s hearing loss different frequencies are presented; the is so great that the person is unable goal is to find the softest sound level relatively flat hearing losses, and the to recognize/repeat the words, yet is which one can hear (threshold) the average of 500 and 1000 Hz for those aware that words have been presented. -

Chapter 9 Hearing Loss
Chapter 9 Hearing loss 9.1 Estimation of noise induced hearing loss on the basis of the record of past noise exposure Noise-induced hearing loss is considered to become a detectable per- manent hearing loss through the repetition of temporary hearing loss and its recovery that starts an undetectable infinitesimal permanent hearing loss and its accumulation. The past noise exposure during the Vietnam War era was estimated in the previous section using measurements recorded at the residential areas in the vicinity of Kadena airfield in 1968 and 1972. The estimated WECPNL was around 105, and the equivalent continuous sound pressure level, LAeq, for averaging time of 24 hours came to 83 dB. These values are serious when com- pared with the permissible criteria of occupational noise exposure for hearing conservation recommended by Japan Society for Occupational Health which is 80 dB for 24 working hours a day. The criteria is provided in the expectation that average hearing loss can be controlled after prolonged exposure of over years under 20 dB for the test frequency of 4 kHz. 9.1.1 Estimation of TTS due to aircraft noise A method of computation of average temporary threshold shift (TTS) (Takagi K, Hiramatsu K & Yamamoto T; 1988) is available if the temporal and spectral features of noise exposure are given; in its turn, permanent aver- age hearing loss can be estimated to a certain extent from past measurement of noise exposure. The method consists of two stages. One is the critical band theory with respect to TTS, which deals with the spectral aspect of the exposure noise. -

Benign Paroxysmal Positional Vertigo and Tinnitus
DOI: 10.5935/0946-5448.20130003 ORIGINAL ARTICLE International Tinnitus Journal. 2013;18(1):16-19. Benign paroxysmal positional vertigo and tinnitus Stefania Barozzi1 Marina Socci1 Daniela Ginocchio1 Eliana Filipponi2 Maria Grazia Troja Martinazzoli1 Antonio Cesarani1 Abstract Introduction: In our clinical experience, some of the patients affected by benign paroxysmal positional vertigo (BPPV) reported the onset of tinnitus shortly before or in association with the positional vertigo. Objectives: The aim of this study was to describe the prevalence and the clinical patterns of tinnitus episodes which occurred in association with BPPV and to suggest possible interpretative hypotheses. Methods: 171 normal hearing patients affected by BPPV (50 males and 122 females; age range: 25-77 years; mean age 60.3 years ± 14.9) underwent pure tone audiome- try, immittance test and a clinical vestibular evaluation before and after repositioning manoeuvers. Those suffering from tinnitus were also assessed using visual analogue scales and tinnitus handicap inventory. Results: 19.3% of the patients reported the appearance of tinnitus concurrently with the onset of the positional vertigo. It was mostly unilateral, localized on the same ear as the BPPV, slight in intensity and intermittent. Tinnitus disappeared or decreased in all patients except two, either spontaneously, before performing the therapeutic manoeuvers, or shortly after. Conclusions: A possible vestibular origin of tinnitus determined by the detachment of macular debris into the ductus reuniens and cochlear duct is discussed. Keywords: tinnitus, vertigo, vestibular diseases. 1 Audiology Unit, Department of Clinical Sciences and Community Health, Università degli Studi di Milano; Fondazione IRCCS Ca’ Granda, Ospedale Maggiore Policlinico. E-mail: [email protected]. -

Tympanometry EDWARD ONUSKO, M.D., Clinton Memorial Hospital, Wilmington, Ohio
Tympanometry EDWARD ONUSKO, M.D., Clinton Memorial Hospital, Wilmington, Ohio Tympanometry provides useful quantitative information about the presence of fluid in the middle ear, mobility of the middle ear system, and ear canal volume. Its use has been recommended in conjunction with more qualitative information (e.g., history, appearance, and mobility of the tympanic membrane) in the evaluation of otitis media with effusion and to a lesser extent in acute otitis media. It also can provide useful information about the patency of tympanostomy tubes. Tympanometry is not reliable in infants younger than seven months because of the highly compliant ear canals of infants. Tympanogram tracings are classified as type A (normal), type B (flat, clearly abnormal), and type C (indicating a significantly negative pressure in the middle ear, possibly indicative of pathology). According to the Agency for Healthcare Research and Quality guidelines on otitis media with effusion, the positive predictive value of an abnormal (flat, type B) tympanogram is between 49 and 99 percent. A type C curve may be useful when correlated with other findings, but by itself it is an imprecise estimate of middle ear pressure and does not have high sensitivity or specificity for middle ear disorders. (Am Fam Physician 2004;70:1713-20. Copy- right© 2004 American Academy of Family Physicians.) titis media with effusion (OME) tympanic membrane should be performed is defined as fluid in the middle before tympanometry.6 Using pneumatic ear without signs or symptoms otoscopy with tympanometry improves of ear infection.1 Acute otitis the accuracy of diagnosis because many O media (AOM) is defined as the presence of abnormalities of the eardrum and ear canal middle ear effusion in conjunction with the that might cause an abnormal tracing can recent, abrupt onset of one or more signs be visualized. -

Giant Congenital Cholesteatoma of the Temporal Bone
Global Journal of Otolaryngology ISSN 2474-7556 Case Report Glob J Otolaryngol Volume 18 Issue 5 - January 2019 Copyright © All rights are reserved by Cristina Laza DOI: 10.19080/GJO.2019.18.555998 Giant Congenital Cholesteatoma of the Temporal Bone Cristina Laza* and Eugenia Enciu Clinical county hospital for emergencies Constanta, Romania Submission: December 15, 2018; Published: January 03, 2019 *Corresponding author: Cristina Laza, Clinical county hospital for emergencies Constanta, Romania Abstract Congenital or primitive cholesteatoma is a benign disease with slow progressive growth that destroys neighboring structures. It is a rare disease considered an epidermal cyst originating from the remnants of squamous keratinized epithelium, in several regions of the temporal bone such as in the middle ear (most frequent) as well as in the petrous apex, cerebellopontine cistern, external acoustic meatus and mastoid process. In this case report, we present a giant congenital cholesteatoma, occupying a part of the petrous part of the temporal bone, including middle ear and mastoid process discovered at a 12-years-old girl as an acute right otomastoiditis complicated with retro auricular abscess. There were no history of ear infections, trauma or previous surgeries on this area, the eardrum was intact, all the accusing starts after an infection of the naos- pharynx –typical for congenital cholesteatoma. In emergency using a retro auricular approach we drain the abscess located sub-periosteal a minutia’s excision of the cholesteatoma and a permanent follow up recurrence was discovered after 4 years at 16 years old –without signs of infectionand finally but we with remove tinnitus the andcholesteatoma vertigo and usingwe explore a radical the mastoidectomycavity and remove with the canal new wallcholesteatoma. -

Differential Diagnosis and Treatment of Hearing Loss JON E
Differential Diagnosis and Treatment of Hearing Loss JON E. ISAACSON, M.D., and NEIL M. VORA, M.D., Milton S. Hershey Medical Center, Hershey, Pennsylvania Hearing loss is a common problem that can occur at any age and makes verbal communication difficult. The ear is divided anatomically into three sections (external, middle, and inner), and pathology contributing to hearing loss may strike one or more sections. Hearing loss can be cat- egorized as conductive, sensorineural, or both. Leading causes of conductive hearing loss include cerumen impaction, otitis media, and otosclerosis. Leading causes of sensorineural hear- ing loss include inherited disorders, noise exposure, and presbycusis. An understanding of the indications for medical management, surgical treatment, and amplification can help the family physician provide more effective care for these patients. (Am Fam Physician 2003;68:1125-32. Copyright© 2003 American Academy of Family Physicians) ore than 28 million Amer- tive, the sound will be heard best in the icans have some degree of affected ear. If the loss is sensorineural, the hearing impairment. The sound will be heard best in the normal ear. differential diagnosis of The sound remains midline in patients with hearing loss can be sim- normal hearing. Mplified by considering the three major cate- The Rinne test compares air conduction gories of loss. Conductive hearing loss occurs with bone conduction. The tuning fork is when sound conduction is impeded through struck softly and placed on the mastoid bone the external ear, the middle ear, or both. Sen- (bone conduction). When the patient no sorineural hearing loss occurs when there is a longer can hear the sound, the tuning fork is problem within the cochlea or the neural placed adjacent to the ear canal (air conduc- pathway to the auditory cortex. -

An Integrated Osteopathic Treatment Approach in Acute Otitis Media
C A RF IC)RT S • An integrated osteopathic treatment approach in acute otitis media WILLIAM J. PINTAL, no MARGOT E. KURTZ, PhD Ear pain is a common patient pathogens, Streptococcus pneumoniae and Haemo- complaint in the practice of the primary philus influenzae, causative agents may include care physician. Acute otitis media can Streptococcus pyogenes, Staphylococcus aureus, My- affect a person of any age, although it is coplasma pneumoniae, and Corynebacterium diphth- more often seen in children than in adults. eriae. The disease is usually caused by Classically, the tympanic membrane is thick- Streptococcus pneumoniae (Diplococcus ened, and a gray or amber fluid is seen in the mid- pneumoniae) or Haemophilus influenzae. dle ear. Sometimes a fluid meniscus, air bubbles The differential diagnosis and subsequent of bluish fluid, may appear behind the tympanic treatment of otitis media is approximately membrane, the mobility of which is generally im- the same for children and adults. First-line paired. Depending on individual circumstances, the therapy usually consists of an antibiotic tympanic membrane may be either bulging or re- regimen of amoxicillin in combination with tracted. The bulging or retraction may result from autoinflation exercises. In the case the development of a positive or negative internal presented, a pharmacologic regimen was pressure, respectively, caused by dysfunction of the combined with osteopathic manipulation. eustachian tube. In the differential diagnosis, one must distin- guish between an acute purulent otitis media and In the course of caring for a wide range of pa- a serous or mucoid otitis media as well as between tients of different ages in a general practice–fam- the short-term perforation of the tympanic mem- ily medicine setting, one has the opportunity to care brane that is associated with acute purulent otitis for many ear infections. -
Audiometric Findings with Voluntary Tensor Tympani Contraction Brandon Wickens1 , Duncan Floyd2 and Manohar Bance3*
Wickens et al. Journal of Otolaryngology - Head and Neck Surgery (2017) 46:2 DOI 10.1186/s40463-016-0182-y ORIGINALRESEARCHARTICLE Open Access Audiometric findings with voluntary tensor tympani contraction Brandon Wickens1 , Duncan Floyd2 and Manohar Bance3* Abstract Background: Tensor tympani contraction may have a "signature" audiogram. This study demonstrates audiometric findings during voluntary tensor tympani contraction. Methods: Five volunteers possessing the ability to voluntarily contract their tensor tympani muscles were identified and enrolled. Tensor tympani contraction was confirmed with characteristic tympanometry findings. Study subjects underwent conventional audiometry. Air conduction and bone conduction threshold testing was performed with and without voluntary tensor tympani contraction. Main outcome measure: Changes in air conduction and bone conduction thresholds during voluntary tensor tympani contraction. Results: Audiometric results demonstrate a low frequency mixed hearing loss resulting from tensor tympani contraction. Specifically, at 250 Hz, air conduction thresholds increased by 22 dB and bone conduction thresholds increased by 10 dB. Conclusions: Previous research has demonstrated a low frequency conductive hearing loss in the setting of tensor tympanic contraction. This is the first study to demonstrate a low frequency mixed hearing loss associated with tensor tympani contraction. This finding may aid in the diagnosis of disorders resulting from abnormal tensor tympani function. Tensor tympani contraction