Aborigines and Torres Strait Islander People in the ACT
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Sumo Has Landed in Regional NSW! May 2021
Sumo has landed in Regional NSW! May 2021 Sumo has expanded into over a thousand new suburbs! Postcode Suburb Distributor 2580 BANNABY Essential 2580 BANNISTER Essential 2580 BAW BAW Essential 2580 BOXERS CREEK Essential 2580 BRISBANE GROVE Essential 2580 BUNGONIA Essential 2580 CARRICK Essential 2580 CHATSBURY Essential 2580 CURRAWANG Essential 2580 CURRAWEELA Essential 2580 GOLSPIE Essential 2580 GOULBURN Essential 2580 GREENWICH PARK Essential 2580 GUNDARY Essential 2580 JERRONG Essential 2580 KINGSDALE Essential 2580 LAKE BATHURST Essential 2580 LOWER BORO Essential 2580 MAYFIELD Essential 2580 MIDDLE ARM Essential 2580 MOUNT FAIRY Essential 2580 MOUNT WERONG Essential 2580 MUMMEL Essential 2580 MYRTLEVILLE Essential 2580 OALLEN Essential 2580 PALING YARDS Essential 2580 PARKESBOURNE Essential 2580 POMEROY Essential ©2021 ACN Inc. All rights reserved ACN Pacific Pty Ltd ABN 85 108 535 708 www.acn.com PF-1271 13.05.2021 Page 1 of 31 Sumo has landed in Regional NSW! May 2021 2580 QUIALIGO Essential 2580 RICHLANDS Essential 2580 ROSLYN Essential 2580 RUN-O-WATERS Essential 2580 STONEQUARRY Essential 2580 TARAGO Essential 2580 TARALGA Essential 2580 TARLO Essential 2580 TIRRANNAVILLE Essential 2580 TOWRANG Essential 2580 WAYO Essential 2580 WIARBOROUGH Essential 2580 WINDELLAMA Essential 2580 WOLLOGORANG Essential 2580 WOMBEYAN CAVES Essential 2580 WOODHOUSELEE Essential 2580 YALBRAITH Essential 2580 YARRA Essential 2581 BELLMOUNT FOREST Essential 2581 BEVENDALE Essential 2581 BIALA Essential 2581 BLAKNEY CREEK Essential 2581 BREADALBANE Essential 2581 BROADWAY Essential 2581 COLLECTOR Essential 2581 CULLERIN Essential 2581 DALTON Essential 2581 GUNNING Essential 2581 GURRUNDAH Essential 2581 LADE VALE Essential 2581 LAKE GEORGE Essential 2581 LERIDA Essential 2581 MERRILL Essential 2581 OOLONG Essential ©2021 ACN Inc. -
New Pipeline Opened Between Yass and Murrumbateman
Page 1 YASS VALLEY TIMES WEDNESDAY May 19, 2021 $2.00 New Pipeline Opened Between Yass and Murrumbateman Deputy Prime Minister Michael McCormack said consistent water supply for the growing community of Murrumbateman was a positive step in the right direction. “17.9 kilometres of pipeline from Yass to Murrumbateman to make sure that the water needs are served in a growing community.” With Yass water declared undrinkable at times by locals and a boil water alert issued within the last 12 months, the next comment from the Deputy Prime Minister may be harder for Murrumbateman residents to swallow. “The people of Murrumbateman deserve the same water quality as anyone else right around the country and of course especially when you’ve got a growing community and an additional demand on the water supply, to have the consistency of the water quality, to have indeed the volume of water that you need for a growing community,” McCormack said. State Member for Goulburn Wendy Tuckerman, said that whilst fixing some of the consistent issues with water remains a priority, the drought of recent times has reinforced the State Government’s commitment to water supply and security as the priority, particularly in regional communities. Federal Senator for NSW Perin Davey, NSW a $4.22 million contribution from Yass Valley Council. Minister for Water Property and Housing Melinda “That’s what I’m very impressed with is the focus on Pavey, Member for Goulburn Wendy Tuckerman, After a planning process that officially began in water security, obviously going through the drought Deputy Prime Minister Michael McCormack and we did recently, we need to do the work on the Mayor Rowena Abbey. -

Find Your Local Brigade
Find your local brigade Find your district based on the map and list below. Each local brigade is then listed alphabetically according to district and relevant fire control centre. 10 33 34 29 7 27 12 31 30 44 20 4 18 24 35 8 15 19 25 13 5 3 45 21 6 2 14 9 32 23 1 22 43 41 39 16 42 36 38 26 17 40 37 28 11 NSW RFS Districts 1 Bland/Temora 13 Hawkesbury 24 Mid Coast 35 Orana 2 Blue Mountains 14 Hornsby 25 Mid Lachlan Valley 36 Riverina 3 Canobolas 15 Hunter Valley 26 Mid Murray 37 Riverina Highlands 4 Castlereagh 16 Illawarra 27 Mid North Coast 38 Shoalhaven 5 Central Coast 17 Lake George 28 Monaro 39 South West Slopes 6 Chifley Lithgow 18 Liverpool Range 29 Namoi Gwydir 40 Southern Border 7 Clarence Valley 19 Lower Hunter 30 New England 41 Southern Highlands 8 Cudgegong 20 Lower North Coast 31 North West 42 Southern Tablelands 9 Cumberland 21 Lower Western 32 Northern Beaches 43 Sutherland 10 Far North Coast 22 Macarthur 33 Northern Rivers 44 Tamworth 11 Far South Coast 23 MIA 34 Northern Tablelands 45 The Hills 12 Far West Find your local brigade 1 Find your local brigade 1 Bland/Temora Springdale Kings Plains – Blayney Tara – Bectric Lyndhurst – Blayney Bland FCC Thanowring Mandurama Alleena Millthorpe Back Creek – Bland 2 Blue Mountains Neville Barmedman Blue Mountains FCC Newbridge Bland Creek Bell Panuara – Burnt Yards Blow Clear – Wamboyne Blackheath / Mt Victoria Tallwood Calleen – Girral Blaxland Cabonne FCD Clear Ridge Blue Mtns Group Support Baldry Gubbata Bullaburra Bocobra Kikiora-Anona Faulconbridge Boomey Kildary Glenbrook -
Bango Wind Farm IPCN Presentation
Bango Wind Farm Independent Planning Commission NSW Briefing Mike Young & Diana Mitchell March 2018 Contents 1. Project 2. Context 3. Engagement 4. Key Issues 5. Summary Project Regional Context • Southern Tablelands • Hilltops Council & Yass Valley Council • Between Yass and Boorowa • Bango Nature Reserve • Lachlan River Catchment 3 Project Regional Context 4 Project Local Setting • 5 km southwest of Rye Park village • 12 km southeast of Boorowa • 132 kV transmission lines • Residence located along Lachlan Valley Way, Tangmangaroo Road, Wargeila Road • Agricultural grazing land with rolling hills and gentle ridgelines 5 Project Amendments EIS Amended DA/RTS September 2016 May 2017 Number of wind 122 75 turbines Length of high voltage 9 km (up to 132kV) 5.5 km (up to 132 kV) overhead power line Number of site 2 2 substations Maximum tip height 200 m 200 m 6 Project Original Layout • 415 MW • 122 turbines • 3 clusters: o Langs Creek o Kangiara o Mt Buffalo • 200 m tip height 7 Project Revised Layout • 255 MW • 75 turbines • 2 clusters: o Kangiara o Mt Buffalo • 200 m tip height 8 Strategic Context • NSW Renewable Energy Action Plan • NSW Wind Energy Framework o Visual Assessment Bulletin o Noise Assessment Bulletin 9 Statutory Context • State Significant Development • Permissibility o Zoned RU1 – Primary Production o Permissible with consent under Boorow LEP 2012 o Prohibited under Yass Valley LEP 2013 o SEPP (Infrastructure) 2007 • Commonwealth approval 10 Project Benefits • 240 MW (71 turbines) o Generate 730 Gwh annually o Power 117,000 -
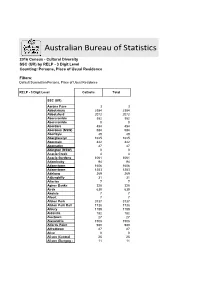
Australian Bureau of Statistics
Australian Bureau of Statistics 2016 Census - Cultural Diversity SSC (UR) by RELP - 3 Digit Level Counting: Persons, Place of Usual Residence Filters: Default Summation Persons, Place of Usual Residence RELP - 3 Digit Level Catholic Total SSC (UR) Aarons Pass 3 3 Abbotsbury 2384 2384 Abbotsford 2072 2072 Abercrombie 382 382 Abercrombie 0 0 Aberdare 454 454 Aberdeen (NSW) 584 584 Aberfoyle 49 49 Aberglasslyn 1625 1625 Abermain 442 442 Abernethy 47 47 Abington (NSW) 0 0 Acacia Creek 4 4 Acacia Gardens 1061 1061 Adaminaby 94 94 Adamstown 1606 1606 Adamstown 1253 1253 Adelong 269 269 Adjungbilly 31 31 Afterlee 7 7 Agnes Banks 328 328 Airds 630 630 Akolele 7 7 Albert 7 7 Albion Park 3737 3737 Albion Park Rail 1738 1738 Albury 1189 1189 Aldavilla 182 182 Alectown 27 27 Alexandria 1508 1508 Alfords Point 990 990 Alfredtown 27 27 Alice 0 0 Alison (Central 25 25 Alison (Dungog - 11 11 Allambie Heights 1970 1970 Allandale (NSW) 20 20 Allawah 971 971 Alleena 3 3 Allgomera 20 20 Allworth 35 35 Allynbrook 5 5 Alma Park 5 5 Alpine 30 30 Alstonvale 116 116 Alstonville 1177 1177 Alumy Creek 24 24 Amaroo (NSW) 15 15 Ambarvale 2105 2105 Amosfield 7 7 Anabranch North 0 0 Anabranch South 7 7 Anambah 4 4 Ando 17 17 Anembo 18 18 Angledale 30 30 Angledool 20 20 Anglers Reach 17 17 Angourie 42 42 Anna Bay 789 789 Annandale (NSW) 1976 1976 Annangrove 541 541 Appin (NSW) 841 841 Apple Tree Flat 11 11 Appleby 16 16 Appletree Flat 0 0 Apsley (NSW) 14 14 Arable 0 0 Arakoon 87 87 Araluen (NSW) 38 38 Aratula (NSW) 0 0 Arcadia (NSW) 403 403 Arcadia Vale 271 271 Ardglen -
Gazette No 68 of 13 June 2008
4773 Government Gazette OF THE STATE OF NEW SOUTH WALES Number 68 Friday, 13 June 2008 Published under authority by Government Advertising LEGISLATION Regulations New South Wales Fair Trading Amendment (Prams and Strollers) Regulation 2008 under the Fair Trading Act 1987 Her Excellency the Governor, with the advice of the Executive Council, has made the following Regulation under the Fair Trading Act 1987. LINDA BURNEY, M.P., MinisterMinister forfor FairFair Trading Trading Explanatory note The object of this Regulation is to amend the Fair Trading Regulation 2007 to prescribe a product safety standard for prams and strollers. The product safety standard prescribed is that prams and strollers must comply with certain provisions of the Australian/New Zealand Standard entitled AS/NZS 2088:2000, Prams and Strollers—Safety requirements. This Regulation is made under the Fair Trading Act 1987, including sections 26 and 92 (the general regulation-making power). s2007-415-32.d04 Page 1 4774 LEGISLATION 13 June 2008 Clause 1 Fair Trading Amendment (Prams and Strollers) Regulation 2008 Fair Trading Amendment (Prams and Strollers) Regulation 2008 under the Fair Trading Act 1987 1 Name of Regulation This Regulation is the Fair Trading Amendment (Prams and Strollers) Regulation 2008. 2 Commencement This Regulation commences on 1 July 2008. 3 Amendment of Fair Trading Regulation 2007 The Fair Trading Regulation 2007 is amended as set out in Schedule 1. Page 2 NEW SOUTH WALES GOVERNMENT GAZETTE No. 68 13 June 2008 LEGISLATION 4775 Fair Trading Amendment (Prams and Strollers) Regulation 2008 Amendment Schedule 1 Schedule 1 Amendment (Clause 3) Part 2, Division 15A Insert after Division 15: Division 15A Prams and strollers 52A Definitions In this Division: AS/NZS 2088 means the Australian/New Zealand Standard entitled AS/NZS 2088:2000, Prams and Strollers—Safety requirements published jointly by Standards Australia and Standards New Zealand on 15 December 2000. -
Boorowa River Catchment – an Overview
4. BOOROWA RIVER CATCHMENT – AN OVERVIEW 4.1 Location The Boorowa Catchment covers an area of about 2,200 km2 (220,000 ha) in the headwaters of the Lachlan River (Figure 1). The boundaries of the Boorowa Catchment Action Plan have been defined to include the area within Boorowa River sub-catchment (~1,820 km2) and Hovells Creek sub-catchment (~380 km2). This area represents about 2.5% of the Lachlan River Catchment, which covers an area of 84,700 km2. The north-south trending Catchment covers a length of about 85 km, and varies in width from roughly 30 km wide to less than 10 km wide near the Boorowa River junction with the Lachlan River, just below the Wyangala Dam. The Catchment straddles the boundary between the Southern Tablelands and South-Western Slopes regions of New South Wales. The centre of the Catchment lies about 110 kilometres NNW of Canberra, between the towns of Yass and Cowra. The southern boundary of the Catchment is located about 15 km north of Yass, and the northern outlet of the Catchment, about 20 km southwest of Cowra. The main town of Boorowa is located in the middle of the catchment, with the smaller villages of Frogmore and Rye Park are located in the eastern part of the catchment (Map 1). 4.2 History The original inhabitants of the Catchment were the Wallabalooa, who lived to the south of the Wiradjuri of the Lachlan River (Jackson-Nakano, 2002). The early explorers, Hamilton Hume, William Broughton and party, arrived in the area known as the Burrowa Plains in 1821. -

Region Localities Inclusion Support Agency New South Wales
u Inclusion and Professional Support Program (IPSP) Grant Application Process 2013-2016 Region Localities Inclusion Support Agency New South Wales This document lists the localities which comprise each Statistical Area Level 2 within each ISA Region in New South Wales. Description This document provides greater detail on the Australian Bureau of Statistics, Statistical Areal Level 2 boundaries within each ISA Region. The localities listed in this document are the ‘gazetted locality boundaries’ supplied by the state or territory government and may differ from commonly used locality and/or suburb names. This document does not provide a definitive list of every suburb included within each ISA Region as this information is not available. Postcodes are provided for those localities which either: cross ISA boundaries or where the same locality name appears in more than one ISA region within the same state or territory. IPSP 2013-2016: ISA Region Localities – New South Wales ISA Region 1 – Sydney Inner – Localities Alexandria Eastlakes Point Piper Annandale Edgecliff Port Botany Balmain Elizabeth Bay Potts Point Balmain East Enmore Pyrmont Banksmeadow (Postcode: 2042) Queens Park Barangaroo Erskineville Randwick Beaconsfield Eveleigh Redfern Bellevue Hill Forest Lodge Rose Bay Birchgrove Glebe Rosebery Bondi Haymarket Rozelle Bondi Beach Hillsdale Rushcutters Bay Bondi Junction Kensington South Coogee Botany Kingsford St Peters Bronte La Perouse Stanmore Camperdown Leichhardt Surry Hills Centennial -
Bango Wind Farm Project
Bango Wind Farm Project Traffic Management Plan 19 February 2021 _________________________________________________________ Contents 1. Introduction .................................................................................................. 1 1.1 Stakeholder Consultation................................................................................... 1 1.2 Scope and Methodology .................................................................................... 1 1.3 Conditions of Consent Requirements ................................................................ 2 1.4 Report Structure ................................................................................................ 5 2. Construction, Operation and Decommissioning ....................................... 6 2.1 Project Description ............................................................................................ 6 2.2 Construction and Decommissioning .................................................................. 6 3. Existing Road Network Conditions ............................................................ 8 3.1 Lachlan Valley Way ........................................................................................... 8 3.2 Tangmangaroo Road ......................................................................................... 8 4. Proposed Conditions ................................................................................. 10 4.1 Wind Farm Site Access Locations ................................................................... 10 -

The Working Miners of Southern New South Wales: Adaptability, Class and Identity
Journal of Australasian Mining History, Vol. 1, No. 1, September 2003. The Working Miners of Southern New South Wales: Adaptability, Class and Identity By BARRY McGOWAN Australian National University iners in the colonial and immediate post colonial period worked in one of three ways: on their own account, either independently or in co-operative M groups, or as wage employees for companies or syndicates. They also worked as tributers.1 The term ‘working miner’ was used by contemporary observers, and it will be used in this discussion to refer to all miners, including tributers, who were working on their own account or in co-operative groups. This paper examines the place of the working miners in the historiography and contemporary mining society, their identity and class, and the implications of this discussion for the wider historical discourse on the role of independent workers and labor organisations generally. The discussion falls into two parts. In the first part it is argued that miners generally should be viewed as part of a wider, more adaptable work force, and a number of examples of this adaptability are provided.2 It is concluded that the working miners, in particular, were considerably more prominent and persistent than most historians have realised. In the second part of the discussion the question of class and identity is discussed, in particular the argument that the working miners can be best described as subsistence miners. It is argued that such a definition is too limiting, and that it is more appropriate to apportion them to the middling class. Examples of working miners are derived from a number of mining fields in southern New South Wales, referred to thereafter as the Southern Mining Region, although evidence from other mining regions in Australia is also used. -

List of New South Wales Rural Fire Service Brigades
Article Talk Read Edit View history Search Wikipedia List of New South Wales Rural Fire Service brigades From Wikipedia, the free encyclopedia Main page This article needs more links to other articles to help integrate it into the encyclopedia. Contents Please help improve this article by adding links that are relevant to the context within the Featured content existing text. (April 2017) (Learn how and when to remove this template message) Current events Random article Brigades of the New South Wales Rural Fire Service Donate to Wikipedia Wikipedia store Contents [hide] Interaction 1 Listing by Rural Fire Service district 1.1 State Mitigation Support Services Bases Help About Wikipedia 1.2 Blue Mountains district Community portal 1.3 Lithgow district Recent changes 1.4 Cudgegong district Contact page 1.5 Cumberland zone 1.6 Far South Coast Team Tools 1.7 Central Coast District (Formerly The Lakes Team and Gosford District) What links here Related changes 1.8 Hawkesbury district Upload file 1.9 The Hills district Special pages 1.10 Hornsby / Ku-Ring-Gai district Permanent link 1.11 Illawarra zone Page information 1.12 Lake George zone Wikidata item 1.13 Macarthur zone Cite this page 1.14 MIA district Print/export Create PDF in your applications with the Pdfcrowd HTML to PDF API PDFCROWD Create a book 1.15 Mid Lachlan Valley team Download as PDF 1.16 Monaro Team Printable version 1.17 Snowy River district Languages 1.18 Riverina zone Add links 1.19 Southern Highlands team 1.20 Southern Tablelands zone 1.21 Sutherland district 1.22 Northern Beaches district 2 References Listing by Rural Fire Service district [ edit ] State Mitigation Support Services Bases [ edit ] Glenndening – HQ Blue Mountains district [ edit ] Stand alone district. -

Bango Wind Farm (SSD 6686)
STATE SIGNIFICANT DEVELOPMENT ASSESSMENT Bango Wind Farm (SSD 6686) Assessment Report Section 89E of the Environmental Planning and Assessment Act 1979 February 2018 Cover Photograph: Sourced from Green Bean Design Pty Ltd, Bango Wind Farm Landscape & Visual Impact Assessment, May 2016. © Crown copyright 2018 Published February 2018 NSW Department of Planning and Environment www.planning.nsw.gov.au Disclaimer: While every reasonable effort has been made to ensure that this document is correct at the time of publication, the State of New South Wales, its agents and employees, disclaim any and all liability to any person in respect of anything or the consequences of anything done or omitted to be done in reliance upon the whole or any part of this document Bango Wind Farm Assessment Report TABLE OF CONTENTS EXECUTIVE SUMMARY ................................................................................................................................ 1 1. Project ...................................................................................................................................................... 4 2. Strategic Context ................................................................................................................................... 10 2.1 Wind Energy ...................................................................................................................................... 10 2.2 Regional and Local Population ........................................................................................................