Design of Wound Protector/Retractor for Thyroid Surgery
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
CST-On-Demand-Binder.Pdf
Zander Perioperative Education Zander CST Exam Preparation Course Zander Perioperative Education Certification Preparation for CNOR, CAPA-CPAN, CST and CBSPD Wendy Zander MSN/Ed, RN, CNOR [email protected] Test Taking Strategies Objectives: 1. Apply Test Taking Strategies for the CST exam 2. Create a Personal Study Plan 3. Eligibility • Registering for the exam • Exam Format • Time Management • Test Taking Strategies Eligibility • Current or previously Certified Surgical Technologist (CST) ▫ Evidence of CST Certification • Graduate of a surgical technology program accredited by CAAHEP ▫ Evidence of proof of graduation • Graduate of a surgical technology accredited by ABHES ▫ Evidence of proof of graduation www.periop-ed.com 1 Zander Perioperative Education Military Eligible • A graduate of a military training program in surgical technology is always eligible whether it was before, during or after having CAAHEP accreditation. ▫ a copy of your DD214 (must state location of the base where program was completed), ▫ a copy of your graduation certificate from the surgical technology training program ▫ a smart transcript Accelerated Alternate Delivery (AAD) Pathway • Have on-the-job training in surgical technology • Are a graduate from a surgical technology program that did not hold CAAHEP accreditation during your enrollment CST Testing Fees First Time Test Takers Exam Fee (AST Members) Exam Fee (Non Members) $190 $290 Current or Previous Certified Surgical Technologist Renewing First Time Test Takers Certification by Examination Exam Fee -
Minimal Endoscope-Assisted Thyroidectomy Through a Retroauricular Approach: an Evolving Solo Surgery Technique
ORIGINAL ARTICLE Minimal Endoscope-assisted Thyroidectomy Through a Retroauricular Approach: An Evolving Solo Surgery Technique Myung Jin Ban, MD,*w Jae Won Chang, MD,z Won Shik Kim, MD,y Hyung Kwon Byeon, MD, PhD,y Yoon Woo Koh, MD, PhD,y and Jae Hong Park, MD, PhD* (RA), or transoral approach.1–5 Endoscopic thyroidectomy Abstract: This study aimed to evaluate the feasibility and efficacy of through an RA approach is an especially excellent choice minimal endoscope-assisted thyroidectomy (MEAT) through a for head and neck surgeons because of their familiarity with retroauricular (RA) approach. Most of the thyroidectomy oper- the direction of the approach, the short distance to the ative time was accounted for by direct visualization through the thyroid gland, and a good cosmetic outcome without the RA window, minimizing interference between surgical instruments. 6 Endoscope use was minimized and limited to critical surgical need for additional incisions. aspects, including preservation of the recurrent laryngeal nerve and Despite the advantages of the RA approach, funda- parathyroid glands. The recurrent laryngeal nerve was neuro- mental limitations of endoscopic surgery still exist, includ- monitored throughout the procedure. MEAT through an RA ing a narrow operative field that restricts the free movement approach was performed in 8 patients with papillary thyroid car- of instruments. Gas insufflation, an additional incision for cinoma (mean tumor size, 1.2 ± 0.5 cm). The mean patient age was the endoscope port, robotic arm assistance, and a flexible 41.1 ± 7.5 years. The endoscopic operating time was endoscope holder for solo surgery have all been used to 19 ± 3.4 minutes, and no postoperative hematoma, seroma, or overcome this limitation.3,7,8 vocal cord paralysis was observed. -
Chordee Without Hypospadias Components Steps OR Set-Up 1
Chordee without Hypospadias Components Steps OR Set-up 1. Confirm meatus position, that hypospadias is not present Gauze sponge 2. Crede to confirm urinary stream is axially directed Towel 3. Evaluate for concealment. 1. Strategy Snugger 4. Artificial erection induced PRN “Grandfather forceps” 1. Robot clamp set-up Robot clamp 2. Safely position glans traction hemostat to avoid hitting the 2. Robot setup boy’s head or dislodging ET tube Robot Arm 3. Suture taut, but not tight Marking pen 1. Midline scrotal incision Scalpel 3. Complex scrotoplasy 2. Paired base incision as saw tooth Straight serrated scissors Grandfather forceps Marking pen 4. Reconstruct 1. Normalize preputial meatus 7x7-0 Vicryl (TG 140-8) [J546] - one appearance of skin 2. Rearrange foreskin to approach normal needle cut off “Father” forceps Straight serrated scissors 5-0 Ethibond (RB –1) [X 870] 1. Walk needle from dorsal meatus into lumen 5. Glans suture Straight hemostat 2. Exit needle1/3 of width of glans Needle holder Marking pen “Baby” forceps 1. Crede to assess if urinary stream shows a normal direction Scalpel 2. Expose urethral web skin as “goal posts” Wreck-cel 3. Make urethrotomy incision between the “goal posts” Saline irrigation 6. Urethrotomy 4. Rechecks stream by crede after urethrotomy is complete 7-0 Vicryl (TG 140 - 8)[J546] -one needle cut off Curved Wescott scissors Assorted catheters Straight iris scissors Straight hemostat 1. Advance urethra catheter to peno-scrotal junction “Fathers” foceps 7. Catheterize urethra 2. Check how thin the urethra is 5-0 Ethibond (RB –1) [X 870] 3. Suture ligate catheter to glans traction suture 8 French Red Rubber 5 French Feeding Tube CEVL 2009 Chordee without Hypospadias Components Steps OR Set-up 1. -

Rapid HTA Report Ultrasonic Energy Devices for Surgery July 2014
Rapid HTA report 1 Ultrasonic energy devices for surgery July 2014 1 This report should be cited as: Migliore A, Corio M, Perrini MR, Rivoiro C, Jefferson T. Ultrasonic energy devices for surgery: rapid HTA report. Agenas, Agenzia nazionale per i servizi sanitari regionali. Rome, July 2014. Contributions Authors Antonio Migliore, Mirella Corio, Maria Rosaria Perrini, Chiara Rivoiro, and Tom Jefferson Agenas, Agenzia nazionale per i servizi sanitari regionali, Area Funzionale Innovazione, Sperimentazione e Sviluppo, via Puglie 23, 00187 Rome (Italy) Corresponding author Antonio Migliore, MSc ([email protected]) Clinical experts Mario Alessiani, MD FACS Division of General Surgery, Varzi Hospital, University of Pavia (Italy) Marco Filauro, MD Division of General and Hepatobiliopancreatic Surgery, Galliera Hospital, Genova (Italy) Invited reviewers Chuong Ho, MD MSc Canadian Agency for Drugs and Technologies in Health (CADTH), Ottawa (Canada) Björn Fahlgren, MSc 2 Comité d’évaluation des technologies de santé (CEDIT), Paris (France) Acknowledgements Authors would like to thank Marina Cerbo (Agenas) and Simona Paone (Agenas), for the valuable help in reviewing the research protocol and the first draft of the report, Patrizia Brigoni (Agenas) for performing the systematic literature searches, Fabio Bernardini (Agenas) for his relevant support in retrieving the publications, and Laura Velardi (Agenas) for supporting consultation and analysis of databases. Declaration on the conflict of interest and privacy Authors, Clinical expert and External Reviewers declare that they do not receive benefits or harms from the publication of this report. None of the authors have or have held shares, consultancies or personal relationships with any of the producers of the devices assessed in this document. -

Case Report Management of Total Transection of Nasoendotracheal Tube During Lefort I Osteotomy
Hindawi Case Reports in Anesthesiology Volume 2020, Article ID 2097240, 4 pages https://doi.org/10.1155/2020/2097240 Case Report Management of Total Transection of Nasoendotracheal Tube during LeFort I Osteotomy Miles Somers ,1 Peter Tsakiris,1 Peter Isert,2 and Samuel Kim 1 1Department of Oral and Maxillofacial Surgery, Prince of Wales Hospital, Randwick, NSW, Australia 2VMO Anaesthetist, Prince of Wales Private Hospital, Randwick, NSW, Australia Correspondence should be addressed to Miles Somers; [email protected] Received 10 March 2020; Revised 8 August 2020; Accepted 26 October 2020; Published 17 November 2020 Academic Editor: Pavel Michalek Copyright © 2020 Miles Somers et al. *is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Transection of the nasoendotracheal tube during orthognathic surgery is a rare, but life-threatening complication. We present a case of complete nasoendotracheal tube transection during a LeFort 1 osteotomy and discuss appropriate preventative and management techniques. 1. Introduction 2. Case Report Complete transection of the nasoendotracheal tube (NET) A 28-year-old male underwent a 2-piece maxillary osteot- during surgery is rare [1]. However, it poses a potentially life- omy plus right ramus graft for genioplasty. *e aim of the threatening complication that must be managed effectively. surgery was orthognathic correction of a dentoskeletal class *ere are several reported cases in the literature reporting III malocclusion related to hypoplasia of the maxilla sec- both complete [2, 3] and partial transection [4–7]. Maxil- ondary to cleft lip and palate. -

What to Teach a New Technician: Part II
INSTRUMENT WHISPERER What to Teach a New Technician: Part II BY RICK SCHULTZ he Instrument Whisperer retractor is used to move tissue, muscle column in the May/June issue and organs aside in order to expose of PROCESS addressed the the surgical site. It is important for the importance of process in the technician to know the proper names and Thiring, training and retention of quality how to measure (See Figure A) to ensure Sterile Processing (SP) professionals. It the correct retractor is placed into the also specifically addressed the importance surgical set. of instrument inspection and the new technician’s need to know the basic instrument groups. That article focused on inspection of scissors, needle holders and hemostats. This article focuses on Figure B the following three instrument groups: • Retractors; • Suction devices; and • Scalpel handles Note: Once the right person has been hired, it is beneficial to have them observe four or five surgeries of various specialties, so they can see the use of the products they will be putting into trays. Figure A Retractors Retractors play a crucial role in surgery. Two common types of hand-held As with all surgical instruments, it is retractors are the Kelly retractor important to learn the most commonly- (Figure B) and the Richardson retractor used retractors, their main differences (Figure C). and how to properly inspect them. The difference between these retractors There are several broad categories of is the depth and width of the blades. A Figure C retractors: Kelly retractor is always larger than a • Hand-held retractors – A hand-held Richardson retractor. -

Instruments 449-478 4/3/06 10:42 AM Page 449
Instruments_449-478 4/3/06 10:42 AM Page 449 Neuro Hammers & Diagnostic ADC® NEUROLOGICAL HAMMERS Four of the most popular hammers for diagnosis of neurological function. 369110105375 Buck Hammer, 7 1/4˝, Chrome Plated Handle w/2 sided rubber head, Handle Conceals “screw-in” Brush, Needle Contained Within The Head 369310105374 Taylor Hammer, 7 1/2˝, Chrome Handle w/triangular rubber head, Orange 3693BK10141795 Taylor Hammer, 7 1/2˝, Chrome Handle w/triangular rubber head, Black 3693DG10141796 Taylor Hammer, 7 1/2˝, Chrome Handle w/triangular rubber head, Dark Green 3693RB10141797 Taylor Hammer, 7 1/2˝, Chrome Handle w/triangular rubber head, ADC® TUNING FORKS Royal Blue 369510105372 Wartenberg Pinwheel, 7 1/2˝, Stainless Steel Handle w/textured grip, Non magnetic, corrosion resistant aluminum alloy construction weighs 1/3 of Rotating Spur comparable steel tuning forks. Produced from 3/8˝ x 1˝ bar stock for superior 369710105373 Babinski Hammer, 8 1/2˝, Octagonal Stainless Steel Handle w/concealed performance and consistent frequency accuracy. Extra long 2˝ handle of turned needle, Rubber Head smooth aluminum to facilitate bone conduction tests. 50012810105366 Tuning Fork w/fixed weight, 128cps Frequency 50025610105367 Tuning Fork w/fixed weight, 256cps Frequency 50051210105368 Tuning Fork w/o weight, 512cps Frequency 50102410105369 Tuning Fork w/o weight, 1024cps Frequency 50204810105370 Tuning Fork w/o weight, 2048cps Frequency 50409610105371 Tuning Fork w/o weight, 4096cps Frequency 1-200 1-220 MILTEX HAMMERS 1-20010090643 Taylor Percussion -

RENAISSANCE-CATALOG-5-1.Pdf
MICRINS ® Contents Scissors 1-17 Needle Holders 18-25 Thumb Forceps 26-31 Endoscopic Products 32-42 Rhinoplasty Retractors 43 Rasps and Osteotomes 44-47 Elevators and Dissectors 48-50 Rongeurs and Morselizers 51-53 Retractors and Hooks 54-67 Speculums 68 Knives 69-70 Forceps 71-77 Measuring Instruments 78-79 Microsurgery Products 80-110 Electrosurgery 113-118 Miscellaneous 119-122 Care and Handling Instructions 123 Instrument Sets 124-132 Index 133-135 Renaissance Surgical, Inc. 800-833-3380 MICRINS® SURGICAL INSTRUMENTS Product Warranty Surgical instruments bearing the MICRINS brand name are guaranteed to be free from defects in workmanship and materials when used normally for their intended purpose. Any MICRINS instrument proving to be defective will be repaired or replaced at no charge for the repair or for replacement. Renaissance Surgical has the option to repair or replace in its sole discretion. Additionally, Renaissance Surgical provides these specific guaranties against wear: MICRINS RAZOR-EDGE™ scissors are guaranteed forever. Should the scissors ever become dull, for any reason, we will sharpen or replace the scissors at no charge for sharpening or the replacement scissors, for as long as you own the scissors. Sharpening or adjustment by any service or company other than Renaissance Surgical will void the lifetime edge guarantee. SABLE™ Tungsten-Carbide needle holders are guaranteed against wear, under normal use, for five years. We will repair or replace, at our discretion, the needle holder at no charge for the insert or the replacement instrument during the warranty period. Repair or adjustment by any service or company other than Renaissance Surgical will void the warranty. -

Basic Surgical Skills and Techniques
BASIC SURGICAL SKILLS AND TECHNIQUES BASIC SURGICAL SKILLS AND TECHNIQUES THIRD EDITION Editors Sudhir Kumar Jain MS FRCS (Edinburgh) FACS FICS MBA (HCA) Professor Department of Surgery Maulana Azad Medical College New Delhi, India David L Stoker MD FRCS (Edinburgh) Consultant Surgeon North Middlesex University Hospital London, UK Professor St George's International Medical School London, UK Raman Tanwar MS MCh (Urology) FMAS Fellowship in Andrology and Men's Health Consultant Urologist and Andrologist Urocenter, Jyoti Hospital and Paras Hospital Gurugram,Haryana, India Jaypee Brothers Medical Publishers (P) Ltd. Headquarters Jaypee Brothers Medical Publishers (P) Ltd 4838/24, Ansari Road, Daryaganj New Delhi 110 002, India Phone: +91-11-43574357 Fax: +91-11-43574314 Email: [email protected] Overseas Oces J.P. Medical Ltd 83 Victoria Street, London, SW1H 0HW (UK) Phone: +44 20 3170 8910 Fax: +44 (0)20 3008 6180 Email: [email protected] Jaypee-Highlights Medical Publishers Inc City of Knowledge, Bld. 235, 2nd Floor, Clayton Panama City, Panama Phone: +1 507-301-0496 Fax: +1 507-301-0499 Email: [email protected] Jaypee Brothers Medical Publishers (P) Ltd 17/1-B Babar Road, Block-B, Shaymali Mohammadpur, Dhaka-1207 Bangladesh Mobile: +08801912003485 Email: [email protected] Jaypee Brothers Medical Publishers (P) Ltd Bhotahity, Kathmandu Nepal Phone: +977-9741283608 Email: [email protected] Website: Www.Jaypeebrothers.Com Website: Www.Jaypeedigital.Com © 2018, Jaypee Brothers Medical Publishers The views and opinions expressed in this book are solely those of the original contributor(s)/author(s) and do not necessarily represent those of editor(s) of the book. All rights reserved. -

Thoracoscopic Spine Surgery for Decompression and Stabilization of the Anterolateral Thoracolumbar Spine
Neurosurg Focus 19 (6):E4, 2005 Thoracoscopic spine surgery for decompression and stabilization of the anterolateral thoracolumbar spine AMIN AMINI, M.D., M.SC., RUDOLF BEISSE, M.D., AND MEIC H. SCHMIDT, M.D. Department of Neurosurgery, University of Utah, Salt Lake City, Utah; and Department of Trauma Surgery, Berufsgenossenschaftliche Unfallklinik Murnau, Germany The anterior thoracolumbar spine can be exposed via a variety of approaches. Historically, open anterolateral or pos- terolateral approaches have been used to gain access to the anterior thoracolumbar spinal column. Although the expo- sure is excellent, open approaches are associated with significant pain and respiratory problems, substantial blood loss, poor cosmesis, and prolonged hospitalization. With the increasing use of the endoscope in surgical procedures and recent advances in video-assisted thoracoscopic surgery, minimally invasive thoracoscopic spine surgery has been developed to decrease the morbidity associated with open thoracotomy. The purpose of this article is to illustrate the surgical technique of a minimally invasive thoracoscopic approach to the anterolateral thoracolumbar spine and to dis- cuss its potential indications and contraindications in patients with diseases involving the anterior thoracic and lumbar regions. KEY WORDS • endoscopic spinal surgery • thoracoscopy • thoracic spine • lumbar spine • thoracoscopic spinal instrumentation Since the introduction of thoracoscopic surgery by Jaco- Minimal access surgical techniques can potentially de- baeus15 in 1910, the technique has undergone enormous crease spinal access morbidity and speed recovery and advances. With the development of high-quality video im- healing.4,7,16,17 At the University of Utah Medical Center, we aging, small endoscopes, and modified new instruments, have performed 30 thoracoscopic spine surgeries for tho- video-assisted thoracic surgery has become the minimally racolumbar trauma, tumors, and infection. -

Cardiovascular/ Thoracic Portfolio
CVT-2 CARDIOVASCULAR/THORACIC Cardiovascular/ Scan the code above to learn more about our Cardiovascular/ Thoracic portfolio. Thoracic Portfolio Questions? Contact us at [email protected] or learn more at symmetrysurgical.com CARDIOVASCULAR/THORACIC CVT-1 Cardiovascular/Thoracic CVT Approximators CVT-2 Punches CVT-136 Cannulas CVT-3 Raspatory CVT-137 Clamps CVT-3 Retractors CVT-138 Containers CVT-55 Rib Spreader CVT-186 Cords CVT-63 Rongeurs CVT-187 Cups CVT-63 Saws CVT-188 Dilators CVT-64 Scissors CVT-188 Dissectors CVT-68 Shears CVT-216 Elevators CVT-70 Spatulas CVT-218 Forceps CVT-71 Spreaders CVT-218 Hooks CVT-121 Stringers CVT-220 Knife Handles CVT-121 Strippers CVT-222 Knives CVT-122 Suction Tubes CVT-223 Loops CVT-122 Sump Suction CVT-225 Markers CVT-122 Tourniquets CVT-225 Needle Holders CVT-123 Trocars CVT-225 Needles CVT-135 Tunnelers CVT-226 Obturators CVT-135 Valvulotomes CVT-227 Pliers CVT-135 Wire & Pin Cutters CVT-227 Questions? Contact us at [email protected] or learn more at symmetrysurgical.com Questions? Contact us at [email protected] or learn more at symmetrysurgical.com The Surgical Instrument Desk Reference How to Use Our Catalog U.S. Customer Service The Symmetry Surgical catalog is designed with Your Symmetry Surgical Customer Service team wants you in mind, to be your trusted resource for surgical to make ordering surgical instruments the easiest part instrumentation. We took great care in creating an of your day. We accept orders via phone, fax, email, our easy-to-use, robust catalog and we think you'll be website, Global Healthcare Exchange (GHX) and pleased with the design as you become more familiar through the mail. -
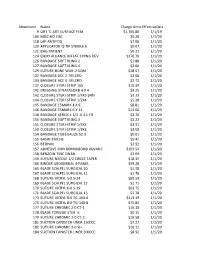
Mnemonic Name Charge Amounteffectivedate 9 ORT TJ ART
Mnemonic Name Charge AmountEffectiveDate 9 ORT TJ ART SURFACE FEM $1,765.80 1/1/19 100 MISC NO CHG $0.20 1/1/20 118 LAP ANTIFOG $7.06 1/1/20 120 APPLICATOR Q-TIP STERILE 6 $0.07 1/1/20 121 BAG PATIENT $0.21 1/1/20 124 ENDO ALLIANCE INFLAT SYRNG DEV $176.70 1/1/20 126 BANDAGE SOFT KLING 2 $1.88 1/1/20 127 BANDAGE SOFT KLING 4 $2.60 1/1/20 129 SUTURE BONE WAX 2.5QM $28.57 1/1/20 132 BANDAGE ACE 2 VELCRO $2.06 1/1/20 133 BANDAGE ACE 3 VELCRO $2.72 1/1/20 137 CLOSURE STERI-STRIP 1X5 $10.39 1/1/20 141 DRESSING STRATASORB 4 X 4 $9.25 1/1/20 142 CLOSURE STERI-STRIP 1/4X3 BRN $3.33 1/1/20 144 CLOSURE STERI-STRIP 1/2X4 $5.28 1/1/20 145 BANDAGE ESMARK 4 X 9 $8.81 1/1/20 146 BANDAGE ESMARK 6 X 12 $13.00 1/1/20 148 BANDAGE KERLIX 4 1/2 X 4.1 YD $3.70 1/1/20 150 BANDAGE SOFT KLING 3 $2.23 1/1/20 151 CLOSURE STERI-STRIP 1/4X3 $3.31 1/1/20 153 CLOSURE STERI-STRIP 1/8X3 $3.00 1/1/20 154 BANDAGE TUBEGAUZE SZ 3 $0.01 1/1/20 155 BASIN EMESIS $0.41 1/1/20 156 BEDPAN $2.92 1/1/20 157 ADHESIVE SKIN DERMABOND ADVANC $103.54 1/1/20 158 BENZOIN TINC SWAB $2.09 1/1/20 159 SUTURE NEEDLE 1/2 CIRCLE TAPER $18.35 1/1/20 160 BINDER ABDOMINAL 4-PANEL $59.28 1/1/20 165 BLADE SCALPEL SURGICAL 10 $1.78 1/1/20 167 BLADE SCALPEL SURGICAL 11 $1.78 1/1/20 168 SUTURE VICRYL 5-0 S-24 $69.59 1/1/20 169 BLADE SCALPEL SURGICAL 12 $1.71 1/1/20 170 SUTURE VICRYL 6-0 S-29 $63.75 1/1/20 171 BLADE SCALPEL SURGICAL 15 $1.78 1/1/20 173 SUTURE VICRYL 8-0 TG-160-6 $113.19 1/1/20 175 SUTURE VICRYL 8-0 TG-140-8 $75.84 1/1/20 177 SUTURE CHROMIC 2-0 CT-1 $16.10 1/1/20 178 BLADE TONGUE STER.