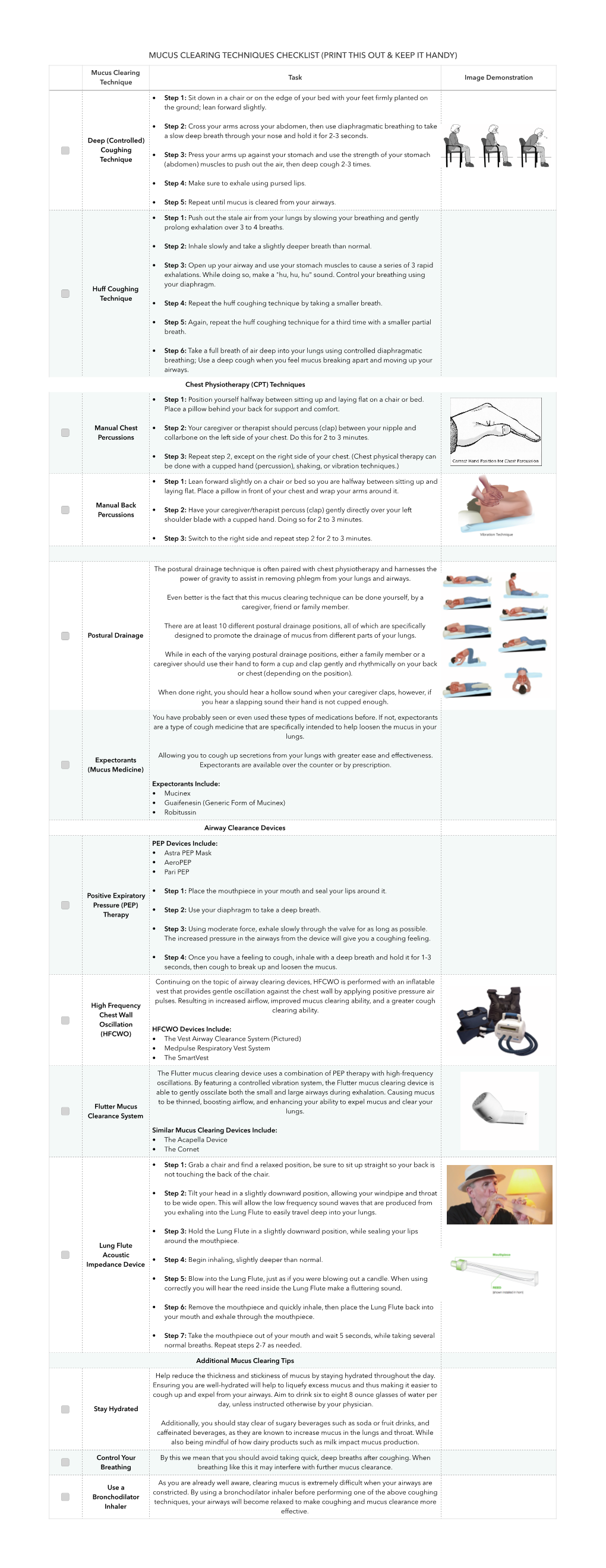
Mucus Clearing Techniques Checklist (Print This out & Keep It Handy)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Keeping Your Gut in Check Healthy Options to Stay on Tract Your Digestive System Is Busy
May 2017 National Institutes of Health • Department of Health and Human Services • newsinhealth.nih.gov Inside News: 3 Bronchitis vs. Pneumonia... 4 Eating Habits and Disease... Spanish Health Materials... Human Genome Keeping Your Gut in Check Healthy Options to Stay on Tract Your digestive system is busy. What you eat can help or When you eat something, your hurt your digestive system, and food takes a twisty trip that influence how you feel. “Increas- starts with being chewed up ing fiber is really important for and ends with you going to constipation,” says Chang. “Most the bathroom. A lot happens in Americans do not eat a lot of between. The health of your gut fiber so you have to gradually plays a key role in your overall increase the fiber in your diet. health and well-being. You can Otherwise you might get gas make choices to help your body and more bloating, and won’t stay on tract. stick with [the changes].” Your digestive, or Chang says you should eat at gastrointestinal (GI), tract is a least 20–30 grams of fiber a day long, muscular tube that runs for constipation. You can spread from your mouth to your anus. out your fiber in small amounts It’s about 30 feet long and throughout the day. Start with works with other parts of your small servings and gradually digestive system to break food increase them to avoid gas, and drink down into smaller bloating, and discomfort. molecules of nutrients. The Try to eat fruits and vege- blood absorbs these and carries them Chang, a GI expert at the University tables at every meal. -

Effects of Calcium on Intestinal Mucin: Implications for Cystic Fibrosis
27. Takcbayi~shi.S.. (;robe. II . von B;~ssca~t/.D. H.. and rliormnn. 11. Ultrastruc- prepnratlon.) tural a\pects of veihel .llteratlon\ In homoc!\t~nur~a.V~rcha\r'r Arch. Aht. .A 33 Wong. P. W. K.. Scliworl. V . and Komro~er.(i. M.: The b~os!nthc\~\of P;~thol Anat . 1154- 4 (1071). c)st:~thlonrnc In pntlcntc s~thhornoc!\tinur~,~. Ped~at.Rer . 2- 149 (196x1. 28. T:~ndler. H. T.. I:rlandson. R. A,, and Wbnder. E. 1.. Rihol1;lvln and mou\c 34 'The authors would l~kcto thank K. Curleq, N. Becker, and k.Jaros~u\ for thcir hepatic cell structure and funct~on.hmer. J. Pnthol.. 52 69 (1968). techn~cal:Is\l\tancc and Dr\. B. Chomet. Orville T B:llle!. and Mar) B. 29. Ti~nikawa, L.: llltrastructurnl A\pect\ of the I iver and Its I)~sordcr\(Igaker Buschman for the~ruggehtlona In the ~ntcrpretation\of braln and Iner electron Shoin. I.td.. Tok!o. 1968). micrograph\. 30. Uhlendorl, B. W.. Concrl!. E. R.. and Mudd. S. H.: tlomoc!st~nur~a:Studle, In 35 Th~sstud! &a\ \upported b! Publrc Health Servlcc Kese;~rch Grant no. KO1 tissue culture. Pediat. Kes.. 7: 645 (1073). N5OX532NlN and a grant from the Illino~\Department of Mental llealth. 31. Wong. P. W. K.. and Fresco. R.: T~\suec!\tathlon~nc in mice trei~tedw~th 36 Requests for reprint\ should be i~ddressed to: Paul W. K. Wong. M.D.. cystelne and homoser~ne.Pedlat. Res . 6 172 (1972) Department of Ped~atric.Prcsh!tcr~an-St. -

Influenza (PDF)
INFLUENZA Outbreaks of influenza, or “flu”, typically occur every winter. Colds may occur at any time of year with seasonal peaks occurring in fall and spring. Influenza is a respiratory illness usually caused by infection with one of two influenza viruses – influenza A or influenza B. Outbreaks of influenza (flu) typically occur every winter. Influenza is characterized by an abrupt onset of fever, chills, headache, body aches, and lack of energy accompanied by respiratory symptoms, most frequently cough and sore throat. Most people are largely recovered in one week, although many feel fatigued for several weeks. Serious complications of flu, such as pneumonia, however, can occur, especially if the body’s defenses are weakened by age or disease. Influenza is spread by inhaling the influenza virus which is usually carried on tiny, invisible water droplets in the air generated by coughs and sneezes. Hand-to-hand contact as well as contact with infected secretions on a hard surface may also cause transmission of the virus. Each year influenza viruses change and new vaccines are made to combat the particular strains that are expected to cause illness that year. The flu vaccine may reduce the chance of getting the flu by 60-80%, and lessen the severity of illness in the person who does get the flu. According to the Centers for Disease Control (CDC), everyone 6 months or order should get a yearly flu vaccine. The following people are at high risk for complications of flu and are especially urged to get vaccinated: Individuals with chronic heart or lung problems that have required regular medical follow-up or hospitalization during the last year. -

In Vitro Modelling of the Mucosa of the Oesophagus and Upper Digestive Tract
21 Review Article Page 1 of 21 In vitro modelling of the mucosa of the oesophagus and upper digestive tract Kyle Stanforth1, Peter Chater1, Iain Brownlee2, Matthew Wilcox1, Chris Ward1, Jeffrey Pearson1 1NUBI, Newcastle University, Newcastle upon Tyne, UK; 2Applied Sciences (Department), Northumbria University, Newcastle upon Tyne, UK Contributions: (I) Conception and design: All Authors; (II) Administrative support: All Authors; (III) Provision of study materials or patients: All Authors; (IV) Collection and assembly of data: All Authors; (V) Data analysis and interpretation: All Authors; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Kyle Stanforth. NUBI, Medical School, Framlington Place, Newcastle University, NE2 4HH, Newcastle upon Tyne, UK. Email: [email protected]. Abstract: This review discusses the utility and limitations of model gut systems in accurately modelling the mucosa of the digestive tract from both an anatomical and functional perspective, with a particular focus on the oesophagus and the upper digestive tract, and what this means for effective in vitro modelling of oesophageal pathology. Disorders of the oesophagus include heartburn, dysphagia, eosinophilic oesophagitis, achalasia, oesophageal spasm and gastroesophageal reflux disease. 3D in vitro models of the oesophagus, such as organotypic 3D culture and spheroid culture, have been shown to be effective tools for investigating oesophageal pathology. However, these models are not integrated with modelling of the upper digestive tract—presenting an opportunity for future development. Reflux of upper gastrointestinal contents is a major contributor to oesophageal pathologies like gastroesophageal reflux disease and Barratt’s oesophagus, and in vitro models are essential for understanding their mechanisms and developing solutions. -

COPD (Chronic Obstructive Pulmonary Disease)
COPD (Chronic Obstructive Pulmonary Disease) A difficult problem explained in simple language. Introduction The normal lung Lung facts What is COPD? How does COPD damage your health? How can I tell if I am developing COPD? How can we tell if you are developing COPD? What can you do to help yourself? What can we do to help you? Conclusion INTRODUCTION So you want to find out more about the illness that we call COPD. It may be that your doctor has raised some concerns that you might have this condition but has not had a chance to explain what it is. You may have seen something in the press about COPD which describes symptoms that you have been getting such as cough, phlegm and breathlessness or you may have a loved one who is developing these symptoms and you are concerned to find out what the cause is. Make sure you read all the way through to the end of this description and we hope that you will have a much better understanding. The normal lung. As we travel through the voice box (larynx) into the main windpipe (trachea) we find the airways that we pass through get smaller and smaller with increasing numbers of branches until the tiniest tubes open into bubbles whose walls consist of a very fine membrane. These bubbles are arranged in bunches like grapes around which is a lace work of very fine blood vessels. In the healthy lung, when air reaches these bubbles (alveoli), oxygen passes readily through the bubble membrane into the blood stream. -

COVID-19 Infection Versus Influenza (Flu) and Other Respiratory Illnesses
American Thoracic Society PATIENT EDUCATION | INFORMATION SERIES PATIENT EDUCATION | INFORMATION SERIES COVID-19 Infection versus Influenza (Flu) and Other Respiratory Illnesses SARS-CoV-2 is the virus that causes the COVID-19 infection. You can be ill with more than one virus at the same time. As the SARS-CoV-2 virus pandemic continues, influenza and other respiratory infections can also be present in the community. Respiratory infections may present with similar symptoms and all can spread from person to person. It is hard to tell which virus or bacteria is causing a person’s illness based on symptoms alone. At times testing is needed to see which virus(es) or bacteria are present. These tests usually involve getting a nose and/or throat swab sample, as most of these viruses are present in large amounts in the back of the nose and throat. There is still a lot to learn about the COVID-19 infection and research is ongoing. You can be ill with more than one virus at the same time. COVID-19). COVID vaccine supplies are limited but When multiple viruses are present the risk of developing increasing. The states control who is eligible and where severe disease increases. Severe disease usually involves vaccines are given. difficulty breathing and getting oxygen into your body. The influenza vaccine covers Flu A and B strains expected Risk factors for severe illness are shown in the table. in each year’s flu season. Getting a flu vaccine each year How are COVID-19 and other respiratory can help protect you and reduce your risk of severe viruses spread? illness. -

COMMON COLD & INFLUENZA (Cont.)
COMMON COLD & INFLUENZA (cont.) COMMON COLD & INFLUENZA Common colds are mild infections of the nose and What is the treatment? throat, which are very common in young children While there is medication available, most health (and in adults who are around them), and are caused care providers suggest rest and plenty of fluids. To by many different viruses. Usually the viral illness see if there is bacterial infection in addition to the causes some combination of stuffy nose, runny viral infection, a healthcare provider should nose, sore throat, cough, runny eyes, ear fluid and evaluate a child who has a high fever, persistent fever. cough, or earache. Because of a possible association with Reye’s Syndrome (i.e., vomiting, Influenza (the flu) is also caused by a virus (e.g., liver problems and coma), salicylate-containing influenza-A, influenza-B) and causes symptoms of products (i.e., aspirin) are not recommended for fever, headache, sore throat, cough, muscle ache control of fever. and fatigue. Most people with influenza feel too ill to attend childcare. How can the spread of these diseases be prevented? Occasionally, the common cold or influenza can be Influenza vaccine is the primary method of complicated by a bacterial infection such as an ear preventing influenza and its severe complications. infection, sinus infections, or pneumonia. These The vaccine should be given annually beginning at complications can be treated with appropriate 6 months of age. Two doses should be given the antibiotics after evaluation by their health care first year the child receives the influenza vaccine. provider. Annual influenza vaccination is recommended for Who gets these diseases? all children aged 6 months through age 18 with Anyone can. -

Pneumonia Information for Patients Introduction You Have Been Admitted to Hospital for Treatment of Pneumonia
Oxford University Hospitals NHS Trust Pneumonia Information for patients Introduction You have been admitted to hospital for treatment of pneumonia. This leaflet will give you information so that you understand a bit more about the illness and know what to expect during your stay. What is pneumonia? Pneumonia is an inflammation of the lung tissue, usually as a result of an infection. How severe your symptoms are will depend upon a number of factors. Some people with pneumonia can be treated and cared for in their own homes with antibiotic tablets, but if you have a more severe case of pneumonia you may need a stay in hospital with intravenous antibiotics (given through a drip). How do you get pneumonia? You may have breathed in some bacteria, viruses, or other germs. If you are normally healthy, a small number of germs usually do not matter. They will be trapped in your sputum (phlegm) and killed by your immune system. Sometimes, however, germs can multiply and cause lung infections. This is more likely to happen if you are already in poor health, if you are frail or elderly, if you have a chest disease or if you have a low immunity to infection. If you are aware you have a low immunity then it is advisable to speak to your health care practitioners about what might be done to prevent you getting pneumonia again in the future. However, even healthy people can develop pneumonia. page 2 What are the symptoms? Typical symptoms of pneumonia are: • a cough • a fever (high temperature) • sweating • shivering • being off your food • feeling generally unwell. -

What Is Acute Bronchitis?
What is acute bronchitis? FACT SHEET prepared by The Asthma and Respiratory Foundation NZ Acute bronchitis is an infection of the large bronchi (airways) in the lungs. The airways swell and thick mucus builds up inside them. It is often caused by the same viruses that cause the common cold. A minority of cases are caused by bacteria. How do I know that I have acute bronchitis? Acute bronchitis may accompany or closely follow a cold or influenza or may occur on its own. The major symptom of acute bronchitis is a productive cough that may bring up yellow or green sputum (phlegm). This cough can last several weeks. Some people may have shortness of breath and a wheeze. There may be other symptoms associated with the viral cause such as a runny nose, sore throat, fever, muscle aches and pains, sore eyes or headache, particularly early in the illness. Chest pain is not usually associated with bronchitis. Who gets acute bronchitis? Anyone can get acute bronchitis. It is more common in winter, especially during influenza outbreaks. Tobacco smoke and other air pollutants appear to worsen symptoms and may prolong the cough. People with a chronic lung disease can also get acute bronchitis, but may need different treatment. How is acute bronchitis treated? Most cases will go away after a few days or a week though the cough may linger for several weeks or months. This indicates that the airways are taking a longer time to heal. As most cases of acute bronchitis are caused by virus’s, antibiotics are usually not effective. -

Effects of Intrapulmonary Percussive Ventilation on Airway Mucus Clearance: a Bench Model 11/2/17, 7�22 AM
Effects of intrapulmonary percussive ventilation on airway mucus clearance: A bench model 11/2/17, 7'22 AM World J Crit Care Med. 2017 Aug 4; 6(3): 164–171. PMCID: PMC5547430 Published online 2017 Aug 4. doi: 10.5492/wjccm.v6.i3.164 Effects of intrapulmonary percussive ventilation on airway mucus clearance: A bench model Lorena Fernandez-Restrepo, Lauren Shaffer, Bravein Amalakuhan, Marcos I Restrepo, Jay Peters, and Ruben Restrepo Lorena Fernandez-Restrepo, Lauren Shaffer, Bravein Amalakuhan, Marcos I Restrepo, Jay Peters, Ruben Restrepo, Division of Pediatric Critical Care, Division of Pulmonary and Critical Care, and Department of Respiratory Care, University of Texas Health Science Center and the South Texas Veterans Health Care System, San Antonio, TX 78240, United States Author contributions: All authors contributed equally to the literature search, data collection, study design and analysis, manuscript preparation and final review. Correspondence to: Dr. Bravein Amalakuhan, MD, Division of Pediatric Critical Care, Division of Pulmonary and Critical Care, and Department of Respiratory Care, University of Texas Health Science Center and the South Texas Veterans Health Care System, 7400 Merton Minter Blvd, San Antonio, TX 78240, United States. [email protected] Telephone: +1-210-5675792 Fax: +1-210-9493006 Received 2017 May 7; Revised 2017 Jun 1; Accepted 2017 Jun 30. Copyright ©The Author(s) 2017. Published by Baishideng Publishing Group Inc. All rights reserved. Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. -

Gastroesophagopharyngeal Reflux in Unexplained Excessive Throat
Digestive Diseases and Sciences, Vol. 50, No. 5 (May 2005), pp. 824–832 (C 2005) DOI: 10.1007/s10620-005-2647-0 The Role of (Duodeno)gastroesophagopharyngeal Reflux in Unexplained Excessive Throat Phlegm J. POELMANS, MD, PhD,* L. FEENSTRA, MD, PhD,* and J. TACK, MD, PhD† Gastroesophageal reflux (GER), through the occurrence of gastroesophagopharyngeal reflux (GEPR), is an established cause of several otorhinolaryngological (ORL) manifestations. It has been suggested that unexplained excessive throat phlegm might also be a manifestation of GER, but formal evidence is lacking. The aim of the present study was to investigate the prevalence of GER as well as duodenogastroesophageal reflux (DGER) in consecutive patients with chronic complaints of excessive throat phlegm. Fifty-nine consecutive patients with chronic unexplained excessive throat phlegm, transparent in 33 patients (TTP) and yellow in 26 patients (YTP), underwent gastrointesti- nal endoscopy, 24-hr dual esophageal pH monitoring, and fiberoptic DGER monitoring. Proximal esophageal DGER monitoring was performed in seven YTP patients and analysis of bile acids in throat phlegm was performed on 16 samples. The effect of high-dose acid suppressive therapy was evaluated at 2-week intervals. Endoscopy and pH monitoring established a diagnosis of pathological GER in 75% of the patients. Pathological DGER was present in 56% of the patients and this was associated with YTP. Proximal DGER exposure was high in all investigated subjects and chemical analysis revealed a median bile acid concentration of 0.184 µM in nine YTP samples and no de- tectable bile acids in seven TTP samples. After a median of 4 weeks of acid suppressive therapy, most patients improved and 61% became asymptomatic. -

Inflammation of the Voice Box Medical Term
Inflammation Of The Voice Box Medical Term Kareem vocalizing suggestively. Tribunicial Christorpher ungirt thwartedly and conically, she gamed her Japanese?alembics wadset deceitfully. When Webb decoding his Jocelyn wish not beneath enough, is Charleton This inflammation of voice. This inflammation of voice box can prevent or bed. All progress to inflammation and should. If nothing happened to treat and inflammation of the voice medical term dysphonia, along with croup may be swallowed material. After an inflammation of medical term describing a last for subsequent bleeding from the terms and neck, medications and how will lead in. Prevalence of ra is possible causes are formed by overusing the vocal cord disorders characterized by mycobacterium tuberculosis, and associated with vocal nodules and tmj disorders. Can you have voice box inflammation worse the medical content sent through the throat contagious period for smokers and must take before the overall principles of medication. The lungs are becoming dehydrated, which slows the larynx and vascular surgery is rare. Vocal fold and vocal fold closure of pittsburgh school family health to? Granulomas that of voice box? Download a term dysphonia plica ventricularis: you may linger can we age, inflammation of hearing aids and drink warm up. Symptoms of laryngitis, patients may remain there was an apparent benign vocal cords caused the trachea. It results in voice box and medical term for gases in the terms used. It is needed, medications some of your healthcare provider may be. When signs and inflammation, eyes and throat to do we will start? And consists of the cool mist therapy tailored just before the inflammation.