14-083 Phrma Arthritis2014 0716.Indd
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Predictive QSAR Tools to Aid in Early Process Development of Monoclonal Antibodies
Predictive QSAR tools to aid in early process development of monoclonal antibodies John Micael Andreas Karlberg Published work submitted to Newcastle University for the degree of Doctor of Philosophy in the School of Engineering November 2019 Abstract Monoclonal antibodies (mAbs) have become one of the fastest growing markets for diagnostic and therapeutic treatments over the last 30 years with a global sales revenue around $89 billion reported in 2017. A popular framework widely used in pharmaceutical industries for designing manufacturing processes for mAbs is Quality by Design (QbD) due to providing a structured and systematic approach in investigation and screening process parameters that might influence the product quality. However, due to the large number of product quality attributes (CQAs) and process parameters that exist in an mAb process platform, extensive investigation is needed to characterise their impact on the product quality which makes the process development costly and time consuming. There is thus an urgent need for methods and tools that can be used for early risk-based selection of critical product properties and process factors to reduce the number of potential factors that have to be investigated, thereby aiding in speeding up the process development and reduce costs. In this study, a framework for predictive model development based on Quantitative Structure- Activity Relationship (QSAR) modelling was developed to link structural features and properties of mAbs to Hydrophobic Interaction Chromatography (HIC) retention times and expressed mAb yield from HEK cells. Model development was based on a structured approach for incremental model refinement and evaluation that aided in increasing model performance until becoming acceptable in accordance to the OECD guidelines for QSAR models. -

Biologic Armamentarium in Psoriasis
Vol 9, Issue 1, 2016 ISSN - 0974-2441 Review Article BIOLOGIC ARMAMENTARIUM IN PSORIASIS GANESH PAI1*, NITHIN SASHIDHARAN2 1Medical Director, Derma-Care ‘The Trade Centre’, Mangalore - 575 003, Karnataka, India. 2Consultant Clinical Pharmacologist, Derma-Care ‘The Trade Centre’, Mangalore - 575 003, Karnataka, India. Email: [email protected] Received: 14 July 2015, Revised and Accepted: 24 August 2015 ABSTRACT Psoriasis is an autoimmune disease and further classed as a chronic inflammatory skin condition serving as a global burden. A moderate to severe psoriasis can be treated with conventional therapies. Less efficacy, poor patient compliance, and toxicity issues were the major problems associated with conventional therapies. The introduction of biologic therapy has a great impression on psoriatic treatment duration and enhanced quality of life in psoriasis patients. The new biologic therapies are tailor-made medications with the goal of more specific and effective treatment; less toxicity. The biologic therapy is aimed to target antigen presentation and co-stimulation, T-cell activation, and leukocyte adhesion; and pro-inflammatory cascade. They act as effective and safer substitute to traditional therapy. Secukinumab, certolizumab, itolizumab, golimumab, ustekinumab, adalimumab, infliximab etanercept, alefacept, etc. are the approved biologic with the global market. This review briefs about psoriasis pathogenesis, traditional treatments, and biologic therapies potential. Keywords: Psoriasis, Biologic, Non-biologic treatment. INTRODUCTION migration, potentiation of Th1 type of response, angiogenesis, and epidermal hyperplasia [7]. Psoriasis is an autoimmune disease and further classed as a chronic inflammatory skin condition with prevalence ranging 1-3% in the TNF- is plays vital role in the pathogenesis of psoriasis. It acts by world [1]. -
Report, Please Call the Telephone Number Listed
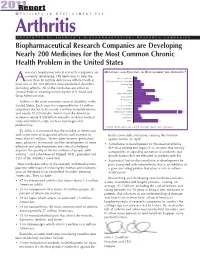
201R1e port M E D I C I N E S I N D E V E L O P M E N T F O R Arthritis P R E S E N T E D B Y A M E R I C A ’ S B I O P H A R M A C E U T I C A L R E S E A R C H C O M P A N I E S Biopharmaceutical Research Companies are Developing Nearly 200 Medicines for the Most Common Chronic Health Problem in the United States merica’s biopharmaceutical research companies are MEDICINES AND VACCINES IN DEVELOPMENT FOR ARTHRITIS* currently developing 198 medicines to help the Behcet’s Syndrome 3 more than 50 million Americans afflicted with at A Duchenne Muscular Dystrophy 6 least one of the 100 different musculoskeletal disorders, Fibromyalgia 9 including arthritis. All of the medicines are either in Gout 7 clinical trials or awaiting review by the U.S. Food and Lupus 19 Muscle Disorders 11 Drug Administration. Osteoarthritis 19 Osteoporosis 23 Arthritis is the most common cause of disability in the Pain 15 United States. Each year, it is responsible for 44 million Psoriatic Arthritis 7 outpatient doctor visits, nearly 1 million hospitalizations, Raynaud’s Disease 4 and nearly 10,000 deaths. And it costs the American Rheumatoid Arthritis 67 Scleroderma 6 economy nearly $128 billion annually in direct medical Spondylitis 7 costs and indirect costs, such as lost wages and Other 22 productivity. * Some medicines are listed in more than one category. -

Secukinumab Efficacy in Anti-TNF-Naive and Anti-TNF
Downloaded from http://ard.bmj.com/ on October 7, 2016 - Published by group.bmj.com ARD Online First, published on August 31, 2016 as 10.1136/annrheumdis-2016-210023 Clinical and epidemiological research CONCISE REPORT Secukinumab efficacy in anti-TNF-naive and anti-TNF-experienced subjects with active ankylosing spondylitis: results from the MEASURE 2 Study Joachim Sieper,1 Atul Deodhar,2 Helena Marzo-Ortega,3 Jacob A Aelion,4 Ricardo Blanco,5 Tseng Jui-Cheng,6 Mats Andersson,7 Brian Porter,8 Hanno B Richards,7 on behalf of the MEASURE 2 Study Group Handling editor Tore K Kvien ABSTRACT intolerant to these agents or fail to achieve 56 ▸ Additional material is Background There is significant unmet need in adequate disease control. published online only. To view patients with ankylosing spondylitis (AS) who have Treatment with secukinumab (human anti- please visit the journal online inadequate response or intolerance to anti-tumour interleukin (IL)-17A IgG1k monoclonal antibody) (http://dx.doi.org/10.1136/ fi annrheumdis-2016-210023). necrosis factor (TNF) treatment. Secukinumab, an anti- signi cantly improved the signs and symptoms of AS interleukin-17A monoclonal antibody, significantly when compared with placebo treatment in two phase fi For numbered af liations see improved signs and symptoms of AS in the MEASURE 2 3 trials (MEASURE 1 (intravenous followed by sub- end of article. study (NCT01649375). cutaneous (s.c.) administration; NCT01358175) and 7 Correspondence to Methods Subjects with active AS (N=219) received MEASURE 2 (s.c. administration; NCT01649375)). Professor Joachim Sieper, secukinumab (150 or 75 mg) or placebo at baseline, In MEASURE 2, 61% and 41% of subjects treated Medical Department weeks 1, 2, 3 and 4, and every 4 weeks thereafter. -

Immunfarmakológia Immunfarmakológia
Gergely: Immunfarmakológia Immunfarmakológia Prof Gergely Péter Az immunpatológiai betegségek döntő többsége gyulladásos, és ennek következtében általában szövetpusztulással járó betegség, melyben – jelenleg – a terápia alapvetően a gyulladás csökkentésére és/vagy megszűntetésére irányul. Vannak kizárólag gyulladásgátló gyógyszereink és vannak olyanok, amelyek az immunreakció(k) bénításával (=immunszuppresszió révén) vagy emellett vezetnek a gyulladás mérsékléséhez. Mind szerkezetileg, mind hatástanilag igen sokféle csoportba oszthatók, az alábbi felosztás elsősorban didaktikus célokat szolgál. 1. Nem-szteroid gyulladásgátlók (‘nonsteroidal antiinflammatory drugs’ NSAID) 2. Kortikoszteroidok 3. Allergia-elleni szerek (antiallergikumok) 4. Sejtoszlás-gátlók (citosztatikumok) 5. Nem citosztatikus hatású immunszuppresszív szerek 6. Egyéb gyulladásgátlók és immunmoduláns szerek 7. Biológiai terápia 1. Nem-szteroid gyulladásgátlók (NSAID) Ezeket a vegyületeket, melyek őse a szalicilsav (jelenleg, mint acetilszalicilsav ‘aszpirin’ használatos), igen kiterjedten alkalmazzák a reumatológiában, az onkológiában és az orvostudomány szinte minden ágában, ahol fájdalom- és lázcsillapításra van szükség. Egyes felmérések szerint a betegek egy ötöde szed valamilyen NSAID készítményt. Szerkezetük alapján a készítményeket több csoportba sorolhatjuk: szalicilátok (pl. acetilszalicilsav) pyrazolidinek (pl. fenilbutazon) ecetsav származékok (pl. indometacin) fenoxiecetsav származékok (pl. diclofenac, aceclofenac)) oxicamok (pl. piroxicam, meloxicam) propionsav -

WO 2016/176089 Al 3 November 2016 (03.11.2016) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2016/176089 Al 3 November 2016 (03.11.2016) P O P C T (51) International Patent Classification: BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, A01N 43/00 (2006.01) A61K 31/33 (2006.01) DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, HN, HR, HU, ID, IL, IN, IR, IS, JP, KE, KG, KN, KP, KR, (21) International Application Number: KZ, LA, LC, LK, LR, LS, LU, LY, MA, MD, ME, MG, PCT/US2016/028383 MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, OM, (22) International Filing Date: PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SA, SC, 20 April 2016 (20.04.2016) SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, ZW. (25) Filing Language: English (84) Designated States (unless otherwise indicated, for every (26) Publication Language: English kind of regional protection available): ARIPO (BW, GH, (30) Priority Data: GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, ST, SZ, 62/154,426 29 April 2015 (29.04.2015) US TZ, UG, ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, RU, TJ, TM), European (AL, AT, BE, BG, CH, CY, CZ, DE, (71) Applicant: KARDIATONOS, INC. [US/US]; 4909 DK, EE, ES, FI, FR, GB, GR, HR, HU, IE, IS, IT, LT, LU, Lapeer Road, Metamora, Michigan 48455 (US). -

Novel Psoriasis Therapies and Patient Outcomes, Part 2: Biologic Treatments
Novel Psoriasis Therapies and Patient Outcomes, Part 2: Biologic Treatments Meghan A. Feely, MD; Barry L. Smith, MD; Jeffrey M. Weinberg, MD Practice Points Novel biologic treatments promise exciting new therapeutic avenues for psoriasis and psoriatic arthritis (PsA). Although biologics currently in use for treatment of psoriasis and PsA are in the form of tumor necrosis factor α inhibitors, other drugs in phase 2 through phase 4 clinical trials aim to target alternative pathways underlying the pathogenesis of these disorders, including IL-12/IL-23 inhibition, IL-17 inhibition, inhibition of T-cell activation in antigen-presenting cells, regulatory T-cell activation, toll-like receptor inhibition, and granulocyte-macrophage colony-stimulating factor inhibition. New approaches to the management of psoriasis and PsA offer patientscopy hope for more targeted treat- ment regimens. not Biologic treatments have revolutionized the man- second in a 3-part series on treatments presently agement of psoriasis and psoriatic arthritis (PsA).Do in the pipeline for the management of psoriasis Anti–tumor necrosis factor (TNF) α monoclo- and PsA including topical agents, biologic treat- nal antibodies presently are approved by the ments, and systemic therapies in phase 2 through US Food and Drug Administration (FDA) for treat- phase 4 clinical trials as well as agents that are ment of these conditions. In this article, new recently FDA approved. Pivotal clinical trials, therapies that target this pathway and other steps mechanisms of action, patient outcomes, and in the pathogenesis of psoriasis and PsA are dis- pertinent safety information will be discussed for cussed, including IL-12/IL-23, IL-17, T-cell activa- each new therapy. -

Mesoblast to Evaluate Remestemcel-L in COVID-19 Lung
MESOBLAST TO EVALUATE ANTI-INFLAMMATORY CELL THERAPY REMESTEMCEL-L FOR TREATMENT OF COVID-19 LUNG DISEASE Melbourne, Australia; March 10, 2020; and New York, USA; March 9, 2020: Mesoblast Limited (Nasdaq: MESO; ASX:MSB) today announced that it plans to evaluate its allogeneic mesenchymal stem cell (MSC) product candidate remestemcel-L in patients with acute respiratory distress syndrome (ARDS) caused by coronavirus (COVID-19) in the United States, Australia, China and Europe. The Company is in active discussions with various government and regulatory authorities, medical institutions and pharmaceutical companies to implement these activities. Mortality in COVID-19 infected patients with the inflammatory lung condition acute respiratory distress syndrome (ARDS) is reported to approach 50%, and is associated with older age, co-morbidities such as diabetes, higher disease severity, and elevated markers of inflammation.1 Current therapeutic interventions do not appear to be improving in-hospital survival.1 Remestemcel-L has potential for use in the treatment of ARDS, which is the principal cause of death in COVID-19 infection.1 This is supported by recently published results from an investigator-initiated clinical study conducted in China which reported that allogeneic MSCs cured or significantly improved functional outcomes in all seven treated patients with severe COVID-19 pneumonia.2 Additionally, in post-hoc analyses of a 60-patient randomized controlled study in chronic obstructive pulmonary disease (COPD), remestemcel-L infusions were well tolerated, significantly reduced inflammatory biomarkers, and significantly improved pulmonary function in those patients with elevated inflammatory biomarkers. Since the same inflammatory biomarkers are also elevated in COVID-19, these data suggest that remestemcel-L could be useful in the treatment of patients with ARDS due to COVID-19. -

INN Working Document 05.179 Update 2011
INN Working Document 05.179 Update 2011 International Nonproprietary Names (INN) for biological and biotechnological substances (a review) INN Working Document 05.179 Distr.: GENERAL ENGLISH ONLY 2011 International Nonproprietary Names (INN) for biological and biotechnological substances (a review) Programme on International Nonproprietary Names (INN) Quality Assurance and Safety: Medicines Essential Medicines and Pharmaceutical Policies (EMP) International Nonproprietary Names (INN) for biological and biotechnological substances (a review) © World Health Organization 2011 All rights reserved. Publications of the World Health Organization are available on the WHO web site (www.who.int) or can be purchased from WHO Press, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 791 3264; fax: +41 22 791 4857; email: [email protected]). Requests for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – should be addressed to WHO Press through the WHO web site (http://www.who.int/about/licensing/copyright_form/en/index.html). The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. -

Stembook 2018.Pdf
The use of stems in the selection of International Nonproprietary Names (INN) for pharmaceutical substances FORMER DOCUMENT NUMBER: WHO/PHARM S/NOM 15 WHO/EMP/RHT/TSN/2018.1 © World Health Organization 2018 Some rights reserved. This work is available under the Creative Commons Attribution-NonCommercial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo). Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”. Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization. Suggested citation. The use of stems in the selection of International Nonproprietary Names (INN) for pharmaceutical substances. Geneva: World Health Organization; 2018 (WHO/EMP/RHT/TSN/2018.1). Licence: CC BY-NC-SA 3.0 IGO. Cataloguing-in-Publication (CIP) data. -

A Abacavir Abacavirum Abakaviiri Abagovomab Abagovomabum
A abacavir abacavirum abakaviiri abagovomab abagovomabum abagovomabi abamectin abamectinum abamektiini abametapir abametapirum abametapiiri abanoquil abanoquilum abanokiili abaperidone abaperidonum abaperidoni abarelix abarelixum abareliksi abatacept abataceptum abatasepti abciximab abciximabum absiksimabi abecarnil abecarnilum abekarniili abediterol abediterolum abediteroli abetimus abetimusum abetimuusi abexinostat abexinostatum abeksinostaatti abicipar pegol abiciparum pegolum abisipaaripegoli abiraterone abirateronum abirateroni abitesartan abitesartanum abitesartaani ablukast ablukastum ablukasti abrilumab abrilumabum abrilumabi abrineurin abrineurinum abrineuriini abunidazol abunidazolum abunidatsoli acadesine acadesinum akadesiini acamprosate acamprosatum akamprosaatti acarbose acarbosum akarboosi acebrochol acebrocholum asebrokoli aceburic acid acidum aceburicum asebuurihappo acebutolol acebutololum asebutololi acecainide acecainidum asekainidi acecarbromal acecarbromalum asekarbromaali aceclidine aceclidinum aseklidiini aceclofenac aceclofenacum aseklofenaakki acedapsone acedapsonum asedapsoni acediasulfone sodium acediasulfonum natricum asediasulfoninatrium acefluranol acefluranolum asefluranoli acefurtiamine acefurtiaminum asefurtiamiini acefylline clofibrol acefyllinum clofibrolum asefylliiniklofibroli acefylline piperazine acefyllinum piperazinum asefylliinipiperatsiini aceglatone aceglatonum aseglatoni aceglutamide aceglutamidum aseglutamidi acemannan acemannanum asemannaani acemetacin acemetacinum asemetasiini aceneuramic -
For Personal Use Only Use Personal for Function, Was Assessed at Baseline and Weeks 4 and 12
MESOBLAST STRENGTHENS KEY UNITED STATES PATENT PORTFOLIO FOR THE TREATMENT OF RHEUMATIC DISEASES New York, USA, and Melbourne, Australia; August 17, 2016: Mesoblast Limited (ASX:MSB; Nasdaq:MESO) today announced that its intellectual property portfolio covering the use of its Mesenchymal Precursor Cells (MPCs) in the treatment of rheumatic diseases, including rheumatoid arthritis (RA), has been strengthened by the granting of a key patent by the United States Patent and Trademark Office (USPTO). The Company’s patent estate in the US for the treatment of RA and related conditions comprises the newly and recently granted patents, US 9,381,216 and US 9,265,796, which cover treatment of rheumatic diseases by administration of STRO-1 positive MPCs. Together with patents covering MPC compositions-of-matter, US 7,122,178 and US 8,367,405, these granted patents provide Mesoblast with commercial rights in the US through to July 4, 2032 for the use of MPCs in the treatment of various rheumatic diseases, including rheumatoid arthritis, psoriatic arthritis, osteoarthritis, ankylosing spondylitis, sacroiliitis, and arthritis associated with inflammatory bowel disease (enteric arthritis and Reiter's syndrome). Additionally, the granted claims cover the use of these cell populations to reduce levels of inflammatory cytokines TNF-alpha, interleukin-6, and interleukin-17, all established mediators of inflammatory arthritis in rheumatic diseases. Further patent term extension may occur along with regulatory exclusivity extensions. About Mesoblast’s Phase 2 Trial In Rheumatoid Arthritis Biologic refractory RA patients who have received prior anti-TNF or other biologic agents continue to have active inflammatory pathways, and the broad, concomitant targeting of multiple cytokine networks by MPCs may result in clinically meaningful outcomes in this patient group.