Interaction Between Health Institutions in Knowledge and Medical Practices in South Kordofan / Nuba Mountains
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Past, Present, and Future FIFTY YEARS of ANTHROPOLOGY in SUDAN
Past, present, and future FIFTY YEARS OF ANTHROPOLOGY IN SUDAN Munzoul A. M. Assal Musa Adam Abdul-Jalil Past, present, and future FIFTY YEARS OF ANTHROPOLOGY IN SUDAN Munzoul A. M. Assal Musa Adam Abdul-Jalil FIFTY YEARS OF ANTHROPOLOGY IN SUDAN: PAST, PRESENT, AND FUTURE Copyright © Chr. Michelsen Institute 2015. P.O. Box 6033 N-5892 Bergen Norway [email protected] Printed at Kai Hansen Trykkeri Kristiansand AS, Norway Cover photo: Liv Tønnessen Layout and design: Geir Årdal ISBN 978-82-8062-521-2 Contents Table of contents .............................................................................iii Notes on contributors ....................................................................vii Acknowledgements ...................................................................... xiii Preface ............................................................................................xv Chapter 1: Introduction Munzoul A. M. Assal and Musa Adam Abdul-Jalil ......................... 1 Chapter 2: The state of anthropology in the Sudan Abdel Ghaffar M. Ahmed .................................................................21 Chapter 3: Rethinking ethnicity: from Darfur to China and back—small events, big contexts Gunnar Haaland ........................................................................... 37 Chapter 4: Strategic movement: a key theme in Sudan anthropology Wendy James ................................................................................ 55 Chapter 5: Urbanisation and social change in the Sudan Fahima Zahir El-Sadaty ................................................................ -

SUDAN Livelihood Profiles, North Kordofan State August 2013
SUDAN Livelihood Profiles, North Kordofan State August 2013 FEWS NET FEWS NET is a USAID-funded activity. The content of this report does Washington not necessarily reflect the view of the United States Agency for [email protected] International Development or the United States Government. www.fews.net SUDAN Livelihood Profiles, North Kordofan State August 2013 TABLE OF CONTENTS Acknowledgements ................................................................................................................................................ 3 Acronyms and Abbreviations .................................................................................................................................. 4 Summary of Household Economy Approach Methodology ................................................................................... 5 The Household Economy Assessment in Sudan ..................................................................................................... 6 North Kordofan State Livelihood Profiling .............................................................................................................. 7 Overview of Rural Livelihoods in North Kordofan .................................................................................................. 8 Zone 1: Central Rainfed Millet and Sesame Agropastoral Zone (SD14) ............................................................... 10 Zone 2: Western Agropastoral Millet Zone (SD13) .............................................................................................. -
SUDAN Price Bulletin August 2021
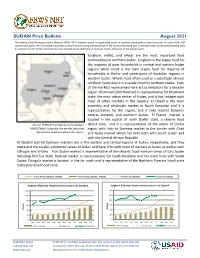
SUDAN Price Bulletin August 2021 The Famine Early Warning Systems Network (FEWS NET) monitors trends in staple food prices in countries vulnerable to food insecurity. For each FEWS NET country and region, the Price Bulletin provides a set of charts showing monthly prices in the current marketing year in selected urban centers and allowing users to compare current trends with both five-year average prices, indicative of seasonal trends, and prices in the previous year. Sorghum, millet, and wheat are the most important food commodities in northern Sudan. Sorghum is the staple food for the majority of poor households in central and eastern Sudan regions while millet is the main staple food for majority of households in Darfur and some parts of Kordofan regions in western Sudan. Wheat most often used as a substitute all over northern Sudan but it is a staple food for northern states. Each of the markets represented here act as indicators for a broader region. Khartoum (Om Durman) is representative for Khartoum state, the main urban center of Sudan, and it has linkages with most of other markets in the country. El Obeid is the main assembly and wholesale market in North Kordofan and it is representative for the region, and it links market between central, western, and southern Sudan. El Fasher market is located in the capital of north Darfur state, a chronic food Source: FEWS NET gratefully acknowledges deficit area, and it is representative of the entire of Darfur FAMIS/FMoA, Sudan for the market data and region with links to Geneina market in the border with Chad information used to produce this report. -

Sudan: West Kordofan - Who Does What Where (3Ws) 1 April 2018 Jebrat El Sheikh Sodari
Sudan: West Kordofan - Who Does What Where (3Ws) 1 April 2018 Jebrat El Sheikh Sodari 2(UN/IOs) Organizations per locality / per sector NORTH KORDOFAN (INGOs) El Kuma 2 No. of organizations per sector: < 5 5 - 10 11 - 20 > 20 No data Sodari 8(NNGOs) 12 Localities Sectors Level of needs O per locality Total number of organizations SRCS IOM, SRCS SRCS SRCS IOM, SOS Sahel, SRCS Bara D Low Map legend A No. of organizations B Medium A State capital Umm Keddada per locality High Primary towns Total El Nehoud ABU Z Primary/paved road < 5 Acute Locality boundary 5 - 10 - 1 2 1 - 1 - - 3 - 3 Umm Keddada KalimendoState Boundary El Obeid 11 - 20 Undetermined Boundary > 20 WEST No data SRCS SRCS SRCS GAH SRCS Badya, SOS Sahel Wad Banda D SRCS KORDOFAN Shiekan GLA Abu Zabad Wad Banda El Nehoud U NORTH Abu Zabad En Nehoud Um Rawaba Localities Sectors DARFUR YEI -M Total Ghubaysh B Al Sunut A - 1 1 1 1 1 2 - 1 - 4 El Taweisha Al Qoz SRCS SRCS SRCS SRCS SRCS El Salam Ghubaysh Babanusa Lagawa IOM IOM Al Sunut Rashad T Ailliet Dilling Total Ghubaysh Abyei - Muglad KHOWAI AL Dalami Abu Karinka Habila Keilak - 1 1 1 - 1 - - 1 - 1 El Fula SUNU L Ed Daein A Total SOUTH - - 1 - - - - - 1 - 1 Adila KORDOFAN Um Heitan El Salam SRCS SRCS SRCS SC-S SRCS SRCS Heiban A Assalaya I Ed Daein EAST Babanussa Lagawa Reif Ashargi SRCS SRCS SRCS SC-S SRCS SOS Sahel SECS, Y SRCS Y Babanusa A DARFUR Heiban D UN /IOs & INGOs staff no. -

(I): War in South Kordofan
Sudan’s Spreading Conflict (I): War in South Kordofan Africa Report N°198 | 14 February 2013 International Crisis Group Headquarters Avenue Louise 149 1050 Brussels, Belgium Tel: +32 2 502 90 38 Fax: +32 2 502 50 38 [email protected] Table of Contents Executive Summary ................................................................................................................... i Recommendations..................................................................................................................... iii I. Introduction ..................................................................................................................... 1 II. The Roots of Persistent Conflict ....................................................................................... 3 A. Continued Marginalisation ........................................................................................ 4 B. Changing Ethnic Dynamics ....................................................................................... 8 III. Failure of the CPA ............................................................................................................. 11 IV. Outbreak of Fighting and the Still-born Framework Agreement ................................... 17 V. All-Out Conflict ................................................................................................................ 20 VI. The Humanitarian Crisis .................................................................................................. 27 VII. Regional and Wider -

Welcome to Africa
WELCOME TO AFRICA Scientific Cooperation Network on Climate Change Adaptation STUDENTS EXCURSION 2 – 15 March 2013 „Summer School on Climate Change Adaptation” Khartoum / El-Obeid, Sudan Technische Universität Dresden Faculty of Environmental Sciences Institute of International Forestry and Forest Products PF 1117, 01735 Tharandt In the first two weeks of March 2013, while Germany was still covered in snow, the winter ended suddenly with a students’ excursion headed by Prof. Dr. Jürgen Pretzsch. Ten bachelor and master students of the TU Dresden travelled to Sudan thus to participate in the Summer School, which is part of the project “Scientific Cooperation Network on Climate Change Adaptation” and financed by the DAAD program “Welcome to Africa”. The workshop on “Climate Change Adaptation” took place in cooperation with the local partners, the University of Khartoum and the University of Kordofan. The Summer School workshop was held from 4th to 12th March in two Sudanese cities – Khartoum and El-Obeid. Day 1 (3rd March 2013) After a long but interesting trip, taken from Berlin to Khartoum, we were warmly welcomed to Sudan by Dr. Yahia Gumaa. He was always extraordinarily concerned to create our stay in Khartoum as agreeable as possible. Together with scientists from partner research institutes and universities in Ethiopia, Tanzania and Uganda, we stayed in the guest house of the University of Khartoum, which is very close to the campus of the Faculty of Forestry and right next to the river Nile. Sunday, the 3rd of March, was our first day in Khartoum and for some of us it was also the first day in Africa. -

Ldcs) for Adaptation to Climate Change (Clacc
CLACC Working Paper 5 CAPACITY STRENGTHENING IN THE LEAST DEVELOPED COUNTRIES (LDCS) FOR ADAPTATION TO CLIMATE CHANGE (CLACC) CLIMATE CHANGE AND HEALTH IN SUDAN SECS Hanan Ali, Sumaya Ahmed Zakieldeen, and Suad Sulaiman 2008 FOREWORD This study “Human Health and Climate Change” was carried out under the Capacity Strengthening of Least Developed Countries (LDCs) for Adaptation to Climate Change (CLACC) network. Primary objective of the study was to create awareness among the health professional in Sudan. We would like to thank the focal point for Climate change in Sudan at the Higher Council for Environment and Natural Resources (HCENR) for their support, advices and contribution. We are also grateful for Dr. Wsilat Zarwoog, Ministry of Health, Malaria Control Program, for her help and provision of information during the period of study. We are grateful to the Department for International Development (DFID) of the United Kingdom and the International Institute for Environment and Development (IIED-UK) for providing financial and technical assistance that has made this document possible. Page ii EXECUTIVE SUMMARY Sudan is a developing country and at the moment many developmental projects are being implemented. In the national strategies many major projects are also planned for the near future. Many of the these developmental projects (such as dams, agricultural projects) are likely to cause drastic changes in the environment (micro, meso, macro environment) and are likely, if not carefully managed, to encourage the spread of diseases (malaria, bilharzias etc.). The joint negative impacts of climate change and lack of development could be very dangerous and might threaten the health of a large number of people in the country. -

Health Care System in Sudan: Review and Analysis of Strength, Weakness, Opportunity, and Threats (SWOT Analysis) Ebrahim M
Sudan Journal of Medical Sciences Volume 12, Issue no. 3, DOI 10.18502/sjms.v12i3.924 Production and Hosting by Knowledge E Research Article Health Care System in Sudan: Review and Analysis of Strength, Weakness, Opportunity, and Threats (SWOT Analysis) Ebrahim M. A. Ebrahim1, Luam Ghebrehiwot, Tasneem Abdalgfar1, and Muhammad Hanafiah Juni2 1MPH (Master of Public Health) candidates, Department of Community Health, Faculty of Medicine and Health Sciences, Universiti Putra Malaysia 2Associate Professor, Department of Community Health, Faculty of Medicine and Health Sciences, Universiti Putra Malaysia Abstract Background: The Republic of the Sudan located in north-east of Africa and is considered to be a lower-middle income country. The country has well established healthcare system with many drawbacks mainly due to economic and managerial reasons followed by prolonged political instability and sanctions. Objective: The aim of this study is to give an insight over the health services system in Sudan and to analyze the strength, weakness, opportunities, and threats (SWOT). Materials and Methods: The search was done from two electronic databases: MEDLINE/Pubmed and from public search engines: Google Scholar and Google with key Search Corresponding Author: words used mainly as “Healthcare system in Sudan“. Additionally, SWOT analysis of Muhammad Hanafiah Juni; email: healthcare system in Sudan was carried out based on the Roemer’s model of health hanafi[email protected], service system. Results: The Sudanese healthcare system was analyzed for different Ebrahim M. A. Ebrahim; components of the system: The system in Sudan has full package of strategic plans email: dr.ibrahim.ibrahim@ and policies be it in a long term or short. -

Sudan National Human Development Report 2012
MWSS UNIVERSITY of GEZIRA SUDAN NATIONAL HUMAN DEVELOPMENT REPORT 2012 Geography of peace: Putting human development at the centre of peace in Sudan MWSS UNIVERSITY of GEZIRA SUDAN NATIONAL HUMAN DEVELOPMENT REPORT 2012 Geography of peace: Putting human development at the centre of peace in Sudan Copyright © 2012 By the United Nations Development Programme House 7, Block 5, Gamaá Avenue P.O. Box 913 Khartoum, SUDAN Website: www.sd.undp.org The designations employed and the presentation of material on the maps do not imply the expression of any opinion whatsoever on the part of the Secretariat of the United Nations or UNDP concerning the legal status of any country, territory, city or area or its authorities, or concerning the delimitation of its frontiers or boundaries. Design, layout and production by Phoenix Design Aid A/S, Denmark. ISO 14001/ISO 9000 certified and approved CO2 neutral company – www.phoenixdesignaid.com. Printed on environmentally friendly paper (without chlorine) with vegetable-based inks. The printed matter is recyclable. Printed in the European Union Cover page by Phoenix Design Aid A/S, Denmark Copyedit Angela Marie Stephen P.O. Box 4278 Washington, DC 20044-9278 The analysis and policy recommendations of the Report do not necessarily reflect the views of the United Nations Development Programme, its Executive Board, or its Member States or the Government of Sudan. The Report is an independent publication commissioned by UNDP SUDAN. It is the product of collaborative efforts by a team of independent consultants, -

Report for North Kordofan State
Socio-economic and opportunity mapping Assessment report for North Kordofan State Joint mission (NSDDRC NKS-SC / UNDP) 11th – 13th May 2010 Economic potentiality in North Kordofan state Socio-economic and opportunity mapping Assessment report for North Kordofan State Joint mission (NSDDRC-SC/ UNDP) Table of contents: Abstract (summary) State Back ground information Objectives Steps and Methods Employment opportunities Agriculture sector Socio-economic infrastructure Education and training providers UN Agencies and NGOs Need assessment for central sector commission Lesson learned and recommendations Annexes Socio-economic and opportunity mapping Assessment report for North Kordofan State Joint mission (NSDDRC-SC/ UNDP) Abstract (summary) North Kpordofan state is one of the target areas to be covered with Socio-economic opportunity mapping assessment for reintegration services. A team from UNDP central, North Kordofan Sector and central Sector Commission visited the state during the period from 11 th up to 13 th of May 2010. The main purpose of the assessment is to map out and identify the operational environment, institutional setup, community services, and socio-economic situation in the state which may enhance or impede implementation of reintegration activities also the gathered information will be used for better planning of DDR programme . The assessment will activate the already existing community sensitization about DDR programme and come up with recommendations and lesson learned on best strategy that could be adopted for DDR programme as well as assessing the availability of office sharing cost for the possible future placement of NDDRC/ North Kordofan Sector and UNDP/DDR Reintegration staff. The assessment team adopted different approaches for information collection and gathering such as presentation, observation, questionnaire, group discussion and individual interviews. -

Kalakla Turkish Hospital Sudan Kalakla Turkish Hospital
REPUBLIC OF TURKEY MINISTRY OF HEALTH DEPARTMENT OF FOREIGN AFFAIRS SUDAN KALAKLA TURKISH HOSPITAL SUDAN KALAKLA TURKISH HOSPITAL This book is published by the Ministry of Health i n 200 copies Ankara, 2007 ISBN 978-975-590-240- 1 MINISTRY PUBLICATION NO: 724 Prof. Dr. Nihat TOSUN Deputy Undersecretary, Ministry of Health Kamuran ÖZDEN Head of Department of Foreign Affairs, Ministry of Health Surgeon Dr. Adnan HASANOĞLU Sudan Coordinator / Ankara Training and Research Hospital, Deputy Chief Physician Sevim TEZEL AYDIN Deputy Head, Department of Foreign Affairs, Ministry of Health We believe the truth is the humanity, the truth is the love. In Fuzuli’s words: “ A k imi her ve var alemde, ilim bir kil-u kal imi ancak... If we start our journey in life with this pearl of wisdom, and if we dedicate ourselves in what we do, we will have the chance to wash away all the negativeness with the rains of happiness. Now, it is time for you to discover the chronology and photographs of the Sudan story of the Ministry of Health of the Republic of Turkey. Text and Redaction: Dr. Osman AYYILDIZ Memduh Atınç ATALAY - Director, Information Processing Division, Department of Foreign Affairs, Ministry of Health Translation: Beste Sultan GÜLGÜN, Department of Foreign Affairs, Ministry of Health 2 The mother in Darfur, whose son went to bed when hungry, the mother in Palestine crying over her son who cannot go to school as he lost his arm in a bomb explosion, the father somewhere in Africa who is in misery since he cannot access to medicine for his sick daughter…If they cannot be happy, we cannot sleep in serenity when they are not happy, until we will eliminate their problems and we cannot live in such a world in which peace does not exist. -

Inequalities in Public Services in the Sudan Using a Perceptions-Informed View to Drive Policy in Education, Health and Water Provision
Creative commons picture; Source: UNAMID (2014) Inequalities in Public Services in the Sudan Using a perceptions-informed view to drive policy in education, health and water provision LSE Master of Public Administration (MPA) Capstone Report March 13, 2014 Client: DFID Sudan Authors: Naomi Crowther, Keisuke Okamura, Chandni Raja, David Rinnert, Ella Spencer Advisors: Professor Patrick Dunleavy (LSE), Dr. Alexander Hamilton (DFID Sudan), Dr. Kostas Matakos (LSE) Fall 08 Chapter 1 Introduction This report was produced on behalf of DFID Sudan as part of the Master of Public Administration (MPA) programme Capstone project. The authors are indebted to Professor Patrick Dunleavy and Dr. Kostas Matakos for their continued academic support, to Dr. Alexander Hamilton and DFID Sudan for their invaluable time and continued support and to the experts who were interviewed in the writing of this report. Map of Sudan Figure 1 - Map of Sudan. Source: Authors of this report, using creative commons sources from Wikimedia Commons. The choropleth maps within this report were created using GIS data from the GADM spatial database and reflect data from March 2009. We were not able to access more recent data. As is clear from the map, this data does not reflect changes made to the boundaries of Sudanese states following 2005; specifically, West Kordofan was abolished in 2005 and incorporated into North and South Kordofan, but appears in our choropleth maps as a state. This area is shown in white, it can be assumed that the data for this area was collected and is captured within North and South Kordofan. With respect to Darfur, our GIS data reflects the borders when the region was comprised of three states: North, South, and West Darfur, and the DFID 2012 and 2013 household survey data also report responses in these terms.