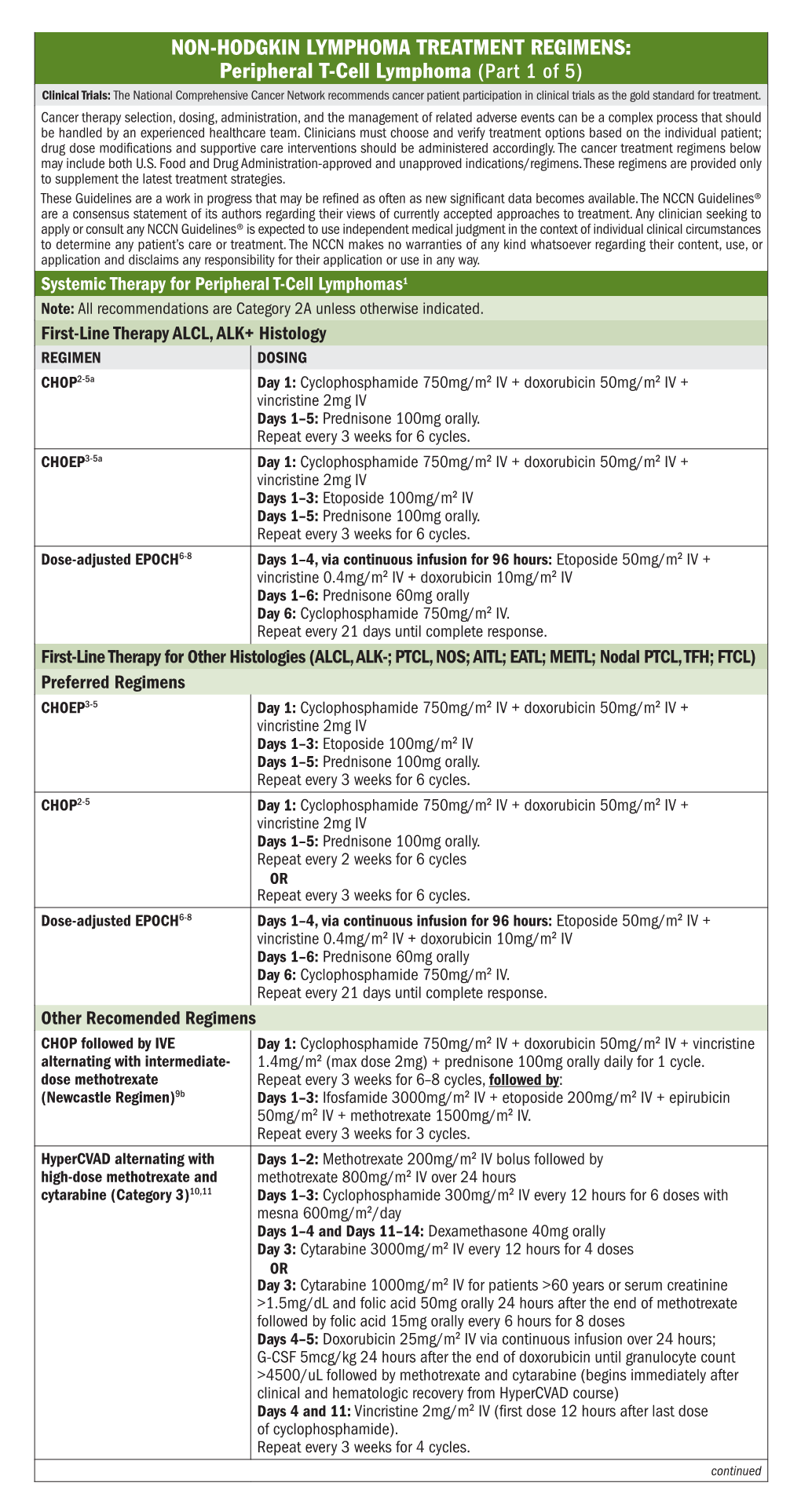
Peripheral T-Cell Lymphoma
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Alemtuzumab Comparison with Rituximab and Leukemia Whole
Mechanism of Action of Type II, Glycoengineered, Anti-CD20 Monoclonal Antibody GA101 in B-Chronic Lymphocytic Leukemia Whole Blood Assays in This information is current as Comparison with Rituximab and of September 27, 2021. Alemtuzumab Luca Bologna, Elisa Gotti, Massimiliano Manganini, Alessandro Rambaldi, Tamara Intermesoli, Martino Introna and Josée Golay Downloaded from J Immunol 2011; 186:3762-3769; Prepublished online 4 February 2011; doi: 10.4049/jimmunol.1000303 http://www.jimmunol.org/content/186/6/3762 http://www.jimmunol.org/ Supplementary http://www.jimmunol.org/content/suppl/2011/02/04/jimmunol.100030 Material 3.DC1 References This article cites 44 articles, 24 of which you can access for free at: http://www.jimmunol.org/content/186/6/3762.full#ref-list-1 by guest on September 27, 2021 Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2011 by The American -

Primary Mediastinal Large B-Cell Lymphoma
Primary Mediastinal Large B-Cell Lymphoma Page 1 of 13 Disclaimer: This algorithm has been developed for MD Anderson using a multidisciplinary approach considering circumstances particular to MD Anderson’s specific patient population, services and structure, and clinical information. This is not intended to replace the independent medical or professional judgment of physicians or other health care providers in the context of individual clinical circumstances to determine a patient's care. This algorithm should not be used to treat pregnant women. Note: Consider Clinical Trials as treatment options for eligible patients. PATHOLOGIC DIAGNOSIS INITIAL EVALUATION ESSENTIAL: 5 ● Physical exam: attention to node-bearing areas, including Waldeyer's ring, ESSENTIAL: and to size of liver and spleen ● ECOG performance status ● Hematopathology review of all slides with at least one paraffin ● B symptoms (Unexplained fever >38°C during the previous month; block or 15 unstained slides representative of the tumor. Rebiopsy if Recurrent drenching night sweats during the previous month; Weight consult material is nondiagnostic. loss >10 percent of body weight ≤ 6 months of diagnosis) ● Adequate morphology and immunophenotyping to establish 1 ● CBC with differential, LDH, BUN, creatinine, albumin, AST, diagnosis ALT, total bilirubin, alkaline phosphatase, serum calcium, uric acid ○ Paraffin Panel: CD3, CD20 and/or another pan-B-cell marker ● Beta 2 microglobulin (CD19, PAX-5, CD79a) or ● Screening for HIV 1 and 2, hepatitis B and C (HBcAb, HBsAg, HCV -

(12) Patent Application Publication (10) Pub. No.: US 2017/0209462 A1 Bilotti Et Al
US 20170209462A1 (19) United States (12) Patent Application Publication (10) Pub. No.: US 2017/0209462 A1 Bilotti et al. (43) Pub. Date: Jul. 27, 2017 (54) BTK INHIBITOR COMBINATIONS FOR Publication Classification TREATING MULTIPLE MYELOMA (51) Int. Cl. (71) Applicant: Pharmacyclics LLC, Sunnyvale, CA A 6LX 3/573 (2006.01) A69/20 (2006.01) (US) A6IR 9/00 (2006.01) (72) Inventors: Elizabeth Bilotti, Sunnyvale, CA (US); A69/48 (2006.01) Thorsten Graef, Los Altos Hills, CA A 6LX 3/59 (2006.01) (US) A63L/454 (2006.01) (52) U.S. Cl. CPC .......... A61 K3I/573 (2013.01); A61K 3 1/519 (21) Appl. No.: 15/252,385 (2013.01); A61 K3I/454 (2013.01); A61 K 9/0053 (2013.01); A61K 9/48 (2013.01); A61 K (22) Filed: Aug. 31, 2016 9/20 (2013.01) (57) ABSTRACT Disclosed herein are pharmaceutical combinations, dosing Related U.S. Application Data regimen, and methods of administering a combination of a (60) Provisional application No. 62/212.518, filed on Aug. BTK inhibitor (e.g., ibrutinib), an immunomodulatory agent, 31, 2015. and a steroid for the treatment of a hematologic malignancy. US 2017/0209462 A1 Jul. 27, 2017 BTK INHIBITOR COMBINATIONS FOR Subject in need thereof comprising administering pomalido TREATING MULTIPLE MYELOMA mide, ibrutinib, and dexamethasone, wherein pomalido mide, ibrutinib, and dexamethasone are administered con CROSS-REFERENCE TO RELATED currently, simulataneously, and/or co-administered. APPLICATION 0008. In some aspects, provided herein is a method of treating a hematologic malignancy in a subject in need 0001. This application claims the benefit of U.S. -

Alemtuzumab Comparison with Rituximab and Leukemia Whole
Mechanism of Action of Type II, Glycoengineered, Anti-CD20 Monoclonal Antibody GA101 in B-Chronic Lymphocytic Leukemia Whole Blood Assays in This information is current as Comparison with Rituximab and of September 29, 2021. Alemtuzumab Luca Bologna, Elisa Gotti, Massimiliano Manganini, Alessandro Rambaldi, Tamara Intermesoli, Martino Introna and Josée Golay Downloaded from J Immunol 2011; 186:3762-3769; Prepublished online 4 February 2011; doi: 10.4049/jimmunol.1000303 http://www.jimmunol.org/content/186/6/3762 http://www.jimmunol.org/ Supplementary http://www.jimmunol.org/content/suppl/2011/02/04/jimmunol.100030 Material 3.DC1 References This article cites 44 articles, 24 of which you can access for free at: http://www.jimmunol.org/content/186/6/3762.full#ref-list-1 by guest on September 29, 2021 Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2011 by The American -

Hodgkin Lymphoma Treatment Regimens
HODGKIN LYMPHOMA TREATMENT REGIMENS (Part 1 of 5) Clinical Trials: The National Comprehensive Cancer Network recommends cancer patient participation in clinical trials as the gold standard for treatment. Cancer therapy selection, dosing, administration, and the management of related adverse events can be a complex process that should be handled by an experienced health care team. Clinicians must choose and verify treatment options based on the individual patient; drug dose modifications and supportive care interventions should be administered accordingly. The cancer treatment regimens below may include both U.S. Food and Drug Administration-approved and unapproved indications/regimens. These regimens are provided only to supplement the latest treatment strategies. These Guidelines are a work in progress that may be refined as often as new significant data become available. The NCCN Guidelines® are a consensus statement of its authors regarding their views of currently accepted approaches to treatment. Any clinician seeking to apply or consult any NCCN Guidelines® is expected to use independent medical judgment in the context of individual clinical circumstances to determine any patient’s care or treatment. The NCCN makes no warranties of any kind whatsoever regarding their content, use, or application and disclaims any responsibility for their application or use in any way. Classical Hodgkin Lymphoma1 Note: All recommendations are Category 2A unless otherwise indicated. Primary Treatment Stage IA, IIA Favorable (No Bulky Disease, <3 Sites of Disease, ESR <50, and No E-lesions) REGIMEN DOSING Doxorubicin + Bleomycin + Days 1 and 15: Doxorubicin 25mg/m2 IV push + bleomycin 10units/m2 IV push + Vinblastine + Dacarbazine vinblastine 6mg/m2 IV over 5–10 minutes + dacarbazine 375mg/m2 IV over (ABVD) (Category 1)2-5 60 minutes. -

Clinical Policy: Pralatrexate (Folotyn)
Clinical Policy: Pralatrexate (Folotyn) Reference Number: CP.PHAR.313 Effective Date: 02.01.17 Last Review Date: 11.19 Coding Implications Line of Business: HIM*, Medicaid, HIM-Medical Benefit Revision Log See Important Reminder at the end of this policy for important regulatory and legal information. Description Pralatrexate injection (Folotyn®) is a folate analog metabolic inhibitor. ____________ *For Health Insurance Marketplace (HIM), if request is through pharmacy benefit, Folotyn (40 mg/2mL vial) is non-formulary and cannot be approved using these criteria; refer to the formulary exception policy, HIM.PA.103. FDA Approved Indication(s) Folotyn is indicated for the treatment of patients with relapsed or refractory peripheral T-cell lymphoma (PTCL). Policy/Criteria Provider must submit documentation (such as office chart notes, lab results or other clinical information) supporting that member has met all approval criteria. It is the policy of health plans affiliated with Centene Corporation® that Folotyn is medically necessary when the following criteria are met: I. Initial Approval Criteria A. Peripheral T-Cell Lymphoma (must meet all): 1. Diagnosis of PTCL; 2. Prescribed by or in consultation with an oncologist or hematologist; 3. Age ≥ 18 years; 4. Failed prior therapy (see Appendix B for examples); *Prior authorization may be required for prior therapies 5. Request meets one of the following (a or b):* a. Dose does not exceed 30 mg/m2 once weekly for 6 weeks in 7-week cycles; b. Dose is supported by practice guidelines or peer-reviewed literature for the relevant off-label use (prescriber must submit supporting evidence). *Prescribed regimen must be FDA-approved or recommended by NCCN. -

Antibody–Drug Conjugates
Published OnlineFirst April 12, 2019; DOI: 10.1158/1078-0432.CCR-19-0272 Review Clinical Cancer Research Antibody–Drug Conjugates: Future Directions in Clinical and Translational Strategies to Improve the Therapeutic Index Steven Coats1, Marna Williams1, Benjamin Kebble1, Rakesh Dixit1, Leo Tseng1, Nai-Shun Yao1, David A. Tice1, and Jean-Charles Soria1,2 Abstract Since the first approval of gemtuzumab ozogamicin nism of activity of the cytotoxic warhead. However, the (Mylotarg; Pfizer; CD33 targeted), two additional antibody– enthusiasm to develop ADCs has not been dampened; drug conjugates (ADC), brentuximab vedotin (Adcetris; Seat- approximately 80 ADCs are in clinical development in tle Genetics, Inc.; CD30 targeted) and inotuzumab ozogami- nearly 600 clinical trials, and 2 to 3 novel ADCs are likely cin (Besponsa; Pfizer; CD22 targeted), have been approved for to be approved within the next few years. While the hematologic cancers and 1 ADC, trastuzumab emtansine promise of a more targeted chemotherapy with less tox- (Kadcyla; Genentech; HER2 targeted), has been approved to icity has not yet been realized with ADCs, improvements treat breast cancer. Despite a clear clinical benefit being dem- in technology combined with a wealth of clinical data are onstrated for all 4 approved ADCs, the toxicity profiles are helping to shape the future development of ADCs. In this comparable with those of standard-of-care chemotherapeu- review, we discuss the clinical and translational strategies tics, with dose-limiting toxicities associated with the mecha- associated with improving the therapeutic index for ADCs. Introduction in antibody, linker, and warhead technologies in significant depth (2, 3, 8, 9). Antibody–drug conjugates (ADC) were initially designed to leverage the exquisite specificity of antibodies to deliver targeted potent chemotherapeutic agents with the intention of improving Overview of ADCs in Clinical Development the therapeutic index (the ratio between the toxic dose and the Four ADCs have been approved over the last 20 years (Fig. -

Horizon Scanning Status Report June 2019
Statement of Funding and Purpose This report incorporates data collected during implementation of the Patient-Centered Outcomes Research Institute (PCORI) Health Care Horizon Scanning System, operated by ECRI Institute under contract to PCORI, Washington, DC (Contract No. MSA-HORIZSCAN-ECRI-ENG- 2018.7.12). The findings and conclusions in this document are those of the authors, who are responsible for its content. No statement in this report should be construed as an official position of PCORI. An intervention that potentially meets inclusion criteria might not appear in this report simply because the horizon scanning system has not yet detected it or it does not yet meet inclusion criteria outlined in the PCORI Health Care Horizon Scanning System: Horizon Scanning Protocol and Operations Manual. Inclusion or absence of interventions in the horizon scanning reports will change over time as new information is collected; therefore, inclusion or absence should not be construed as either an endorsement or rejection of specific interventions. A representative from PCORI served as a contracting officer’s technical representative and provided input during the implementation of the horizon scanning system. PCORI does not directly participate in horizon scanning or assessing leads or topics and did not provide opinions regarding potential impact of interventions. Financial Disclosure Statement None of the individuals compiling this information have any affiliations or financial involvement that conflicts with the material presented in this report. Public Domain Notice This document is in the public domain and may be used and reprinted without special permission. Citation of the source is appreciated. All statements, findings, and conclusions in this publication are solely those of the authors and do not necessarily represent the views of the Patient-Centered Outcomes Research Institute (PCORI) or its Board of Governors. -

Structure–Function Relationships of the Variable Domains of Monoclonal
Critical Reviews in Oncology/Hematology 64 (2007) 210–225 Structure–function relationships of the variable domains of monoclonal antibodies approved for cancer treatment Charlotte Magdelaine-Beuzelin a,b, Quentin Kaas c, Vanessa Wehbi a, Marc Ohresser a, Roy Jefferis d, Marie-Paule Lefranc c, Herve´ Watier a,b,∗ a Universit´eFran¸cois Rabelais de Tours, EA 3853 “Immuno-Pharmaco-G´en´etique des Anticorps th´erapeutiques”, France b CHRU de Tours, Laboratoire d’Immunologie, France c IMGT, Laboratoire d’ImmunoG´en´etique Mol´eculaire, LIGM, Institut de G´en´etique Humaine, UPR CNRS 1142, Montpellier, France d Immunity and Infection, University of Birmingham, United Kingdom Accepted 20 April 2007 Contents 1. Chimeric and humanized antibodies .................................................................................... 211 2. IMGT Collier de Perles ............................................................................................... 217 3. Antibody/antigen interactions.......................................................................................... 219 4. Variable domain genetic analysis....................................................................................... 220 5. Immunogenicity...................................................................................................... 222 Reviewers ........................................................................................................... 223 Acknowledgements.................................................................................................. -

BC Cancer Benefit Drug List September 2021
Page 1 of 65 BC Cancer Benefit Drug List September 2021 DEFINITIONS Class I Reimbursed for active cancer or approved treatment or approved indication only. Reimbursed for approved indications only. Completion of the BC Cancer Compassionate Access Program Application (formerly Undesignated Indication Form) is necessary to Restricted Funding (R) provide the appropriate clinical information for each patient. NOTES 1. BC Cancer will reimburse, to the Communities Oncology Network hospital pharmacy, the actual acquisition cost of a Benefit Drug, up to the maximum price as determined by BC Cancer, based on the current brand and contract price. Please contact the OSCAR Hotline at 1-888-355-0355 if more information is required. 2. Not Otherwise Specified (NOS) code only applicable to Class I drugs where indicated. 3. Intrahepatic use of chemotherapy drugs is not reimbursable unless specified. 4. For queries regarding other indications not specified, please contact the BC Cancer Compassionate Access Program Office at 604.877.6000 x 6277 or [email protected] DOSAGE TUMOUR PROTOCOL DRUG APPROVED INDICATIONS CLASS NOTES FORM SITE CODES Therapy for Metastatic Castration-Sensitive Prostate Cancer using abiraterone tablet Genitourinary UGUMCSPABI* R Abiraterone and Prednisone Palliative Therapy for Metastatic Castration Resistant Prostate Cancer abiraterone tablet Genitourinary UGUPABI R Using Abiraterone and prednisone acitretin capsule Lymphoma reversal of early dysplastic and neoplastic stem changes LYNOS I first-line treatment of epidermal -
![Bendamustine and Cytosine Arabinoside: a Highly Synergistic Combination Visco C*, Carli G and Rodeghiero F Further DNA Synthesis [24]](https://docslib.b-cdn.net/cover/9877/bendamustine-and-cytosine-arabinoside-a-highly-synergistic-combination-visco-c-carli-g-and-rodeghiero-f-further-dna-synthesis-24-599877.webp)
Bendamustine and Cytosine Arabinoside: a Highly Synergistic Combination Visco C*, Carli G and Rodeghiero F Further DNA Synthesis [24]
Open Access Austin Journal of Cancer and Clinical Research Editorial Bendamustine and Cytosine Arabinoside: A Highly Synergistic Combination Visco C*, Carli G and Rodeghiero F further DNA synthesis [24]. The synergistic effect of bendamustine Department of Cell Therapy and Hematology, San Bortolo and cytarabine could be related to the individual mechanism of Hospital, Italy action of the two drugs, whose serial administration would avoid *Corresponding author: Carlo Visco, Department of the saturation of the common pathways. Cells escaping the cell cycle Cell Therapy and Hematology, San Bortolo Hospital, Via arrest induced by bendamustine and trying to repair their damage Rodolfi 37, 36100 Vicenza, Italy, Tel: +39 0444 753626; would be prone to incorporate the metabolite ara-CTP into DNA, Fax: +39 0444 920708; Email: [email protected] as reported by Staib [19] in acute myeloid leukemia cells. Indeed, the Received: January 07, 2015; Accepted: March 16, sequential treatment with bendamustine followed by cytarabine was 2015; Published: April 03, 2015 proven to be more effective than simultaneous addition of the two drugs (Figure 2) [21-23]. The S phase of the cell cycle is a crucial step Editorial of replication in mantle cell lymphoma (MCL) cells, where cyclin D1 Bendamustine is a bifunctional compound that has shown clinical overexpression deregulates the cell cycle at the G1/S phase transition, activity against various human cancers including non-Hodgkin’s and and is likely the engine continuously pushing cells towards S-phase Hodgkin’s lymphoma [1,2], chronic lymphocytic leukemia (CLL) [3], (Figure 3). Indeed, both drugs are known to be particularly active in multiple myeloma [4,5], breast cancer [6], and small-cell lung cancer patients with MCL. -

B-Cell Targets to Treat Antibody-Mediated Rejection In
Muro et al. Int J Transplant Res Med 2016, 2:023 Volume 2 | Issue 2 International Journal of Transplantation Research and Medicine Commentary: Open Access B-Cell Targets to Treat Antibody-Mediated Rejection in Transplantation Manuel Muro1*, Santiago Llorente2, Jose A Galian1, Francisco Boix1, Jorge Eguia1, Gema Gonzalez-Martinez1, Maria R Moya-Quiles1 and Alfredo Minguela1 1Immunology Service, University Clinic Hospital Virgen de la Arrixaca, Spain 2Nephrology Service, University Clinic Hospital Virgen de la Arrixaca, Spain *Corresponding author: Manuel Muro, PhD, Immunology Service, University Clinic Hospital “Virgen de la Arrixaca”, Biomedical Research Institute of Murcia (IMIB), Murcia, Spain, Tel: 34-968-369599, E-mail: [email protected] Antibody-mediated rejection (AMR) in allograft transplantation APRIL (a proliferation-inducing ligand). These co-activation signals can be defined with a rapid increase in the levels of specific are required for B-cell differentiation into plasma cell and enhancing serological parameters after organ transplantation, presence of donor their posterior survival and are a key determinant of whether specific antibodies (DSAs) against human leukocyte antigen (HLA) developing B-cells will survive or die during the establishment molecules, blood group (ABO) antigens and/or endothelial cell of immuno-tolerance [5,6]. Important used agents commercially antigens (e.g. MICA, ECA, Vimentin, or ETAR) and also particular available are Tocilizumab (anti-IL6R) and Belimumab (BAFF). histological parameters [1,2]. If the AMR persists or progresses, the The receptors of BAFF and APRIL could also be important as treatment to eliminate the humoral component of acute rejection eventual targets, for example BAFF-R, TACI (transmembrane include three sequential steps: (a) steroid pulses, antibody removal activator and calcium modulator and cyclophyllin ligand interactor) (plasma exchange or immuno-adsorption) and high doses of and BCMA (B-cell maturation antigen).