Primary Cysts of the Iris
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Affections of Uvea Affections of Uvea
AFFECTIONS OF UVEA AFFECTIONS OF UVEA Anatomy and physiology: • Uvea is the vascular coat of the eye lying beneath the sclera. • It consists of the uvea and uveal tract. • It consists of 3 parts: Iris, the anterior portion; Ciliary body, the middle part; Choroid, the third and the posterior most part. • All the parts of uvea are intimately associated. Iris • It is spongy having the connective tissue stroma, muscular fibers and abundance of vessels and nerves. • It is lined anteriorly by endothelium and posteriorly by a pigmented epithelium. • Its color is because of amount of melanin pigment. Mostly it is brown or golden yellow. • Iris has two muscles; the sphincter which encircles the pupil and has parasympathetic innervation; the dilator which extends from near the sphincter and has sympathetic innervation. • Iris regulates the amount of light admitted to the interior through pupil. • The iris separates the anterior chamber from the posterior chamber of the eye. Ciliary Body: • It extends backward from the base of the iris to the anterior part of the choroid. • It has ciliary muscle and the ciliary processes (70 to 80 in number) which are covered by ciliary epithelium. Choroid: • It is located between the sclera and the retina. • It extends from the ciliaris retinae to the opening of the optic nerve. • It is composed mainly of blood vessels and the pigmented tissue., The pupil • It is circular and regular opening formed by the iris and is larger in dogs in comparison to man. • It contracts or dilates depending upon the light source, due the sphincter and dilator muscles of the iris, respectively. -

Glaucoma Related to Ocular and Orbital Tumors Sonal P
Chapter Glaucoma Related to Ocular and Orbital Tumors Sonal P. Yadav Abstract Secondary glaucoma due to ocular and orbital tumors can be a diagnostic challenge. It is an essential differential to consider in eyes with a known tumor as well as with unilateral, atypical, asymmetrical, or refractory glaucoma. Various intraocular neoplasms including iris and ciliary body tumors (melanoma, metasta- sis, lymphoma), choroidal tumors (melanoma, metastasis), vitreo-retinal tumors (retinoblastoma, medulloepithelioma, vitreoretinal lymphoma) and orbital tumors (extra-scleral extension of choroidal melanoma or retinoblastoma, primary orbital tumors) etc. can lead to raised intraocular pressure. The mechanisms for glaucoma include direct (tumor invasion or infiltration related outflow obstruction, tra- becular meshwork seeding) or indirect (angle closure from neovascularization or anterior displacement or compression of iris) or elevated episcleral venous pressure secondary to orbital tumors. These forms of glaucoma need unique diagnostic techniques and customized treatment considerations as they often pose therapeutic dilemmas. This chapter will review and discuss the mechanisms, clinical presenta- tions and management of glaucoma related to ocular and orbital tumors. Keywords: ocular tumors, secondary glaucoma, orbital tumors, angle infiltration, neovascular glaucoma, neoplastic glaucoma 1. Introduction With the advent of constantly evolving and advancing ophthalmic imaging tech- niques as well as surgical modalities in the field of ophthalmic diseases, diagnostic accuracy, and treatment outcomes of ocular as well as orbital tumors have improved remarkably over the past few years. Raised intraocular pressure (IOP) is known to be one of the presenting features or associated finding for numerous ocular as well as orbital tumors. Ocular and orbital tumors can cause secondary glaucoma due to various mechanisms. -

Primary Pupillary Margin Cyst of the Iris Pigment Epithelium
Chinese Medicine, 2011, 2, 16-19 doi:10.4236/cm.2011.21003 Published Online March 2011 (http://www.SciRP.org/journal/cm) Primary Pupillary Margin Cyst of the Iris Pigment Epithelium Rosanna Dammacco1, Giovanni Giancipoli1, Silvana Guerriero1, Domenico Piscitelli2, Nicola Cardascia1 1Department of Ophthalmology and Otorhinolaryngology, Bari University, Bari, Italy 2Department of Pathological Anatomy, Bari University, Bari, Italy E-mail: [email protected] Received January 13, 2011; revised February 2, 2011; accepted February 10, 2011 Abstract Purpose: Description of a patient with a solitary cyst of the pupillary margin iris pigment epithelium (IPE). Methods: A 63-year-old man referred a suspected iris-ciliary body melanoma in his left eye. Based on both clinical examination and ultrasound biomicroscopy, melanoma was considered unlikely. Surgery was under- taken to correct recurrent deterioration of vision due to movement of the lesion across the visual axis. Results: The lesion was excised completely. Ultrasound biomicroscopy and histopathological examination ruled out melanoma and allowed a final diagnosis of primary pupillary margin cyst of the IPE, characterized of pig- mented epithelium, with no connective tissue or vessels. No recurrences or fresh lesions appeared during a one-year follow-up. Conclusions: Primary epithelial iris cysts are usually benign. Treatment is required only in symptomatic patients and those with an uncertain diagnosis. Ultrasound biomicroscopy is indispensable to confirm the clinical diagnosis, follow the clinical course and intervene if surgery is required. Keywords: Melanoma, Iris Pigment Epithelium, Pupillary Cyst, Surgical Excision, Ultrasound Biomicroscopy 1. Introduction This paper describes a case of symptomatic primary central IPE cyst initially mistaken for an iris melanoma. -
ICO Residency Curriculum 2Nd Edition and Updated Community Eye Health Section
ICO Residency Curriculum 2nd Edition and Updated Community Eye Health Section The International Council of Ophthalmology (ICO) Residency Curriculum offers an international consensus on what residents in ophthalmology should be taught. While the ICO curriculum provides a standardized content outline for ophthalmic training, it has been designed to be revised and modified, with the precise local detail for implementation left to the region’s educators. Download the Curriculum from the ICO website: icoph.org/curricula.html. www.icoph.org Copyright © International Council of Ophthalmology 2016. Adapt and translate this document for your noncommercial needs, but please include ICO credit. All rights reserved. First edition 201 6 . First edition 2006, second edition 2012, Community Eye Health Section updated 2016. International Council of Ophthalmology Residency Curriculum Introduction “Teaching the Teachers” The International Council of Ophthalmology (ICO) is committed to leading efforts to improve ophthalmic education to meet the growing need for eye care worldwide. To enhance educational programs and ensure best practices are available, the ICO focuses on "Teaching the Teachers," and offers curricula, conferences, courses, and resources to those involved in ophthalmic education. By providing ophthalmic educators with the tools to become better teachers, we will have better-trained ophthalmologists and professionals throughout the world, with the ultimate result being better patient care. Launched in 2012, the ICO’s Center for Ophthalmic Educators, educators.icoph.org, offers a broad array of educational tools, resources, and guidelines for teachers of residents, medical students, subspecialty fellows, practicing ophthalmologists, and allied eye care personnel. The Center enables resources to be sorted by intended audience and guides ophthalmology teachers in the construction of web-based courses, development and use of assessment tools, and applying evidence-based strategies for enhancing adult learning. -

Posterior Uveal (Ciliary Body and Choroidal) Melanoma Leslie T
Posterior Uveal (Ciliary Body and Choroidal) Melanoma Leslie T. L. Pham, MD, Jordan M. Graff, MD, and H. Culver Boldt, MD July 27, 2010 Chief Complaint: 31-year-old man with "floaters and blurry vision" in the right eye (OD). History of Present Illness: In August 2007, a healthy 31-year-old truck driver from Nebraska started noticing floaters in his right eye. The floaters gradually worsened and clouded his central vision. His family doctor tried changing his blood pressure medications, but this did not help. He later saw an ophthalmologist in his home state who told him there was a "mass" in his right eye. He was referred to the University of Iowa Department of Ophthalmology and Visual Sciences. Past Ocular History: The patient has had no prior eye surgery or trauma. Past Medical History: The patient reports prior excision of a benign skin nevus. He also has hypertension. Medications: Metoprolol and triamterene/hydrochlorothiazide Family History: The patient’s mother has a history of neurofibromatosis. His father had an enucleation for an "eye cancer" and subsequently died due to metastatic spread of the cancer. His grandmother had skin melanoma. Social History: The patient lives in Nebraska with his wife and child. He has never smoked and only drinks on "special occasions". Review of Systems: Negative, except as noted above. Ocular Examination: General: Well-developed, well-nourished Caucasian man in a pleasant mood Skin: Several scattered macules and papules on the trunk and all four extremities Distance visual acuity (without correction): o 20/60-2 OD o 20/20 OS Near acuity (without correction) o 20/30 OD o 20/20 OS Ocular motility: Full OU. -

Ophthalmic Pathology and Oncology A) Pathology
Ophthalmic pathology and oncology Objective Understanding the pathophysiology and oncology of the eye and in systemic diseases and their presentations. Differentiation of benign and malignant eye diseases, understanding the pathology and examination techniques with focus on the main risk factors of the disease. Recognising signs and symptoms of the disease with diagnostic tests at the slit lamp as well as functional and structural analysis. Management of presentation, including various therapeutic options (medical and surgical) and follow-up. Psychology and management of patients presenting with a potentially blinding and life-threatening disease. A) Pathology Anatomy and pathophysiology of: -Ocular anatomy and histology of the major structures of the eye and its adnexa: • Conjunctiva • Cornea • Sclera • Anterior chamber • Posterior chamber • Iris • Ciliary body • Lens • Vitreous • Retina and retinal pigment epithelium • Choroid • Optic nerve • Visual pathway • Eyelids • Extraocular muscles • Lacrimal system • Orbit Disease process • Congenital anomaly • Choristoma versus hamartoma Inflammation • Acute versus chronic • Focal versus diffuse • Granulomatus versus nongranulomatous Degeneration (includes dystrophy) Neoplasia • Benign versus malignant • Epithelial versus soft tissue versus haematopoietic -Basic pathophysiology of the common disease processes of the eye and its adnexa, and identify the major histologic findings: a. Degeneration (e.g., pterygium, keratoconus) b. Dystrophy (e.g., Fuchs’ dystrophy, TGFBI-associated dystrophies) c. Infection (e.g., fungal keratitis, bacterial endophthalmitis) d. Inflammation (e.g., chalazion, idiopathic orbital inflammation) e. Neoplasm and proliferation (e.g., basal and squamous cell carcinoma, uveal melanoma, retinoblastoma) - Pathophysiology and identify the major histologic findings of common diseases of the eye (e.g., keratitis, exfoliation syndrome, corneal and retinal dystrophies and degenerations, frequent neoplasms, oculoplastics, cornea, glaucoma, retina, ophthalmic oncology). -

Download Report Appendixes [PDF · 224
Appendices Appendix A. Selected Internet Links Appendix Table A1. Internet links for radiotherapy organizations Organization URL address Deutsche Gesellschaft fur http://www.degro.org/jsp_public/cms/index.jsp Radiooncologie European Society for Therapeutic http://www.estroweb.org/estro/index.cfm Radiology and Oncology American Society for Therapeutic http://www.astro.org/ Radiology and Oncology National Association for Proton http://www.proton-therapy.org/ Therapy Particle Therapy Cooperative http://ptcog.web.psi.ch/ Group (Accessed June 16, 2008) Appendix Table A2. Internet links for particle beam instrumentation companies Company URL address Ion Beam Applications (IBA) http://www.iba-worldwide.com/ Solutions Still River Systems Inc http://www.stillriversystems.com/ Optivus Proton Therapy http://www.optivus.com/ Siemens http://www.medical.siemens.com/ Hitachi: Proton beam Therapy http://www.pi.hitachi.co.jp/rd-eng/product/industrial-sys/accelerator- sys/proton-therapy-sys/proton-beam-therapy/index.html ACCEL Instruments http://www.proton-therapy.com/ (Accessed June 16, 2008) Appendix Table A3. Internet links for particle beam treatment centers in the USA Center/Institute URL address Francis H. Burr Proton Therapy http://www.massgeneral.org/cancer/about/providers/radiation/proton/i Center (NPTC) ndex.asp Loma Linda University Proton http://www.llu.edu/proton/index.html Therapy Center University of California, Crocker http://media.cnl.ucdavis.edu/crocker/website/default.php Nuclear Lab Midwest Proton Radiotherapy http://www.mpri.org/ Institute, Bloomington M.D. Anderson Proton Therapy http://www.mdanderson.org/care_centers/radiationonco/ptc/ Center, Houston University of Florida Proton http://www.floridaproton.org/ Therapy Institute, Jacksonville (Accessed June 16, 2008) A-1 Appendix B. -

Pigmented Iris Cyst in Vitreous Chamber Nimesh Patel,1 Rajeev Reddy Pappuru,1 Soumyava Basu,2 Mudit Tyagi1,2
BMJ Case Rep: first published as 10.1136/bcr-2020-239431 on 13 December 2020. Downloaded from Images in… Pigmented iris cyst in vitreous chamber Nimesh Patel,1 Rajeev Reddy Pappuru,1 Soumyava Basu,2 Mudit Tyagi1,2 1Smt Kanuri Santhamma Center DESCRIPTION Patient’s perspective for Vitreoretinal Diseases, LV A- 45- year old male patient, diagnosed elsewhere as Prasad Eye Institute, Hyderabad, retinal detachment, was seen in the retina services I had a black shadow moving in my eye, and Telangana, India of our institute. There was no history of prior 2Uveitis and Ocular Immunology after the surgery, my vision is more clear and the ocular trauma or surgery. His vision was 20/20 in Services, LV Prasad Eye Institute, shadow has gone. Hyderabad, India his right eye and 20/125 in the left eye. There were no signs of any ocular inflammation and the intra- Correspondence to ocular pressure was within normal limit. A retinal Dr Mudit Tyagi; evaluation revealed a free-floating pigmented Learning points drmudittyagi@ gmail. com cyst in vitreous cavity (figure 1,white arrow). A pars plana vitrectomy was done and the cyst was ► Congenital vitreous cysts may be remnants Accepted 22 October 2020 removed. The histopathology was suggestive of of the hyaloid vascular system such as iris pigment cells. The pigmented cells on the cyst Bergmeister’s papilla and Mittendorf’s dot wall are more likely to originate from the ciliary or may represent choristoma of the hyaloid pigment epithelium. The cysts initially are formed vascular system. on the ciliary body and then get dislodged into the ► Acquired cysts may be associated with vitreous, giving rise to the abrupt symptom of a trauma, uveitis, uveal colobomas and retinal diminution of vision. -
Iris Lymphocytic Lesion Mimicking Amelanotic Melanoma: a Clinico-Pathologic Case Report
Advances in Ophthalmology & Visual System Case Report Open Access Iris lymphocytic lesion mimicking amelanotic melanoma: a clinico-pathologic case report Abstract Volume 3 Issue 1 - 2015 Lymphoproliferative disorders of the iris are rare, they can be benign or malignant and Azza MY Maktabi,1 Mosa AlHarby,2 Hind only few cases have been reported in the literature. We have encountered a 70 year-old 3 male patient who developed an iris mass in his left eye over a period of 1 month. He Manaa Alkatan 1Department of Pathology & Laboratory Medicine, King Khalid was referred to our tertiary eye care center with the provisional diagnosis of melanoma. Eye specialist Hospital, Saudi Arabia His clinical findings raised the suspicious of amelanotic melanoma because of the high 2Anterior Segment & Uveitis Divisions, King Khalid Eye specialist intraocular pressure in the involved eye, the noted vascularization of the mass, and the Hospital, Saudi Arabia anterior segment findings. The histopathological diagnosis of a T-cell rich lymphocytic 3Department of Ophthalmology, College of Medicine, King Saud lesion was not suspected. The clinicopathologic findings of this case are described with University, Saudi Arabia brief specific review of the literature on the topic of lymphomatous lesions of the iris. Correspondence: Hind Manaa Alkatan, Ophthalmology Keywords: amelanotic melanoma, clinicopathologic, ectropion uvea, neovascularization Department, College of Medicine, King Saud University, Riyadh, Saudi Arabia, Tel +966 504492399, Fax +966112052740, Email Received: October 22, 2015 | Published: October 30, 2015 Abbreviations: KP’S, keratic precipitates; UBM, ultrasound infero-nasally, extending from 3 to 6 o’clock, involving the pupillary biomicroscopy; OCT, optical coherence tomography margin and causing ectropion uvea. -

Iris Cysts: Clinical Features, Imaging Findings, and Treatment Results
DOI: 10.4274/tjo.galenos.2019.20633 Turk J Ophthalmol 2020;50:31-36 Ori gi nal Ar tic le Iris Cysts: Clinical Features, Imaging Findings, and Treatment Results Helin Ceren Köse, Kaan Gündüz, Melek Banu Hoşal Ankara University Faculty of Medicine, Department of Ophthalmology, Ankara, Türkiye Abstract Objectives: To report the clinical and demographic characteristics, imaging findings, treatment results, and follow-up data of patients with iris cysts. Materials and Methods: The medical records of 37 patients with iris cysts were retrospectively analyzed. Ultrasound biomicroscopy (UBM), swept-source optical coherence tomography (SS-OCT), and SS-OCT angiography (SS-OCTA) were performed to examine the iris cysts. Results: The mean age of the patients was 34.4 years, ranging from 5 to 85 years. Twenty-four patients (65%) were female and 13 (35%) were male. Mean follow-up period was 21.3 months, ranging from 4 months to 8 years. Thirty-five (94.5%) of the cysts were classified as primary and 2 (4.5%) were classified as secondary. Thirty-one (83.7%) of the primary cysts were pigment epithelial and 4 were stromal. Primary iris pigment epithelial (IPE) cysts were classified as peripheral in 26 patients (72.2%), midzonal in 4 (11.1%), and dislodged in 1 (2.7%). Stromal cysts were classified as acquired in 3 patients (8.1%) and congenital in 1 patient (2.7%). Secondary iris cysts were caused by perforating eye injury. UBM could visualize both the anterior and posterior surfaces of the cysts (26 patients). Anterior segment SS-OCT could visualize the anterior but not the posterior surface of the cysts (4 patients). -
Identifying and Managing Iris Cysts
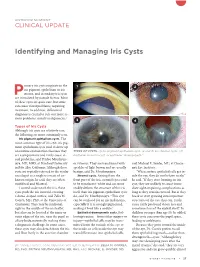
ANTERIOR SEGMENT CLINICAL UPDATE Identifying and Managing Iris Cysts rimary iris cysts originate in the 1 2 iris pigment epithelium or iris Pstroma, and secondary iris cysts are stimulated by outside factors. Most of these cysts are quite rare, but some can cause visual problems, requiring treatment. In addition, differential diagnosis is crucial to rule out more se rious problems, mainly malignancies.1 3 4 Types of Iris Cysts Although iris cysts are relatively rare, the following are more commonly seen. Iris pigment epithelium cysts. The most common type of iris cyst, iris pig ment epithelium cysts tend to show up on routine examinations because they TYPES OF CYSTS. (1) Iris pigment epithelium cyst. (2 and 3) Iris stromal cysts. (4) are asymptomatic and rarely cause vi Epithelial inclusion cyst, or epithelial “downgrowth.” sual problems, said Prithvi Mruthyun jaya, MD, MHS, at Stanford University or vitreous. They are translucent with said Michael E. Snyder, MD, at Cincin in Palo Alto, California. Although these speckles of light brown and are usually nati Eye Institute. cysts are typically referred to the ocular benign, said Dr. Mruthyunjaya. “When surface epithelial cells get in oncologist as a single iris mass of un Stromal cysts. Arising from the side the eye, they do not behave nicely,” known origin, he said, they are often front part of the iris, stromal cysts tend he said. “If they start forming an iris multifocal and bilateral. to be translucentwhite and can more cyst, they are unlikely to cause imme Located underneath the iris, these readily deform the struc ture of the iris diate sightimpairing complications as cysts push the iris forward, creating itself than iris pigment epithelium cysts long as they remain encased. -

Ocular Oncology and Pathology 2018 Hot Topics in Ocular Pathology and Oncology— an Update
Ocular Oncology and Pathology 2018 Hot Topics in Ocular Pathology and Oncology— An Update Program Directors Patricia Chévez-Barrios MD and Dan S Gombos MD In conjunction with the American Association of Ophthalmic Oncologists and Pathologists McCormick Place Chicago, Illinois Saturday, Oct. 27, 2018 Presented by: The American Academy of Ophthalmology 2018 Ocular Oncology and Pathology Subspecialty Day Advisory Committee Staff Planning Group Daniel S Durrie MD Melanie R Rafaty CMP DES, Director, Patricia Chévez-Barrios MD Associate Secretary Scientific Meetings Program Director Julia A Haller MD Ann L’Estrange, Subspecialty Day Manager Dan S Gombos MD Michael S Lee MD Carolyn Little, Presenter Coordinator Program Director Francis S Mah MD Debra Rosencrance CMP CAE, Vice R Michael Siatkowski MD President, Meetings & Exhibits Former Program Directors Kuldev Singh MD MPH Patricia Heinicke Jr, Copy Editor 2016 Carol L Shields MD Mark Ong, Designer Maria M Aaron MD Gina Comaduran, Cover Designer Patricia Chévez-Barrios MD Secretary for Annual Meeting 2014 Hans E Grossniklaus MD Arun D Singh MD ©2018 American Academy of Ophthalmology. All rights reserved. No portion may be reproduced without express written consent of the American Academy of Ophthalmology. ii Planning Group 2018 Subspecialty Day | Ocular Oncology & Pathology 2018 Ocular Oncology and Pathology Planning Group On behalf of the American Academy of Ophthalmology and the American Association of Ophthalmic Oncologists and Pathologists, it is our pleasure to welcome you to Chicago and