Computationally Predicting Clinical Drug Combination Efficacy With
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Combination of Cabazitaxel and Plicamycin Induces Cell Death in Drug Resistant B-Cell Acute Lymphoblastic Leukemia
Clinical and Translational Science Institute Centers 9-1-2018 Combination of cabazitaxel and plicamycin induces cell death in drug resistant B-cell acute lymphoblastic leukemia Rajesh R. Nair West Virginia University Debbie Piktel West Virginia University Werner J. Geldenhuys West Virginia University Laura F. Gibson West Virginia University Follow this and additional works at: https://researchrepository.wvu.edu/ctsi Part of the Medicine and Health Sciences Commons Digital Commons Citation Nair, Rajesh R.; Piktel, Debbie; Geldenhuys, Werner J.; and Gibson, Laura F., "Combination of cabazitaxel and plicamycin induces cell death in drug resistant B-cell acute lymphoblastic leukemia" (2018). Clinical and Translational Science Institute. 34. https://researchrepository.wvu.edu/ctsi/34 This Article is brought to you for free and open access by the Centers at The Research Repository @ WVU. It has been accepted for inclusion in Clinical and Translational Science Institute by an authorized administrator of The Research Repository @ WVU. For more information, please contact [email protected]. HHS Public Access Author manuscript Author ManuscriptAuthor Manuscript Author Leuk Res Manuscript Author . Author manuscript; Manuscript Author available in PMC 2019 September 01. Published in final edited form as: Leuk Res. 2018 September ; 72: 59–66. doi:10.1016/j.leukres.2018.08.002. Combination of cabazitaxel and plicamycin induces cell death in drug resistant B-cell acute lymphoblastic leukemia Rajesh R. Naira, Debbie Piktelb, Werner J. Geldenhuysc, -
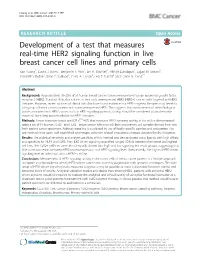
Development of a Test That Measures Real-Time HER2 Signaling Function in Live Breast Cancer Cell Lines and Primary Cells Yao Huang1, David J
Huang et al. BMC Cancer (2017) 17:199 DOI 10.1186/s12885-017-3181-0 RESEARCH ARTICLE Open Access Development of a test that measures real-time HER2 signaling function in live breast cancer cell lines and primary cells Yao Huang1, David J. Burns1, Benjamin E. Rich1, Ian A. MacNeil1, Abhijit Dandapat1, Sajjad M. Soltani1, Samantha Myhre1, Brian F. Sullivan1, Carol A. Lange2, Leo T. Furcht3 and Lance G. Laing1* Abstract Background: Approximately 18–20% of all human breast cancers have overexpressed human epidermal growth factor receptor 2 (HER2). Standard clinical practice is to treat only overexpressed HER2 (HER2+) cancers with targeted anti-HER2 therapies. However, recent analyses of clinical trial data have found evidence that HER2-targeted therapies may benefit a sub-group of breast cancer patients with non-overexpressed HER2. This suggests that measurement of other biological factors associated with HER2 cancer, such as HER2 signaling pathway activity, should be considered as an alternative means of identifying patients eligible for HER2 therapies. Methods: A new biosensor-based test (CELxTM HSF) that measures HER2 signaling activity in live cells is demonstrated using a set of 19 human HER2+ and HER2– breast cancer reference cell lines and primary cell samples derived from two fresh patient tumor specimens. Pathway signaling is elucidated by use of highly specific agonists and antagonists. The test method relies upon well-established phenotypic, adhesion-related, impedance changes detected by the biosensor. Results: The analytical sensitivity and analyte specificity of this method was demonstrated using ligands with high affinity and specificity for HER1 and HER3. The HER2-driven signaling quantified ranged 50-fold between the lowest and highest cell lines. -
Thesis Was Carried out at the K
Experimental modeling and novel therapeutic strategies in melanoma brain metastasis Terje Sundstrøm Dissertation for the degree of philosophiae doctor (PhD) University of Bergen, Norway 2015 Dissertation date: June 9th 2015 LIST OF ABBREVIATIONS 3D 3-dimensional 5-ALA 5-aminolevulinic acid AAAS American Association for the Advancement of Science ACT Adoptive cell transfer ADC Apparent diffusion coefficient AJCC American Joint Committee on Cancer AKT Protein kinase B ALK Anaplastic lymphoma kinase APC Antigen-presenting cell APOE Apolipoprotein-E ATP Adenosine triphosphate B7-H3 B7 homolog 3 BBB Blood-brain barrier BCL2A1 Bcl-2-related protein A1 bFGF Basic fibroblast growth factor BLI Bioluminescence imaging BRAF Serine/threonine-protein kinase B-raf BRMS1 Breast cancer metastasis-suppressor 1 BTB Blood-tumor barrier CI (Mitochondrial) Complex I CC22 Chemokine (C-C motif) ligand 22 CD44v6 CD44 splicing variant 6 CDK4 Cyclin-dependent kinase 4 CDKN2A p16INK4A inhibitor of CDK4 cMAP Connectivity Map CNS Central nervous system COT Serine/threonine kinase Cot CRAF RAF proto-oncogene serine/threonine-protein kinase CT Computed tomography CTLA4 Cytotoxic T-lymphocyte-associated protein 4 CXCR4 C-X-C chemokine receptor type 4 2 Da Dalton (unit) DNA Deoxyribonucleic acid DWI Diffusion weighted imaging ECM Extracranial metastases EDNRB Endothelin receptor B EFSA European Foods Safety Authority EGFR Epidermal growth factor receptor ER Estrogen receptor ERBB2 Receptor tyrosine-protein kinase erbB-2 ERK Extracellular signal-regulated kinase ET3 Endothelin-3 -

Vandetanib-Eluting Beads for the Treatment of Liver Tumours
VANDETANIB-ELUTING BEADS FOR THE TREATMENT OF LIVER TUMOURS ALICE HAGAN A thesis submitted in partial fulfilment of the requirements for the University of Brighton for the degree of Doctor of Philosophy June 2018 ABSTRACT Drug-eluting bead trans-arterial chemo-embolisation (DEB-TACE) is a minimally invasive interventional treatment for intermediate stage hepatocellular carcinoma (HCC). Drug loaded microspheres, such as DC Bead™ (Biocompatibles UK Ltd) are selectively delivered via catheterisation of the hepatic artery into tumour vasculature. The purpose of DEB-TACE is to physically embolise tumour-feeding vessels, starving the tumour of oxygen and nutrients, whilst releasing drug in a controlled manner. Due to the reduced systemic drug exposure, toxicity is greatly reduced. Embolisation-induced ischaemia is intended to cause tumour necrosis, however surviving hypoxic cells are known to activate hypoxia inducible factor (HIF-1) which leads to the upregulation of several pro-survival and pro-angiogenic pathways. This can lead to tumour revascularisation, recurrence and poor treatment outcomes, providing a rationale for combining anti-angiogenic agents with TACE treatment. Local delivery of these agents via DEBs could provide sustained targeted therapy in combination with embolisation, reducing systemic exposure and therefore toxicity associated with these drugs. This thesis describes for the first time the loading of the DEB DC Bead and the radiopaque DC Bead LUMI™ with the tyrosine kinase inhibitor vandetanib. Vandetanib selectively inhibits vascular endothelial growth factor receptor 2 (VEGFR2) and epidermal growth factor receptor (EGFR), two signalling receptors involved in angiogenesis and HCC pathogenesis. Physicochemical properties of vandetanib loaded beads such as maximum loading capacity, effect on size, radiopacity and drug distribution were evaluated using various analytical techniques. -

VIP - Ifosfamide, Cisplatin and Etoposide
THE CLATTERBRIDGE CANCER CENTRE NHS FOUNDATION TRUST Systemic Anti Cancer Treatment Protocol VIP - Ifosfamide, Cisplatin and Etoposide PROTOCOL REF: MPHA VIPGC (Version No: 1.1) Approved for use in: Germ cell Dosage: Drug Dosage Route Frequency Etoposide 75mg/m2 days 1 to 5 IV Every 21 days Cisplatin 20mg/m2 days 1 to 5 IV Every 21 days Mesna 200mg/m2 days 1 to 5 IV Every 21 days Ifosfamide 1500mg/m2 + 1500mg/m2 IV Every 21 days +Mesna days 1 to 5 Mesna 1200mg 1 to 5 Oral Every 21 days Supportive treatments: Domperidone 10mg oral tablets, up to 3 times a day or as required Dexamethasone tablets, 4mg twice daily for 3 days Filgrastim 30MU or 48MU subcutaneous injection daily for 7 days starting on day 6, repeat FBC and continue for further 7 days if neutrophil count has not recovered to 1.0 x 109/L Extravasation risk: Etoposide – Irritant Cisplatin – Exfoliant Ifosfamide - Neutral Issue Date: 31st January 2019 Review Date: January 2022 Page 1 of 10 Protocol reference: MPHAVIPGC Author: Nick Armitage Authorised by: Dr. Ali Version No:1.1 THE CLATTERBRIDGE CANCER CENTRE NHS FOUNDATION TRUST Administration: Day Drug Dosage Route Diluent and Rate 1 Dexamethasone 8mg PO 30 mins before chemotherapy 1 Ondansetron 16mg PO 30 mins before chemotherapy 1 Etoposide 75mg/m2 IV In 250 to 1000mL sodium chloride 0.9% over 60 minutes 1 Cisplatin 20mg/m2 IV 1000mL 0.9% sodium chloride over 90 minutes 1 Mesna 200mg/m2 IV In 500mL sodium chloride 0.9% over 15 minutes 1 Ifosfamide + Mesna 1500mg/m2 IV In 1000mL sodium chloride + 0.9% over 4 hours 1500mg/m2 -

Systematic Drug Screening Identifies Tractable Targeted Combination Therapies in Triple-Negative Breast Cancer
Author Manuscript Published OnlineFirst on November 21, 2016; DOI: 10.1158/0008-5472.CAN-16-1901 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. Systematic drug screening identifies tractable targeted combination therapies in triple-negative breast cancer Vikram B Wali1,3, Casey G Langdon2, Matthew A Held2, James T Platt1, Gauri A Patwardhan1, Anton Safonov1, Bilge Aktas1, Lajos Pusztai1,3, David F Stern2,3,Christos Hatzis1,3 1 Department of Internal Medicine, Section of Medical Oncology, Yale School of Medicine, Yale University, New Haven, Connecticut, USA 2 Department of Pathology, Yale School of Medicine, Yale University, New Haven, Connecticut, USA 3 Yale Cancer Center, New Haven Connecticut, USA Corresponding authors: Christos Hatzis, Ph.D. or Vikram B Wali, Ph.D. Section of Medical Oncology Yale School of Medicine Yale University 333 Cedar Street PO Box 208032 New Haven, CT 06520 [email protected] [email protected] Running Title: Novel Combination Therapies in Triple Negative Breast Cancer CONFLICTS OF INTEREST Authors have no conflict of interest to disclose. 1 Downloaded from cancerres.aacrjournals.org on October 6, 2021. © 2016 American Association for Cancer Research. Author Manuscript Published OnlineFirst on November 21, 2016; DOI: 10.1158/0008-5472.CAN-16-1901 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. ABSTRACT Triple-negative breast cancer (TNBC) remains an aggressive disease without effective targeted therapies. In this study, we addressed this challenge by testing 128 FDA-approved or investigational drugs as either single agents or in 768 pairwise drug combinations in TNBC cell lines to identify synergistic combinations tractable to clinical translation. -

(12) United States Patent (10) Patent No.: US 9,375.433 B2 Dilly Et Al
US009375433B2 (12) United States Patent (10) Patent No.: US 9,375.433 B2 Dilly et al. (45) Date of Patent: *Jun. 28, 2016 (54) MODULATORS OF ANDROGENSYNTHESIS (52) U.S. Cl. CPC ............. A6 IK3I/519 (2013.01); A61 K3I/201 (71) Applicant: Tangent Reprofiling Limited, London (2013.01); A61 K3I/202 (2013.01); A61 K (GB) 31/454 (2013.01); A61K 45/06 (2013.01) (72) Inventors: Suzanne Dilly, Oxfordshire (GB); (58) Field of Classification Search Gregory Stoloff, London (GB); Paul USPC .................................. 514/258,378,379, 560 Taylor, London (GB) See application file for complete search history. (73) Assignee: Tangent Reprofiling Limited, London (56) References Cited (GB) U.S. PATENT DOCUMENTS (*) Notice: Subject to any disclaimer, the term of this 5,364,866 A * 1 1/1994 Strupczewski.......... CO7C 45/45 patent is extended or adjusted under 35 514,254.04 U.S.C. 154(b) by 0 days. 5,494.908 A * 2/1996 O’Malley ............. CO7D 261/20 514,228.2 This patent is Subject to a terminal dis 5,776,963 A * 7/1998 Strupczewski.......... CO7C 45/45 claimer. 514,217 6,977.271 B1* 12/2005 Ip ........................... A61K 31, 20 (21) Appl. No.: 14/708,052 514,560 OTHER PUBLICATIONS (22) Filed: May 8, 2015 Calabresi and Chabner (Goodman & Gilman's The Pharmacological (65) Prior Publication Data Basis of Therapeutics, 10th ed., 2001).* US 2015/O238491 A1 Aug. 27, 2015 (Cecil's Textbook of Medicine pp. 1060-1074 published 2000).* Stedman's Medical Dictionary (21st Edition, Published 2000).* Okamoto et al (Journal of Pain and Symptom Management vol. -

The Temperature-Dependent Effectiveness of Platinum-Based
cells Article The Temperature-Dependent Effectiveness of Platinum-Based Drugs Mitomycin-C and 5-FU during Hyperthermic Intraperitoneal Chemotherapy (HIPEC) in Colorectal Cancer Cell Lines Roxan F.C.P.A. Helderman 1,2 , Daan R. Löke 2, Jan Verhoeff 3 , Hans M. Rodermond 1, Gregor G.W. van Bochove 1, Menno Boon 1, Sanne van Kesteren 1, Juan J. Garcia Vallejo 3, H. Petra Kok 2, Pieter J. Tanis 4 , Nicolaas A.P. Franken 1,2 , Johannes Crezee 2 and Arlene L. Oei 1,2,* 1 Laboratory for Experimental Oncology and Radiobiology (LEXOR), Center for Experimental and Molecular Medicine (CEMM), Amsterdam University Medical Centers (UMC), University of Amsterdam, Cancer Center Amsterdam, P.O. Box 22700, 1100 DE Amsterdam, The Netherlands; [email protected] (R.F.C.P.A.H.); [email protected] (H.M.R.); [email protected] (G.G.W.v.B.); [email protected] (M.B.); [email protected] (S.v.K.); [email protected] (N.A.P.F.) 2 Department of Radiation Oncology, Amsterdam UMC, University of Amsterdam, P.O. Box 22700, 1100 DE Amsterdam, The Netherlands; [email protected] (D.R.L.); [email protected] (H.P.K.); [email protected] (J.C.) 3 Department of Molecular Cell Biology & Immunology, Amsterdam Infection & Immunity Institute and Cancer Center Amsterdam, Amsterdam UMC, P.O. Box 7057, 1007 MB Amsterdam, The Netherlands; j.verhoeff@amsterdamumc.nl (J.V.); [email protected] (J.J.G.V.) 4 Department for Surgery, Amsterdam UMC, University of Amsterdam, Cancer Center Amsterdam, P.O. -

Consumer Medicine Information
DBL™ Docetaxel Concentrated Injection docetaxel Consumer Medicine Information What is in this leaflet It works by stopping cells from • wheezing or difficulty breathing growing and multiplying. or a tight feeling in your chest This leaflet answers some common Ask your doctor if you have any • swelling of the face, lips, tongue questions about DBL Docetaxel, questions about why this medicine or other parts of the body Concentrated Injection. has been prescribed for you. • rash, itching, hives or flushed, red It does not contain all the available Your doctor may have prescribed it skin information. It does not take the for another reason. • dizziness or light-headedness place of talking to your doctor or This medicine is not addictive. • back pain pharmacist. This medicine is available only with Do not use DBL Docetaxel, All medicines have risks and a doctor’s prescription. benefits. Your doctor has weighed Concentrated Injection if you have, You may have taken another the risks of you taking DBL or have had, any of the following Docetaxel, Concentrated Injection medicine to treat your breast, non medical conditions: small cell lung cancer, ovarian, against the benefits they expect it • severe liver problems prostate or head and neck cancer. will have for you. • blood disorder with a reduced However, your doctor has now number of white blood cells If you have any concerns about decided to treat you with docetaxel. taking this medicine, ask your There is not enough information to Do not use this medicine if you are doctor or pharmacist. recommend the use of this medicine pregnant or intend to become Keep this leaflet with the medicine. -

Vorinostat—An Overview Aditya Kumar Bubna
E-IJD RESIDENTS' PAGE Vorinostat—An Overview Aditya Kumar Bubna Abstract From the Consultant Vorinostat is a new drug used in the management of cutaneous T cell lymphoma when the Dermatologist, Kedar Hospital, disease persists, gets worse or comes back during or after treatment with other medicines. It is Chennai, Tamil Nadu, India an efficacious and well tolerated drug and has been considered a novel drug in the treatment of this condition. Currently apart from cutaneous T cell lymphoma the role of Vorinostat for Address for correspondence: other types of cancers is being investigated both as mono-therapy and combination therapy. Dr. Aditya Kumar Bubna, Kedar Hospital, Mugalivakkam Key Words: Cutaneous T cell lymphoma, histone deacytelase inhibitor, Vorinostat Main Road, Porur, Chennai - 600 125, Tamil Nadu, India. E-mail: [email protected] What was known? • Vorinostat is a histone deacetylase inhibitor. • It is an FDA approved drug for the treatment of cutaneous T cell lymphoma. Introduction of Vorinostat is approximately 9. Vorinostat is slightly Vorinostat is a histone deacetylase (HDAC) inhibitor, soluble in water, alcohol, isopropanol and acetone and is structurally belonging to the hydroxymate group. Other completely soluble in dimethyl sulfoxide. drugs in this group include Givinostat, Abexinostat, Mechanism of action Panobinostat, Belinostat and Trichostatin A. These Vorinostat is a broad inhibitor of HDAC activity and inhibits are an emergency class of drugs with potential anti- class I and class II HDAC enzymes.[2,3] However, Vorinostat neoplastic activity. These drugs were developed with the does not inhibit HDACs belonging to class III. Based on realization that apart from genetic mutation, alteration crystallographic studies, it has been seen that Vorinostat of HDAC enzymes affected the phenotypic and genotypic binds to the zinc atom of the catalytic site of the HDAC expression in cells, which in turn lead to disturbed enzyme with the phenyl ring of Vorinostat projecting out of homeostasis and neoplastic growth. -

Hodgkin Lymphoma Treatment Regimens
HODGKIN LYMPHOMA TREATMENT REGIMENS (Part 1 of 5) Clinical Trials: The National Comprehensive Cancer Network recommends cancer patient participation in clinical trials as the gold standard for treatment. Cancer therapy selection, dosing, administration, and the management of related adverse events can be a complex process that should be handled by an experienced health care team. Clinicians must choose and verify treatment options based on the individual patient; drug dose modifications and supportive care interventions should be administered accordingly. The cancer treatment regimens below may include both U.S. Food and Drug Administration-approved and unapproved indications/regimens. These regimens are provided only to supplement the latest treatment strategies. These Guidelines are a work in progress that may be refined as often as new significant data become available. The NCCN Guidelines® are a consensus statement of its authors regarding their views of currently accepted approaches to treatment. Any clinician seeking to apply or consult any NCCN Guidelines® is expected to use independent medical judgment in the context of individual clinical circumstances to determine any patient’s care or treatment. The NCCN makes no warranties of any kind whatsoever regarding their content, use, or application and disclaims any responsibility for their application or use in any way. Classical Hodgkin Lymphoma1 Note: All recommendations are Category 2A unless otherwise indicated. Primary Treatment Stage IA, IIA Favorable (No Bulky Disease, <3 Sites of Disease, ESR <50, and No E-lesions) REGIMEN DOSING Doxorubicin + Bleomycin + Days 1 and 15: Doxorubicin 25mg/m2 IV push + bleomycin 10units/m2 IV push + Vinblastine + Dacarbazine vinblastine 6mg/m2 IV over 5–10 minutes + dacarbazine 375mg/m2 IV over (ABVD) (Category 1)2-5 60 minutes. -

Idelalisib Post Allogeneic Hematopoietic Stem Cell Transplant (Hsct) in B Cell Derived Malignancies: a Phase 1 Double Blinded Randomized Placebo Toxicity Trial
Johns Hopkins Protocol ID: J1633 IND: 131805 IDELALISIB POST ALLOGENEIC HEMATOPOIETIC STEM CELL TRANSPLANT (HSCT) IN B CELL DERIVED MALIGNANCIES: A PHASE 1 DOUBLE BLINDED RANDOMIZED PLACEBO TOXICITY TRIAL Principal Investigator: Douglas E. Gladstone, MD Associate Professor of Oncology CRB I, Room 287 1650 Orleans Street Baltimore, MD 21287 [email protected] Co-Investigators: Javier Bolanos Meade, MD Richard Jones, MD Richard Ambinder. MD Lode Swinnen, MD Statisticians: Marianna Zahurak Study Site: Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins IRB Number: IRB00157704 IND: 131805 Version Date: February 3, 2020 Version Date: February 3, 2020 Page 1 of 31 Johns Hopkins Protocol ID: J1633 IND: 131805 Version Date: February 3, 2020 Page 2 of 31 Johns Hopkins Protocol ID: J1633 IND: 131805 CONTENTS 1. Introduction................................................................................................................................... 5 1.1. Hypothesis ..................................................................................................................................... 6 2. Objectives ...................................................................................................................................... 6 2.1. Primary Endpoint ........................................................................................................................... 6 2.2. Secondary Endpoint ...................................................................................................................... 6