Development of a Novel, Accurate, Automated, Rapid, High-Throughput Technique Suitable for Population-Based Carrier Screening for Fragile X Syndrome Charles M
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Blotting Techniques Blotting Is the Technique in Which Nucleic Acids Or
Blotting techniques Blotting is the technique in which nucleic acids or proteins are immobilized onto a solid support generally nylon or nitrocellulose membranes. Blotting of nucleic acid is the central technique for hybridization studies. Nucleic acid labeling and hybridization on membranes have formed the basis for a range of experimental techniques involving understanding of gene expression, organization, etc. Identifying and measuring specific proteins in complex biological mixtures, such as blood, have long been important goals in scientific and diagnostic practice. More recently the identification of abnormal genes in genomic DNA has become increasingly important in clinical research and genetic counseling. Blotting techniques are used to identify unique proteins and nucleic acid sequences. They have been developed to be highly specific and sensitive and have become important tools in both molecular biology and clinical research. General principle The blotting methods are fairly simple and usually consist of four separate steps: electrophoretic separation of protein or of nucleic acid fragments in the sample; transfer to and immobilization on paper support; binding of analytical probe to target molecule on paper; and visualization of bound probe. Molecules in a sample are first separated by electrophoresis and then transferred on to an easily handled support medium or membrane. This immobilizes the protein or DNA fragments, provides a faithful replica of the original separation, and facilitates subsequent biochemical analysis. After being transferred to the support medium the immobilized protein or nucleic acid fragment is localized by the use of probes, such as antibodies or DNA, that specifically bind to the molecule of interest. Finally, the position of the probe that is bound to the immobilized target molecule is visualized usually by autoradiography. -

Southern Blotting Teacher’S Guidebook
PR139 G-Biosciences ♦ 1-800-628-7730 ♦ 1-314-991-6034 ♦ [email protected] A Geno Technology, Inc. (USA) brand name Southern Blotting Teacher’s Guidebook (Cat. # BE-315) think proteins! think G-Biosciences www.GBiosciences.com MATERIALS INCLUDED ....................................................................................................... 3 SPECIAL HANDLING INSTRUCTIONS ................................................................................... 3 ADDITIONAL EQUIPMENT REQUIRED ................................................................................ 3 TIME REQUIRED ................................................................................................................. 3 AIMS .................................................................................................................................. 4 BACKGROUND ................................................................................................................... 4 TEACHER’S PRE EXPERIMENT SET UP ................................................................................ 5 PREPARATION OF AGAROSE GEL ................................................................................... 5 PREPARE THE DNA LADDER ........................................................................................... 5 PREPARE DILUTE DNA STAINING SOLUTION .................................................................. 5 MATERIALS FOR DEMONSTRATION ................................................................................... 6 DEMONSTRATION -

Bioanalytical Chemistry 4. Gel Electrophoresis
73 Bioanalytical chemistry 4. Gel Electrophoresis Required reading: Sections 9.1, 9.2.3, 9.2.4, 9.5.1, 10.1 to 10.7, 11.1 to 11.5, and 15.5 of Mikkelsen and Cortón, Bioanalytical Chemistry Some objectives for this section ⇒ You will know what DNA agarose gel electrophoresis is ⇒ You will know what the difference between normal and pulsed field electrophoresis of DNA ⇒ You will know what SDS-PAGE is. ⇒ You will understand how the basis for molecular basis for size-based separation of proteins by SDS- PAGE. ⇒ You will know what IEF is. ⇒ You will know how SDS-PAGE and IEF can be combined in 2-dimensional gel electroophoresis ⇒ You will know what a Western Blot is. ⇒ You will appreciate how these techniques can be used in the analysis of DNA and proteins. Primary Source Material • Chapter 4 and 6 of Biochemistry: Berg, Jeremy M.; Tymoczko, John L.; and Stryer, Lubert (NCBI bookshelf). • Chapter 3 and 7 of Molecular Cell Biology 4th ed. (Ch. 9, 5th ed.): Lodish, Harvey; Berk, Arnold; Zipursky, S. Lawrence; Matsudaira, Paul; Baltimore, David; Darnell, James E. (NCBI bookshelf). • Chapter 12 of Introduction to Genetic Analysis Anthony: J.F. Griffiths, Jeffrey H. Miller, David T. Suzuki, Richard C. Lewontin, William M. Gelbart (NCBI bookshelf). • Some animations are from http://www.wiley-vch.de/books/info/3-527-30300-6/. • http://www.piercenet.com/ Electrophoresis 74 The velocity of migration (v) of a molecule in an electric field depends on the electric field strength (E), the net charge on the protein (z), and the frictional coefficient (f). -

Blotting Techniques M.W
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Elsevier - Publisher Connector RESEARCH TECHNIQUES MADE SIMPLE North, South, or East? Blotting Techniques M.W. Nicholas1 and Kelly Nelson2 Journal of Investigative Dermatology (2013) 133, e10; doi:10.1038/jid.2013.216 One of the cornerstones of modern molecular biology, blotting is a powerful and sensitive technique for identifying WHAT BLOTTING DOES the presence of specific biomolecules within a sample. • Blotting allows specific and sensitive detection of a Subtypes of blotting are differentiated by the target protein (western) or specific DNA or RNA sequence molecule that is being sought. The first of these tech (Southern, northern) within a large sample isolate. niques developed was the Southern blot, named for Dr. • Targets are first separated by size/charge via gel Edwin Southern, who developed it to detect specific DNA electrophoresis and then identified using a very sequences (Southern, 1975). Subsequently, the method was sensitive probe. modified to detect other targets. The nomenclature of these • Variations of these techniques can detect post techniques was built around Dr. Southern’s name, resulting translational modifications and DNAbound proteins. in the terms northern blot (for detection of RNA), western blot (for detection of protein), eastern blot (for detection • Western blotting may also be used to detect a of posttranslationally modified proteins), and south circulating antibody in a patient sample or confirm western blot (for detection of DNA binding proteins). Most an antibody’s specificity. researchers consider the eastern blot and the southwestern blot variations of western blots rather than distinct entities. -

Non-Radioactive Southern Blot Reagents Store As Labeled
Product Specifications Non-Radioactive Southern Blot Analysis, Electrophoresis Reagents Polymerase Chain Reaction Reagents, Omni-Pure Reagents, Hybridization and Detection Reagents, Custom Primers and Probes Non-Radioactive Southern Blot Reagents Store as labeled. For research use only. Catalog Number Description Unit Size 40-3010-10 Agarose LE Molecular Biology Grade 100 gms 40-5023-20 Lumisol II Hybridization Solution; for non-toxic hybridizations; 200 mL 200 mL 40-5024-20 Lumisol III Hybridization Solution; for oligonucleotide probes; 200 mL 200 mL 40-5010-10 CDP-Star® Substrate; Ready-to-Use 0.25 mM in spray bottle; 10 mL 10 mL 40-5020-25 Hybwash A, Hybridization Wash Solution Concentrate( 20X SSC); 250 mL 250 mL 40-5021-10 Hybwash B, Hybridization Wash Solution Concentrate (10% SDS); 100 mL 100 mL 40-5025-20 Maleic acid buffer 10X (Buffer M 10X); 200 mL 200 mL 40-5025-50 Maleic acid buffer 10X (Buffer M 10X); 500 mL 500 mL 40-5026-10 Blocking solution for hybridization (10%); 100 mL 100 mL 40-5031-10 AP Detection buffer 10X (Alkaline Phosphatase buffer); 100 mL 100 mL 40-5034-10 Depurination Solution (2X) for Southern Blotting; 1 L 1 L 40-5035-10 Denaturation Solution (2X) for Southern Blotting; 1L 1 L 40-5036-10 Neutralization Solution (2X) for Southern Blotting; 1L 1 L Lumisol II Hybridization Solution; for non-toxic hybridizations; 200 mL Catalog Number 40-5023-20 Lumisol III Hybridization Solution; for oligonucleotide probes; 200 mL Catalog Number 40-5024-20 Storage: Room Temperature. Below 22°C precipitates may appear. Warm to 40°C and gently swirl to dissolve the precipitates. -
Southern and Western Blot Techniques, Dna Profiling
RASAQ NURUDEEN OLAJIDE LECTURE CONTENT INTRODUCTION SOUTHERN BLOTTING WESTERN BLOTTING DNA PROFILING (DNA FINGERPRINTING) PARENTAL TESTING PROCEDURES INTRODUCTION Then the Lord said to Cain, ”Where is your brother Abel?” He said,” I do not know; am I my brother’s keeper?” And the Lord said “What have you done? Listen; your brother’s blood is crying out to me from the ground!”-Genesis 4:9-10 DNA: a true marker of identity FORENSIC SCIENCE Definition – Relating to the use of science or technology in the investigation and establishment of facts or evidence in a court of law. Source – From the Latin word Forum. The Forum was a public gathering place during Roman times, where judicial activities and public business was conducted. HISTORY OF FORENSIC SCIENCE Many people believe that Arthur Conan Doyle was the first to popularize forensic science with his Sherlock Holmes novels. The first, A Study in Scarlet, was published in 1887. WHAT IS BLOTTING? Blots are techniques for transferring DNA , RNA and proteins onto a carrier so they can be separated, and often follows the use of a gel electrophoresis. The Southern blot is used for transferring DNA, the Northern blot for RNA and the western blot for PROTEIN. TYPES OF BLOTTING TECHNIQUES Blotting technique Western blot Southern Blot Northern Blot It is used to detect It is used to detect DNA. It is used to detect RNA. protein. SOUTHERN BLOTTING Professor Sir Edwin Southern, Professor of Biochemistry and Fellow of Trinity developed this method in 1975. Southern won the Lasker Award for Clinical Medical Research prize for the method of finding specific DNA sequences he developed this procedure at Edinburgh University more than 30 years ago. -

Use of Synthetic Oligonucleotides As Hybridization Probes
Proc. NatL Acad. Sci. USA Vol. 78, No. 11, pp. 6613-6617, November 1981 Biochemistry Use of synthetic oligonucleotides as hybridization probes: Isolation of cloned cDNA sequences for human p2-microglobulin* (mixed sequence oligonucleotides/colony screening) SIDNEY V. SUGGS, R. BRUCE WALLACE, TADAAKI HIROSEt, ERIC H. KAWASHIMAt, AND KEIICHI ITAKURA§ Division of Biology, Molecular Genetics Section, City of Hope Research Institute, Duarte, California 91010 Communicated byJames F. Bonner, June 22, 1981 ABSTRACT We have synthesized two sets of 15-base-long Table 1. Oligonucleotide probes for the isolation of 2m oligodeoxyribonucleotides corresponding to all possible coding se- quences for a small portion of human fl2-microglobulin. Labeled 95 96 97 98 99 oligonucleotides were used as hybridization probes to screen bac- Amino acid sequence Trp Asp Arg Asp Met terial clones containing cDNA sequences primed with oligo(dT) Possible codons 5' UGG GAC} AGG GACJ AUG 3' and inserted into the plasmid vector pBR322. One A-microglob- CGN ulin cDNA clone was detected in the 535 bacterial plasmid clones Probe PmI 3' ACC CTG TCT CTG TAC 5' that were screened. The clone has been characterized by blotting Probe P2mll 3' ACC CTG GCN CTG TAC 5' and nucleotide sequence analysis. The cloned P2-microglobulin 75 76 77 78 sequence contains 217 base pairs of the 3' untranslated region of Amino acid sequence Lys Asp Glu Tyr the mRNA and 328 base pairs (97%) of the coding region. Possible codons 5' AAM GAC GAM UAg 3' The hybridization properties ofoligodeoxyribonucleotides have Probe jAmM 3' TTc CTG CTC AT 5' been characterized by a number of techniques (1-4). -

Analysis of Human Mitochondrial DNA Content by Southern Blotting and Nonradioactive Probe Hybridization
Southern Illinois University Carbondale OpenSIUC Articles Biochemistry & Molecular Biology 4-14-2019 Analysis of Human Mitochondrial DNA Content by Southern Blotting and Nonradioactive Probe Hybridization. Joel H Wheeler Carolyn K J Young Matthew J ounY g Follow this and additional works at: https://opensiuc.lib.siu.edu/bmb_articles This is the peer reviewed version of the article cited below, which has been published in final form at Current Protocols in Toxicology. This article may be used for non-commercial purposes in accordance with Wiley Terms and Conditions for Self-Archiving. Recommended Citation Wheeler, Joel H, Young, Carolyn K J and Young, Matthew J. "Analysis of Human Mitochondrial DNA Content by Southern Blotting and Nonradioactive Probe Hybridization.." Curr Protoc Toxicol (Apr 2019). doi:10.1002/cptx.75. This Article is brought to you for free and open access by the Biochemistry & Molecular Biology at OpenSIUC. It has been accepted for inclusion in Articles by an authorized administrator of OpenSIUC. For more information, please contact [email protected]. [*This is a protocol for inclusion in CPTX volume 81. There are 6 Figures and 1 Table. There is an included PMC file.] Analysis of human mitochondrial DNA content by Southern blot and non- radioactive probe hybridization A Southern blot and non-radioactive probe hybridization method to estimate human mitochondrial DNA content Joel H. Wheeler1,2, Carolyn K. J. Young,1,3 and Matthew J. Young1,* 1Department of Biochemistry and Molecular Biology, Southern Illinois University School of Medicine, Carbondale, Illinois 62901 [email protected] [email protected] *Correspondence to [email protected] Significance Statement A single human cell can contain several thousand copies of the maternally inherited mitochondrial DNA genome or mtDNA. -
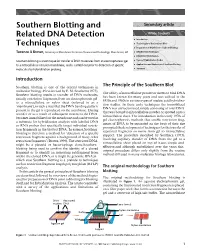
Southern Blotting and Related DNA Detection Techniques
Southern Blotting and Secondary article Related DNA Detection Article Contents . Introduction Techniques . The Principle of the Southern Blot . Preparation of DNA Prior to Southern Blotting Terence A Brown, University of Manchester Institute of Science and Technology, Manchester, UK . DNA Blotting Techniques . DNA/DNA Hybridization Southern blotting is a technique for transfer of DNA molecules from an electrophoresis gel . Types of Hybridization Probes to a nitrocellulose or nylon membrane, and is carried out prior to detection of specific . Applications and Limitations of Southern Blotting molecules by hybridization probing. Summary Introduction Southern blotting is one of the central techniques in The Principle of the Southern Blot molecular biology. First devised by E. M. Southern (1975), The ability of nitrocellulose powder or sheets to bind DNA Southern blotting results in transfer of DNA molecules, has been known for many years and was utilized in the usually restriction fragments,from an electrophoresis gel 1950s and 1960s in various types of nucleic acid hybridiza- to a nitrocellulose or nylon sheet (referred to as a tion studies. In these early techniques the immobilized ‘membrane’),in such a way that the DNA banding pattern DNA was unfractionated,simply consisting of total DNA present in the gel is reproduced on the membrane. During that was bound to nitrocellulose powder or spotted onto a transfer or as a result of subsequent treatment,the DNA nitrocellulose sheet. The introduction in the early 1970s of becomes immobilized on the membrane and can be used as gel electrophoresis methods that enable restriction frag- a substrate for hybridization analysis with labelled DNA ments of DNA to be separated on the basis of their size or RNA probes that specifically target individual restric- prompted the development of techniques for the transfer of tion fragments in the blotted DNA. -

Southern Blotting
Southern Blotting Prepared by Dr. Subhadeep Sarker Associate Professor, Department of Zoology for UG & PG Studies, Serampore College Introduction • A Southern blot is a method routinely used for detection of a specific DNA sequence in DNA samples. • Southern blotting involves transfer of electrophoresis- separated DNA fragments to a filter membrane and subsequent fragment detection by hybridization with a suitable probe. • The method is named after its inventor, the British biologist E. M. Southern. Other blotting methods (i.e., western blot, northern blot, eastern blot, southwestern blot) that employ similar principles, but using RNA or protein, have later been named in reference to Southern’s name. • The amount of DNA needed for this technique is dependent on the size and specific activity of the probe. Short probes tend to be more specific. Under optimal conditions, one can expect to detect 0.1 pg of the DNA. Dr. Subhadeep Sarker Method • DNA Digestion by Restriction Endonuclease: A suitable restriction endonuclease is used to cleave high-molecular-weight DNA into smaller fragments. • Electrophoresis: The DNA fragments are then run by electrophoresis on an agarose gel to separate them by size. Dr. Subhadeep Sarker Method: Depurination • Depurination (Optional): If some of the DNA fragments are larger than 15 kb, then prior to blotting, the gel may be treated with an acid, such as dilute HCl, which depurinates the DNA fragments, breaking the DNA into smaller pieces, thus allowing more efficient transfer from the gel to membrane. • A depurination step is optional. Fragments greater than 15 kb are hard to transfer to the blotting membrane. -

Experiment Objective
The Biotechnology Education Company ® sed Revi nd a ated Upd EDVO-Kit # 311 DNA Fingerprinting III: Southern Blot Analysis Storage: See Page 3 for specifi c storage instructions EXPERIMENT OBJECTIVE: This experiment introduces students to Southern Blot analysis used in DNA Fingerprinting for a hypothetical paternity determination. EDVOTEK, Inc. • 1-800-EDVOTEK • www.edvotek.com EVT 2012_04_12AM 331111 DNA Fingerprinting III: Southern Blot Analysis Experiment Table of Contents Page Experiment Components 3 Experiment Requirements 4 Background Information 5 Experiment Procedures Experiment Overview and General Instructions 13 Module I: Agarose Gel Electrophoresis 14 Module II: Southern Blot Transfer 16 Module III: Non-Isotopic Detection of DNA 19 Study Questions 22 Instructor's Guidelines Notes to the Instructor 24 Pre-Lab Preparations 27 Experiment Results and Analysis 29 Study Questions and Answers 30 Appendices A Agarose Gel Preparation For Southern Blot Analysis 32 B Quantity Preparations for Agarose Gel Electrophoresis 33 C Staining and Visualization of DNA with InstaStain® Ethidium Bromide Cards 34 Material Safety Data Sheets 35 All components are intended for educational research only. They are not to be used for diagnostic or drug purposes, nor administered to or consumed by humans or animals. EDVOTEK and The Biotechnology Education Company are registered trademarks of EDVOTEK, Inc. The Biotechnology Education Company® • 1-800-EDVOTEK • www.edvotek.com 2 DNA Fingerprinting III: Southern Blot Analysis 331111 Experiment Experiment Components -

Memorial Symposium
Memorial Symposium Biomedicum Lecture Hall 1 Monday, May 31 at 9-11 am Special tribute to Academician of Science Leena Peltonen From Individuals to Populations – now and then ANTTI SAJANTILA, MD, PhD, professor Hjelt Institute Department of Forensic Medicine University of Helsinki ContentContent Genetics and identification of individuals Identification of Populations Studies of Past Populations ContentContent Genetics and identification of individuals Identification of Populations Studies of Past Populations Early days of forensic genetics - serology 1901: Karl Landsteiner discovered the human blood groups AB0 (and Rh in 1940) 1925: "secretor" status described – 80% have blood group substances in their body fluids 1932: Leon Lattes finds method for AB0 typing of dried blood flakes 1950's: electrophoresis of serum proteins Revolution in forensic DNA analysis Nature 314:67-73 (1985) The „Gold Rush“ ~1986-89 Commercialisation of forensic DNA analysis: - new opportunities for professional services - lack of standards, quality control and assurance - premature introduction into casework … and the downfall Castro Case (New York, 1989) - Admissibility of DNA challenged in pretrial hearings - Evidence to prove presence of the suspect's DNA was dismissed due to lack of standards and biased interpretation Experts vs Experts ~1990-95 Differences within population may be greater that between populations due to subgroups not conforming to Hardy-Weinberg equilibrium (Lewontin & Hartl, Science 1991) 1992: National Research Council (NRC)