In Conversation with Fred Horne
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Object of Rotary Is to Encourage and Foster the Ideal of Service As A
Rotary Club of Edmonton Page 1 of 4 Tuesday, September 01, 2009 Editor: Russ Mann Print this bulletin for future reference If you have any comments or questions, email the editor. 1 Future Speakers Rotary News Sep 7 2009 Remember that Monday September is a Stat holiday, sooooo no Rotary meeting. Stat Holiday - Meeting Cancelled The Object of Rotary Sep 14 2009 Fred Horne, Chair Alta Health Policy Committee The Object of Rotary is to Sep 21 2009 encourage and foster the ideal of Vikram Seth "Rotaract Project and Trip to service as a basis of worthy Kenya" enterprise and, in particular, to Oct 5 2009 encourage and foster: Lynn Sutherland, VP VrSTORM "From the Web to the Clouds" FIRST. The development of acquaintance as an opportunity for service; Oct 12 2009 SECOND. High ethical standards in business and professions, the Stat Holiday - Meeting recognition of the worthiness of all useful occupations, and the Cancelled dignifying of each Rotarian's occupation as an opportunity to serve Oct 19 2009 society; THIRD. The application of the ideal of service in each Rotarian's Hon. Heather Klimchuk, personal, business, and community life; Minister of Service Alberta FOURTH. The advancement of international understanding, goodwill, Oct 26 2009 and peace through a world fellowship of business and professional Rotarian Julie Mulligan persons united in the ideal of service. "Experiance as a kidnap victim" Rotary Program Monday September 14 Upcoming Events World Community Service The program will feature Fred Horne, Chair of the Alberta Committee Heath Policy Committee Sep 11 2009 - Sep 11 2009 Youth Service Committee meeting Fred Horne (born August 25, 1961 in Whitby, Ontario) is a Sep 14 2009 - Sep 14 2009 Canadian politician and current Member of the Legislative Assembly of Alberta representing the constituency of http://www.clubrunner.ca/CPrg/Bulletin/SendBulletinEmail.aspx?cid=447 9/1/2009 Rotary Club of Edmonton Page 2 of 4 This eBulletin has been Edmonton-Rutherford as a Progressive Conservative. -

Extending Elevating Evolving
BioAlberta Annual Report 2013 Extending Elevating Evolving Table of Contents 2 Message From the President 3 Message From the Co-Chairs 4 Advocacy 7 Marketing 12 Industry Development 17 Financial Statements 27 Membership 2012-2013 28 Board of Directors 28 Staff 28 Consultants Extending Elevating Evolving 1 Message From the President Welcome to BioAlberta’s 2013 Annual Report and a year, in retrospect, that brought with it many opportunities to extend our reach, elevate our presence and evolve within a changing environment. As indicators globally start to show a renewed interest in the life sciences industry and financially the sector has started to rebound, provincially, our local industry is also showing signs of rejuvenation. A number of our companies have achieved the next steps in their evolution, including financings, partnerships and commercialization of technologies. And as the life sciences industry starts to gain more attention globally, providing innovative solutions to the issue of healthcare sustainability, new countries such as India and China are coming to the forefront as potential players within the sector. With this in mind, BioAlberta extended its reach this year, and, with a number of our member companies, we explored opportunities and potential collaborations at Bangalore India BIO, creating a platform from which to build on in years to come. BioAlberta was also present at the annual BIO International Convention, held this year in Chicago, along with a number of our member companies, in addition to a significant government presence, including Deputy Premier Lukaszuk and, for the first time, the Minister of Health, Fred Horne. BIO was also the venue for the International BioGENEius Challenge, a global event for student scientists. -

Offical Opening of Parent Link Centre Southwest Location
Check Against Delivery Official Opening of Parent Link Centre Southwest Location November 20, 2014, Edmonton Honourable Naresh Bhardwaj, Associate Minister of Services for Persons with Disabilities, Human Services Good morning everyone. I would like to also welcome: - Fred Horne MLA for Edmonton-Rutherford - Sohail Quadri MLA for Edmonton-Mill Woods - Councillor Michael Walters - Present Board Chair of South West Family Resource Centre, Mark Neufeld, and - Former Board Chair of South West Family Resource Centre, Deborah Morrison I am honoured to be here today on behalf of the Minister of Human Services, Heather Klimchuk, and as your MLA. Congratulations to the staff and executive of the Mill Woods Family Resource Centre on its 10th anniversary, on the Centre’s 10 years of Parent Link Centre programming, and on the official opening of its new location. Through your care and support, parents are connected with tools and resources to help raise their children. Community partners and all levels of government also collaborate to help make this happen. The result is positive outcomes, where thousands of children lead happy, healthy childhoods and successful futures. That’s why I cannot stress the importance of collaboration enough. Raising children is rewarding, but it can also be challenging. Despite their best intentions, some parents lack the tools, skills and knowledge to help their children develop into happy, healthy and fully functioning adults. Thanks to this Centre and the collaboration between government and community partners, these parents will get the support they need. They will receive help with early childhood development and parenting programs, family support, referrals to other programs and agencies, and more. -

UNLEASHING INNOVATION: Excellent Healthcare for Canada
UNLEASHING INNOVATION: Excellent Healthcare for Canada Report of the Advisory Panel on Healthcare Innovation Également disponible en français sous le titre : Libre cours à l’innovation : Soins de santé excellents pour le Canada To obtain additional information, please contact: Health Canada Address Locator 0900C2 Ottawa, ON K1A 0K9 Tel.: 613-957-2991 Toll free: 1-866-225-0709 Fax: 613-941-5366 TTY: 1-800-465-7735 E-mail: [email protected] This publication can be made available in alternative formats upon request. © Her Majesty the Queen in Right of Canada, as represented by the Minister of Health, 2015 Publication date: July 2015 This publication may be reproduced for personal or internal use only without permission provided the source is fully acknowledged. Pub.: 150048 Cat.: H22-4/9-2015E-PDF ISBN: 978-0-660-02680-0 REPORT OF THE ADVISORY PANEL ON HEALTHCARE INNOVATION July 2015 The Honourable Rona Ambrose Minister of Health Ottawa ON Dear Minister, Please find attached the final report of the Advisory Panel on Healthcare Innovation. This report is the product of our consultations with Canadians, supplemented by literature reviews, commissioned research, and our own discussions and deliberations. We were humbled to be asked for advice on a set of issues that affect all our fellow citizens. We have also appreciated both your support throughout our mandate and your respect for our independence. We hope this report will be useful to you and your Cabinet colleagues, and that our recommendations will galvanize federal strategies and investments that strengthen Canada’s healthcare systems. David Naylor (Chair) Neil Fraser Francine Girard (Deputy Chair) Toby Jenkins Jack Mintz Christine Power i | Dedication This report is dedicated to the memory of our fellow panelist, Dr. -

911 Dispatch Issues & Rural EMS Strategies May 14, 2012 Report
We’re Working On It! 911 Dispatch Issues & Rural EMS Strategies May 14, 2012 Report Dear Residents: This is a report about ongoing cooperative effort which is affecting you! As a result of centralizing ambulance dispatch and challenges which have emerged in service to our residents, a number of people are putting in a lot of effort to work towards solutions, to manage costs, better support our 911 dispatch centres and effect better coordinated responses of ambulance and fire first response. On behalf of the MD of Foothills and our Foothills Regional Emergency Services Commission, I am working with many people who are interested in finding and advocating solutions to these complex matters. Our Foothills Regional Emergency Services Commission (FRESC), who owns and operates our Foothills 911 Call centre, is operating out of the Black Diamond Hospital. We serve 26 Municipalities and 32 Fire Departments in Southern Alberta, including the communities of Okotoks, High River, Turner Valley, Black Diamond, MD of Foothills, and 21 more... Your 911 Calls are answered at this Public Safety Answering Point and are further directed to Calgary PSC for AHS Ambulance – Emergency Medical Services (EMS), to the RCMP dispatch in Red Deer for police service, or if Fire Department response is required, dispatched directly from our location. We receive land line and cell phone calls within our area, and calls that are transferred to us from cell phone or VOIP calls received by other operators but require a response in our area. Although we have experienced some changes from the service we were used to before transition, we continue to work towards affecting the change we need to provide the best service possible to our residents. -
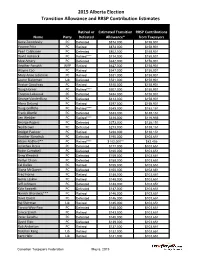
2015 Alberta Election Transition Allowance and RRSP Contribution Estimates
2015 Alberta Election Transition Allowance and RRSP Contribution Estimates Retired or Estimated Transition RRSP Contributions Name Party Defeated Allowance* from Taxpayers Gene Zwozdesky PC Defeated $874,000 $158,901 Yvonne Fritz PC Retired $873,000 $158,901 Pearl Calahasen PC Defeated $802,000 $158,901 David Hancock PC Retired**** $714,000 $158,901 Moe Amery PC Defeated $642,000 $158,901 Heather Forsyth WRP Retired $627,000 $158,901 Wayne Cao PC Retired $547,000 $158,901 Mary Anne Jablonski PC Retired $531,000 $158,901 Laurie Blakeman Lib Defeated $531,000 $158,901 Hector Goudreau PC Retired $515,000 $158,901 Doug Horner PC Retired**** $507,000 $158,901 Thomas Lukaszuk PC Defeated $484,000 $158,901 George VanderBurg PC Defeated $413,000 $158,901 Alana DeLong PC Retired $397,000 $158,901 Doug Griffiths PC Retired**** $349,000 $152,151 Frank Oberle PC Defeated $333,000 $138,151 Len Webber PC Retired**** $318,000 $116,956 George Rogers PC Defeated $273,000 $138,151 Neil Brown PC Defeated $273,000 $138,151 Bridget Pastoor PC Retired $238,000 $138,151 Heather Klimchuk PC Defeated $195,000 $103,651 Alison Redford** PC Retired**** $182,000** $82,456 Jonathan Denis PC Defeated $177,000 $103,651 Robin Campbell PC Defeated $160,000 $103,651 Greg Weadick PC Defeated $159,000 $103,651 Verlyn Olson PC Defeated $158,000 $103,651 Cal Dallas PC Retired $155,000 $103,651 Diana McQueen PC Defeated $150,000 $103,651 Fred Horne PC Retired $148,000 $103,651 Genia Leskiw PC Retired $148,000 $103,651 Jeff Johnson PC Defeated $148,000 $103,651 Kyle Fawcett -

Orange Chinook: Politics in the New Alberta
University of Calgary PRISM: University of Calgary's Digital Repository University of Calgary Press University of Calgary Press Open Access Books 2019-01 Orange Chinook: Politics in the New Alberta University of Calgary Press Bratt, D., Brownsey, K., Sutherland, R., & Taras, D. (2019). Orange Chinook: Politics in the New Alberta. Calgary, AB: University of Calgary Press. http://hdl.handle.net/1880/109864 book https://creativecommons.org/licenses/by-nc-nd/4.0 Attribution Non-Commercial No Derivatives 4.0 International Downloaded from PRISM: https://prism.ucalgary.ca ORANGE CHINOOK: Politics in the New Alberta Edited by Duane Bratt, Keith Brownsey, Richard Sutherland, and David Taras ISBN 978-1-77385-026-9 THIS BOOK IS AN OPEN ACCESS E-BOOK. It is an electronic version of a book that can be purchased in physical form through any bookseller or on-line retailer, or from our distributors. Please support this open access publication by requesting that your university purchase a print copy of this book, or by purchasing a copy yourself. If you have any questions, please contact us at [email protected] Cover Art: The artwork on the cover of this book is not open access and falls under traditional copyright provisions; it cannot be reproduced in any way without written permission of the artists and their agents. The cover can be displayed as a complete cover image for the purposes of publicizing this work, but the artwork cannot be extracted from the context of the cover of this specific work without breaching the artist’s copyright. COPYRIGHT NOTICE: This open-access work is published under a Creative Commons licence. -

Legislative Assembly of Alberta the 28Th Legislature Third Session
Legislative Assembly of Alberta The 28th Legislature Third Session Standing Committee on Public Accounts Monday, March 23, 2015 6:16 p.m. Transcript No. 28-3-6 Legislative Assembly of Alberta The 28th Legislature Third Session Standing Committee on Public Accounts Saskiw, Shayne, Lac La Biche-St. Paul-Two Hills (W), Chair Young, Steve, Edmonton-Riverview (PC), Deputy Chair Allen, Mike, Fort McMurray-Wood Buffalo (PC) Anderson, Rob, Airdrie (PC) Anglin, Joe, Rimbey-Rocky Mountain House-Sundre (Ind) Barnes, Drew, Cypress-Medicine Hat (W) Bilous, Deron, Edmonton-Beverly-Clareview (ND) Donovan, Ian, Little Bow (PC) Hehr, Kent, Calgary-Buffalo (AL) Horne, Fred, Edmonton-Rutherford (PC) Jansen, Sandra, Calgary-North West (PC) Jeneroux, Matt, Edmonton-South West (PC) Luan, Jason, Calgary-Hawkwood (PC) Pastoor, Bridget Brennan, Lethbridge-East (PC) Rowe, Bruce, Olds-Didsbury-Three Hills (PC)* Sarich, Janice, Edmonton-Decore (PC) * substitution for Fred Horne Also in Attendance Starke, Dr. Richard, Vermilion-Lloydminster (PC) Office of the Auditor General Participants Merwan Saher Auditor General Brad Ireland Assistant Auditor General Eric Leonty Assistant Auditor General Support Staff W.J. David McNeil Clerk Robert H. Reynolds, QC Law Clerk/Director of Interparliamentary Relations Shannon Dean Senior Parliamentary Counsel/ Director of House Services Philip Massolin Manager of Research Services Stephanie LeBlanc Legal Research Officer Sarah Amato Research Officer Nancy Robert Research Officer Corinne Dacyshyn Committee Clerk Jody Rempel Committee Clerk Karen Sawchuk Committee Clerk Christopher Tyrell Committee Clerk Rhonda Sorensen Manager of Corporate Communications and Broadcast Services Jeanette Dotimas Communications Consultant Tracey Sales Communications Consultant Janet Schwegel Managing Editor of Alberta Hansard Transcript produced by Alberta Hansard March 23, 2015 Public Accounts PA-441 6:16 p.m. -

Premier Promotes Verlyn Olson and Greg Weadick to Cabinet Cal Dallas Becomes the New Parliamentary Assistant to Finance
February 17, 2011 Premier promotes Verlyn Olson and Greg Weadick to cabinet Cal Dallas becomes the new Parliamentary Assistant to Finance Edmonton... Premier Ed Stelmach announced today that Wetaskiwin-Camrose MLA Verlyn Olson, QC, has been named Minister of Justice and Attorney General, and Lethbridge West MLA Greg Weadick has been named Minister of Advanced Education and Technology. “I’m pleased to welcome Verlyn and Greg to the cabinet table,” said Premier Stelmach. “Verlyn and Greg bring the necessary talent and experience - Greg as a parliamentary assistant and Verlyn as a long-time member of the bar - to complete our cabinet team. Our cabinet will continue to provide the steady leadership required right now to continue building a better Alberta.” Premier Stelmach also named a new Parliamentary Assistant to the Minister of Finance and Enterprise. “I’m pleased that Red Deer South MLA Cal Dallas, who had been serving as the Parliamentary Assistant in Environment, will take over this important role and work closely with Finance Minister Lloyd Snelgrove,” said the Premier. Premier Stelmach also announced changes to committee memberships. Joining the Agenda and Priorities Committee are Sustainable Resource Development Minister Mel Knight, Children and Youth Services Minister Yvonne Fritz and Agriculture and Rural Development Minister Jack Hayden. New members of Treasury Board are Len Webber, Minister of Aboriginal Relations, Heather Klimchuk, Minister of Service Alberta, and Naresh Bhardwaj, MLA for Edmonton-Ellerslie. The new Cabinet members will be sworn in Friday, February 18 at 8:30 a.m. at Government House. Lloyd Snelgrove was sworn in as Minister of Finance and Enterprise on January 31. -

Naughty and Nice to Taxpayers List’ 2013
‘Naughty and Nice to Taxpayers List’ 2013 Naughty Alison Redford: Premier Redford flies around the world more than Santa Claus and gives out more free gifts paid for by debt than the big man in red could ever hope to, using mere elves. Total expense: $82,872 Notable airfare expense claims: o $7,875 to New Brunswick o $6,092 to Chicago o $5,927 to Toronto Notable hotel expense claims: o $876/night in Washington (x2) o $772/night in New York (x3) o $635/night in Toronto (x2) o $649/night in Ottawa (x2) Notable meal & hospitality claims o $22 coffees in Washington o $31 hamburger in Washington Doug Horner: Government debt is sort of like making the kids pay Santa for mom and dad’s presents. Since Doug is leaving behind debt for the little ones, Santa is likely to leave behind a lump of coal for him this year. Large debt and deficit; Even the Auditor General can’t figure out how to make sense out of his books; Initially banning the CTF from the budget lockup. Thomas Lukaszuk: Less naughty than last year, but Minister Lukaszuk sure does love flying to Calgary any chance that the can get. No driving for him. He even managed to find an excuse to be in Calgary on ‘government business’ for five days during Stampede. The last time Santa spent five days at Stampede, the elves fell behind on Cabbage Patch Kids and Mrs. Claus made him sleep on the couch for a week. Add to this his threat to raise beer taxes, and he really had no chance of making the Nice List this year. -

Celebrate Seniors for Their Contributions Seniors’ Week 2014 June 2Nd to 8Th
ACA Celebrate Seniors for their Contributions Seniors’ Week 2014 June 2nd to 8th Alberta Council on Aging Spring 2014 Vol. 46 No. 4 Canadian Publication Mail Product Agreement No. 40028759 Return Undeliverable Canadian addresses to: Box 9 - 11808 St. Albert Trail, Edmonton AB, T5L 4G4 2 ACA News Spring 2014 Table of Contents Reports and Updates Articles President’s Report 4 Top 10 Cyber Crime Prevention Tips 5 Changing Times By Gary Pool Changing face of Recreational Programming 6 Executive Director’s Report 5 Building Alberta 8 Congratulations Seniors! Developing a 50-Year Transportation Strategy By Donna Durand By Becky Shepherd Meeting with the Honorable Dave Quest 7 Information from Johnson`s Inc. 9 Travel Insurance : Limitations and Exclusions Feedback Matters: Pharmacare Update 7 By Donna Durand Alberta Senior’s Benefits Then, and Now 10 A Brief History What Have We Been Doing? 15 Summary of the Alberta Council on Aging’s Actives Public-Private Partnerships 12 By Donna Durand Alberta Health Advocates 15 Linguistic Landmines 14 Health and Housing Committee 2014 16 By Wendy Armstrong Regional Reports 17 What is Person-Centred Care 20 Featuring the 7 Key elements of Person-Centred Care Senior Friendly™ Update 19 Congratulations Sturgeon Foundation Features Community Focus 8 Seasonal Recipe 11 Enactus Cheese and Crackers In Focus : Murray MacKay 12 Tales from the Koffee Klatch 15 The Alberta Council on Aging in Pictures 13 Member Feedback 21 Join the Provincial Launch of Seniors’ week! Older, Bolder, Better Seniors’ Fair and Exhibition -

ALBERTA FIRE CHIEFS ASSOCIATION the an Interview
GTHEazette ALBERTA FIRE CHIEFS ASSOCIATION Fall/Winter 2011 An Interview With Minister Doug Griffiths Women Can Do It! Where is Longview? Who is on the Scene First? Fall/Winter 2011 | 1 Dear Friends, the fire emergency in Slave Lake last spring. Your efforts clearly showed the impact our network of professionals It is great to send you a note with this second edition of can have. It was a job well done. The Gazette in its new format. We have received great reviews from both fire chiefs and advertisers. We also We are already planning the next AGM scheduled for are distributing the magazine to all fire departments June 10 through June 13 in Edmonton at the Mayfield in Manitoba, Saskatchewan, Alberta and British Inn and Convention Centre. Our golf tournament will Columbia—that is good news for advertisers. be held on June 9. Why don’t you surprise us and register early—it will make planning and organizing Please share your copy of The Gazette. We have found much easier. In any case, we want to see you there. If that very few fire personnel have seen the first edition. you are considering a resolution please contact Chief We especially thank the Edmonton and Calgary fire Randy Schroeder in Mayerthorpe. Resolutions must be departments for distributing copies to all their halls. submitted by April 10 so they can be posted on the We will be asking other large fire departments to do AFCA website by April 26, 2012. For more details about the same. If you are in a smaller department and want the AGM see the notice in this magazine or visit the more than one copy, please let us know.