Current Practices in the Assessment of Recreational Noise-Induced Hearing Loss: a Review
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Temporo-Mandibular Joint (Tmj) Dysfunction
Office: (310) 423-1220 BeverlyHillsENT.com Fax: (310) 423-1230 TEMPORO-MANDIBULAR JOINT (TMJ) DYSFUNCTION You may not have heard of it, but you use it hundreds of times every day. It is the Temporo- Mandibular Joint (TMJ), the joint where the mandible (the lower jaw) joins the temporal bone of the skull, immediately in front of the ear on each side of your head. You move the joint every time you chew or swallow. You can locate this joint by putting your finger on the triangular structure in front of your ear. Then move your finger just slightly forward and press firmly while you open your jaw all the way and shut it. The motion you feel is the TMJ. You can also feel the joint motion in your ear canal. These maneuvers can cause considerable discomfort to a patient who is having TMJ trouble, and physicians use these maneuvers with patients for diagnosis. TMJ Dysfunction can cause the following symptoms: Ear pain Sore jaw muscles Temple/cheek pain Jaw popping/clicking Locking of the jaw Difficulty in opening the mouth fully Frequent head/neck aches The pain may be sharp and searing, occurring each time you swallow, yawn, talk, or chew, or it may be dull and constant. It hurts over the joint, immediately in front of the ear, but pain can also radiate elsewhere. It often causes spasms in the adjacent muscles that are attached to the bones of the skull, face, and jaws. Then, pain can be felt at the side of the head (the temple), the cheek, the lower jaw, and the teeth. -

Hearing Thresholds, Tinnitus, and Headphone Listening Habits in Nine-Year-Old Children
International Journal of Audiology ISSN: 1499-2027 (Print) 1708-8186 (Online) Journal homepage: http://www.tandfonline.com/loi/iija20 Hearing thresholds, tinnitus, and headphone listening habits in nine-year-old children Sara Båsjö, Claes Möller, Stephen Widén, Göran Jutengren & Kim Kähäri To cite this article: Sara Båsjö, Claes Möller, Stephen Widén, Göran Jutengren & Kim Kähäri (2016) Hearing thresholds, tinnitus, and headphone listening habits in nine-year-old children, International Journal of Audiology, 55:10, 587-596, DOI: 10.1080/14992027.2016.1190871 To link to this article: http://dx.doi.org/10.1080/14992027.2016.1190871 © 2016 The Author(s). Published by Informa UK Limited, trading as Taylor & Francis Group. Published online: 22 Jun 2016. Submit your article to this journal Article views: 456 View related articles View Crossmark data Full Terms & Conditions of access and use can be found at http://www.tandfonline.com/action/journalInformation?journalCode=iija20 Download by: [Linköping University Library] Date: 07 November 2016, At: 05:25 International Journal of Audiology 2016; 55: 587–596 Original Article Hearing thresholds, tinnitus, and headphone listening habits in nine-year-old children Sara Ba˚sjo¨1,2, Claes Mo¨ller1, Stephen Wide´n1,Go¨ran Jutengren3 & Kim Ka¨ha¨ri4 1Audiological Research Centre, School of Health and Medical Sciences / Swedish Institute for Disability Research, O¨ rebro University Hospital, O¨ rebro University, O¨ rebro, Sweden, 2HEAD Graduate School, Linko¨ping University, Linko¨ping, Sweden, 3School of Health Sciences, University of Bora˚s, Bora˚s, Sweden, and 4Division of Audiology, Sahlgrens’ Academy at Go¨teborg University, Go¨teborg, Sweden ABSTRACT Objective: Investigate hearing function and headphone listening habits in nine-year-old Swedish children. -
Introduction to Tympanometry
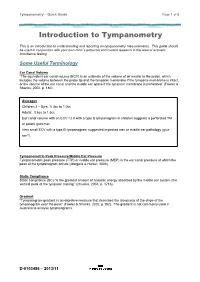
Tympanometry – Quick Guide Page 1 of 6 Introduction to Tympanometry This is an introduction to understanding and reporting on tympanometry measurements. This guide should be used in conjunction with your own clinic’s protocols and current research in the area of acoustic immittance testing. Some Useful Terminology Ear Canal Volume “The equivalent ear canal volume (ECV) is an estimate of the volume of air medial to the probe, which includes the volume between the probe tip and the tympanic membrane if the tympanic membrane is intact, or the volume of the ear canal and the middle ear space if the tympanic membrane is perforated” (Fowler & Shanks, 2002, p. 180). Averages Children 3 – 5yrs: 0.4cc to 1.0cc Adults: 0.6cc to 1.5cc Ear canal volume with an ECV >2.0 with a type B tympanogram in children suggests a perforated TM or patent grommet. Very small ECV with a type B tympanogram suggested impacted wax or middle ear pathology (glue ear?). Tympanometric Peak Pressure/Middle Ear Pressure Tympanometric peak pressure (TTP) or middle ear pressure (MEP) is the ear canal pressure at which the peak of the tympanogram occurs (Margolis & Hunter, 2000). Static Compliance Static compliance (SC) “is the greatest amount of acoustic energy absorbed by the middle ear system (the vertical peak of the tympanic tracing)” (Onusko, 2004, p. 1716). Gradient “Tympanogram gradient is an objective measure that describes the steepness of the slope of the tympanogram near the peak” (Fowler & Shanks, 2002, p.182). The gradient is not commonly used in Australia to analyse -

Investigation of the Incidence of Eustachian Tube Dysfunction in Patients with Sinonasal Disease*
ORIGINAL CONTRIBUTION Investigation of the incidence of Eustachian tube dysfunction in patients with sinonasal disease* 1 2 1 1 C.E. Rennie , M. Gutierrez , Y. Darby , V.J. Lund Rhinology Online, Vol 1: 85 - 89, 2018 http://doi.org/10.4193/RHINOL/18.050 1 Royal National Throat Nose and Ear Hospital, ENT, London, United Kingdom 2 University of North Carolina, Medical student, North Carolina, USA *Received for publication: August 12, 2018 Accepted: August 14, 2018 Abstract Background: Rhinosinusitis is characterised by inflammation affecting the respiratory mucosa of the nose and sinuses. Since the Eustachian tube and the middle ear cavity are also lined by the same mucosa, it is likely that the pathophysiological processes that give rise to rhinosinusitis will also affect these areas. Eustachian tube dysfunction (ETD) is a common condition, but it is often dismissed as a "minor" symptom in rhinology patients. Objective: The aim of this study was to determine the frequency of otologic symptoms in patients attending the rhinology clinic. The seven-item Eustachian Tube Dysfunction Questionnaire (ETDQ-7), a validated disease-specific instrument was used to assess symptoms with respect to ETD7. Study design: 119 patients attending the rhinology outpatient clinic completed ETDQ-7, a SNOT 22 and had their PNIF measured. Results: The results showed a significantly higher rate of ETD (p<0.01 paired t-test) in the rhinology patients (mean score 3.1, SD 1.64) as compared to a control population (mean 1.3, SD 0.3). Conclusion: Eustachian tube dysfunction is more common in rhinology patients then the general population, and within the rhinology population. -

Acoustic Trauma and Hyperbaric Oxygen Treatment
Acoustic Trauma and Hyperbaric Oxygen Treatment Mesut MUTLUOGLU Department of Underwater and Hyperbaric Medicine Gulhane Military Medical Academy Haydarpasa Teaching Hospital 34668, Uskudar, Istanbul TURKEY [email protected] ABSTRACT As stated in the conclusions of the HFM-192 report on hyperbaric oxygen therapy (HBOT) in military medical setting, acoustic trauma is a frequent consequence of military activity in operation. Acoustic trauma refers to an acute hearing loss following a single sudden and very intense noise exposure. It differs from chronic noise induced hearing (NIHL) loss in that it is usually unilateral and causes sudden profound hearing loss. Acoustic trauma is a type of sensorineural hearing loss affecting inner ear structures; particularly the inner and outer hair cells of the organ of Corti within the cochlea. Exposure to noise levels above 85 decibel (dB) may cause hearing loss. While long-term exposure to repetitive or continuous noise above 85 dB may cause chronic NIHL, a single exposure above 130-140 dB, as observed in acoustic trauma, may cause acute NIHL. The loudest sound a human ear may tolerate without pain varies individually, but is usually around 120dB. Military personnel are especially at increased risk for acoustic trauma due to fire arm use in the battle zone. While a machine gun generates around 145dB sound, a rifle generates 157- 163dB, a 105 mm towed howitzer 183dB and an improvised explosive device around 180dB sound. Acoustic trauma displays a gradually down-slopping pattern in the audiogram, particularly after 3000Hz and is therefore described as high-frequency hearing loss. Tinnitus is almost always associated with acoustic trauma. -

Investigations of Auditory Filters Based Excitation Patterns for Assessment of Noise Induced Hearing Loss
Investigations of Auditory Filters Based Excitation Patterns for Assessment of Noise Induced Hearing Loss Wisam Subhi Al-Dayyeni, Pengfei Sun, Jun Qin Department of Electrical and Computer Engineering, Southern Illinois University, Carbondale, IL, USA Abstract: Noise induced hearing loss (NIHL) as one of major avoidable occupational related health issues has been studied for decades. To assess NIHL, the excitation pattern (EP) has been considered as one of mechanisms to estimate movements of basilar membrane (BM) in cochlea. In this study, two auditory filters, dual resonance nonlinear (DRNL) filter and rounded- exponential (ROEX) filter, have been applied to create two EPs, referring as the velocity EP and the loudness EP, respectively. Two noise hazard metrics are also proposed based on the developed EPs to evaluate hazardous levels caused by different types of noise. Moreover, Gaussian noise and pure-tone noise have been simulated to evaluate performances of the developed EPs and noise metrics. The results show that both developed EPs can reflect the responses of BM to different types of noise. For Gaussian noise, there is a frequency shift between the velocity EP and the loudness EP. For pure-tone noise, both EPs can reflect the frequencies of input noise accurately. The results suggest that both EPs can be potentially used for assessment of NIHL. Key words: Noise induced hearing loss; excitation pattern; basilar membrane motion; auditory filter; noise assessment metrics. 1. Introduction Noise-induced hearing loss (NIHL) remains as one of the most common health related problems nowadays as stated by the World Health Organization (WHO). One of the main causes of the permanent hearing loss is the exposure to excessive noise [1-3]. -

Radiographic Mastoid and Middle Ear Effusions in Intensive Care Unit Subjects
Radiographic Mastoid and Middle Ear Effusions in Intensive Care Unit Subjects Phillip Huyett MD, Yael Raz MD, Barry E Hirsch MD, and Andrew A McCall MD BACKGROUND: This study was conducted to determine the incidence of and risk factors associ- ated with the development of radiographic mastoid and middle ear effusions (ME/MEE) in ICU patients. METHODS: Head computed tomography or magnetic resonance images of 300 subjects admitted to the University of Pittsburgh Medical Center neurologic ICU from April 2013 through April 2014 were retrospectively reviewed. Images were reviewed for absent, partial, or complete opacification of the mastoid air cells and middle ear space. Exclusion criteria were temporal bone or facial fractures, transmastoid surgery, prior sinus or skull base surgery, history of sinonasal malignancy, ICU admission < 3 days or inadequate imaging. RESULTS: At the time of admission, of subjects subsequently (31 ؍ of subjects had radiographic evidence of ME/MEE; 10.3% (n 3.7% developed new or worsening ME/MEE during their ICU stay. ME/MEE was a late finding and was found to be most prevalent in subjects with a prolonged stay (P < .001). Variables associated with ME/MEE included younger age, the use of antibiotics, and development of radiographic sinus opacification. The proportion of subjects with ME/MEE was significantly higher in the presence of an endotracheal tube (22.7% vs 0.6%, P < .001) or a nasogastric tube (21.4% vs 0.6%, P < .001). CONCLUSIONS: Radiographic ME/MEE was identified in 10.3% of ICU subjects and should be considered especially in patients with prolonged stay, presence of an endotracheal tube or naso- gastric tube, and concomitant sinusitis. -

MASTOIDECTOMY (With Or Without Tympanoplasty)
MASTOIDECTOMY (with or without tympanoplasty) Informed Surgical Consent A mastoidectomy is a surgical procedure that removes diseased mastoid air cells. These cells sit behind your ear in a hollow space in your skull. Typically, a mastoidectomy (with or without tympanoplasty) is recommended for patients that have a cholesteatoma and/or a chronically infected ear that has failed medical management (chronic otitis media). Your doctor at Suburban Ear, Nose, and Throat is uniquely trained to perform mastoidectomy surgery. A cholesteatoma is a benign skin cyst that grows inside the ear. Most cholesteatomas occupy the middle ear space behind the tympanic membrane (eardrum). Occasionally, cholesteatomas arise from the external ear canal, and then are referred to as canal cholesteatomas. Canal cholesteatomas can usually be managed conservatively with routine ear cleaning in the office, but rarely they will require surgical intervention. Middle ear cholesteatomas, on the other hand, almost always require surgery. They typically occur in children and adults who have chronic eustachian tube dysfunction (ETD), a problem with ventilation or "popping" the ears. When ETD is present for many years, it can lead to development of a cholesteatoma. Although most cholesteatomas are acquired, some patients are actually born with the cholesteatoma; this is called a congenital cholesteatoma. Cholesteatomas grow very slowly, but they can cause significant damage to any structure in the ear that they come in contact with. Commonly, the cholesteatoma erodes into the tiny bones (ossicles) in the middle ear that allow for hearing. Untreated, cholesteatomas can lead to hearing loss, infection, chronic ear discharge, ear pain, dizziness, facial paralysis, or in rare cases, infection that spreads to the brain. -

Audiometric Test Procedures
Audiometric Test Procedures 101 This information is meant to help you better understand the various test procedures as well as some of the terms you might see on an audiometric report. By Larry Medwetsky individual could, in fact, exhibit nor- In the previous issue of Hearing mal hearing acuity across these three Loss Magazine, I provided an over- Anyone who has ever had their frequencies, yet, exhibit a significant view concerning hearing threshold hearing tested should know how hearing loss in the higher frequencies results as recorded on the audiogram to read the audiogram, but that’s (3000-8000 Hz). Thus, it is important and an explanation of the pure-tone easier said than done. Hopefully, to examine the SRT in the context of audiogram. In this article, I will after reading this article you will the other audiometric test findings. describe various test procedures have a greater understanding of the Speech Awareness Threshold that are typically administered in principles discussed and use your (SAT): an audiometric evaluation and what knowledge going forward—be it in Compound words are pre- information the tests provide. reviewing hearing test results you sented, the goal being to determine already have or when discussing your the softest level one can detect the Audiometric Test Procedures results at your next hearing test. presence of words. This test is often Pure-tone Audiometry: Tones of used when an individual’s hearing loss different frequencies are presented; the is so great that the person is unable goal is to find the softest sound level relatively flat hearing losses, and the to recognize/repeat the words, yet is which one can hear (threshold) the average of 500 and 1000 Hz for those aware that words have been presented. -

Tinnitus What Is Tinnitus? Tinnitus Is Defined As the Perception of Sound When No External Sound Is Present
Tinnitus What is tinnitus? Tinnitus is defined as the perception of sound when no external sound is present. The common vernacular is "ringing in the ears"; however, the quality of the tinnitus can range from roaring to hissing and chirping to clicking. Tinnitus can pulsate or be constant. It can be a single tone or multiple tones, and it's amplitude can vary from background noise to an excruciating experience. What causes tinnitus? Tinnitus has a variety of causes. The most common causes include wax in the ear canal, noise trauma or temporomandibular joint (TMJ) dysfunction. It can also be caused by Meniere's disease, endolymphatic hydrops, allergies, destruction of the middle ear bones, infection, nutritional deficiency, cardiovascular disease, thyroid disorders, certain medications, head injury and cervical disorders. Recently, migraine disorders have also been listed as a culprit. Regardless of the inciting etiology, it has been shown that the it is within the brain that the sound resides, persists, evolves and propagates. Tinnitus may begin with damage to the peripheral auditory system (the cochlea and auditory nerve), but its persistence is a function of the attention that it receives parietal cortex and frontal cortex), the importance that it is given (cingulate cortex, anterior insula) and it maintaining residence in the limbic system (the amygdala, hippocampus and thalamus). Ongoing research is being aggressively pursued to stop this feed-forward cycle in its tracks. Medications that may exacerbate tinnitus (adapted from Bailey's Otolaryngology - Head and Neck Surgery 4th ed.) include aspirin and aspirin-containing compounds, aminoglycoside antibiotics, nonsteroidal antiinflammatory drugs and heterocycline antidepressants. -

TMJ (Temporo-Mandibular Joint) Syndrome
TMJ (Temporo-Mandibular Joint) Syndrome What is the TMJ? You may not have heard of it, but you use it hundreds of times every day. It is the Temporo- Mandibular Joint (TMJ), the joint where the mandible (the lower jaw) joins the temporal bone of the skull, immediately in front of the ear on each side of the head. Each time you chew you move it. But you also move it every time you talk and every time you swallow (every 3 minutes or so). It is, therefore, one of the most frequently used of all the joints of the body. You can locate that joint by putting your finger on the triangular structure in front of your ear. Then move your finger just slightly forward and press firmly while you open your jaw all the way and shut it. The motion you feel is the TMJ. You can also feel the joint motion in your ear canal. These maneuvers can cause considerable discomfort to a patient who is having TMJ trouble, and doctors use these maneuvers with patients for diagnosis. How does the TMJ work? When you bite down hard, you put force on the object between your teeth and on the joint. In terms of physics, the jaw is the lever and the TMJ is the fulcrum. Actually, more force is applied (per square inch) to the joint surface than to whatever is between your teeth. To accommodate such forces and to prevent too much wear and tear, the joint was designed to be a sliding joint, rather than the usual ball-and-socket type joint (such as the hip and shoulder, for example). -

Chapter 9 Hearing Loss
Chapter 9 Hearing loss 9.1 Estimation of noise induced hearing loss on the basis of the record of past noise exposure Noise-induced hearing loss is considered to become a detectable per- manent hearing loss through the repetition of temporary hearing loss and its recovery that starts an undetectable infinitesimal permanent hearing loss and its accumulation. The past noise exposure during the Vietnam War era was estimated in the previous section using measurements recorded at the residential areas in the vicinity of Kadena airfield in 1968 and 1972. The estimated WECPNL was around 105, and the equivalent continuous sound pressure level, LAeq, for averaging time of 24 hours came to 83 dB. These values are serious when com- pared with the permissible criteria of occupational noise exposure for hearing conservation recommended by Japan Society for Occupational Health which is 80 dB for 24 working hours a day. The criteria is provided in the expectation that average hearing loss can be controlled after prolonged exposure of over years under 20 dB for the test frequency of 4 kHz. 9.1.1 Estimation of TTS due to aircraft noise A method of computation of average temporary threshold shift (TTS) (Takagi K, Hiramatsu K & Yamamoto T; 1988) is available if the temporal and spectral features of noise exposure are given; in its turn, permanent aver- age hearing loss can be estimated to a certain extent from past measurement of noise exposure. The method consists of two stages. One is the critical band theory with respect to TTS, which deals with the spectral aspect of the exposure noise.