Screening for Lung Cancer
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Lung Cancer Screening
Care Process Model NOVEMBER 2017 A DECISION GUIDE AND PROCESS FOR Lung Cancer Screening The U.S. Preventative Services Task Force (USPSTF) recommends annual lung cancer screening for adults who have no signs or symptoms of lung cancer but who are at high risk for developing the disease because of age and smoking history. USP Based on this recommendation and studies from the National Institute of Health (NIH) NLST, Intermountain Healthcare established the Lung Cancer Screening Program with the support of the Oncology Clinical Program, the Division of Pulmonology and Critical Care Medicine, and Department of Imaging. This screening program facilitates annual screening (and more frequent diagnostic testing when indicated) for patients who meet criteria for high risk of developing lung cancer. Why Focus ON LUNG CANCER SCREENING? • Lung cancer is common. According to the American Cancer Society (ACS), GOALS nearly 225,000 cases of lung cancer are diagnosed annually. The ACS estimates The goals of the Lung Cancer Screening that over 155,000 people will die from lung cancer in 2017, representing the leading Program are as follows: cause of cancer-related mortality in both men and women.ACS A major barrier to • Identify appropriate patients for screening reducing mortality is early detection. Only 16 % are diagnosed at an early stage. ALA through primary care providers (PCPs) and other clinicians • Most high-risk patients can be identified through a simple history. • Track appropriate patients long term to About 85 % of lung cancer diagnoses are related to or caused by smoking, and the ensure that they receive annual screening and risk increases with smoking duration and frequency. -

Lung Cancer Screening What Is Lung Cancer Screening? Screening Exams Find Disease Before Symptoms Begin
Lung Cancer Screening What is lung cancer screening? Screening exams find disease before symptoms begin. The goal of screening is to detect disease at its earliest and most treatable stage. In order to be widely accepted and recommended by medical practitioners, a screening program must meet a number of criteria (https://www.radiologyinfo.org/en/info/safety-hiw_05) , including reducing the number of deaths from the given disease. Screening tests may include lab tests that check blood and other fluids, genetic tests that look for inherited genetic markers linked to disease, and imaging exams that produce pictures of the inside of the body. These tests are typically available to the general population. However, an individual's needs for a specific screening test are based on factors such as age, gender, and family history. In lung cancer screening, individuals who have a high risk of developing lung cancer but no signs or symptoms of the disease undergo low-dose computed tomography (LDCT) scanning of the chest. LDCT combines special x-ray equipment with sophisticated computers to produce multiple, cross-sectional images or pictures of the inside of the body. LDCT produces images of sufficient quality to detect many abnormalities while using up to 90 percent less ionizing radiation than a conventional chest CT (https://www.radiologyinfo.org/en/info/chestct) scan. In the past, doctors used chest x-ray (https://www.radiologyinfo.org/en/info/chestrad) and sputum cytology to check for lung cancer. A chest x-ray makes images of the heart, lungs, airways, blood vessels and the bones of the spine and chest. -

Lung Anatomy
Lung anatomy Breathing Breathing is an automatic and usually subconscious process which is controlled by the brain. The brain will determine how much oxygen we require and how fast we need to breathe in order to supply our vital organs (brain, heart, kidneys, liver, stomach and bowel), as well as our muscles and joints, with enough oxygen to carry out our normal daily activities. In order for breathing to be effective we need to use our lungs, breathing muscles and blood system efficiently. This leaflet should help you to better understand the process of breathing and how we get the much needed oxygen into our bodies. The lungs You have two lungs, one in the right side and one in the left side of your chest. The right lung is bigger than the left due to the position of the heart (which is positioned in the left side of the chest). Source: Pulmonary Rehabilitation Reference No: 66354-1 Issue date: 13/2/20 Review date: 13/2/23 Page 1 of 5 Both lungs are covered by 2 thin layers of tissue called the pleura. The pleura stop the surface of the lungs rubbing together as we breathe in and out. The lungs are protected by the ribcage. The airways Within the lungs there is a vast network of airways (tubes) which help to transport the oxygen into the lungs and the carbon dioxide out. These tubes branch into smaller and smaller tubes the further they go into the lungs. Page 2 of 5 Trachea (windpipe): This tube connects your nose and mouth to your lungs. -

Screening for Lung Cancer: Systematic Review and Meta-Analyses
Screening for Lung Cancer: Systematic Review and Meta-analyses Final Submission: March 31, 2015 McMaster Evidence Review and Synthesis Centre Team: Leslea Peirson, Muhammad Usman Ali, Rachel Warren, Meghan Kenny Maureen Rice, Donna Fitzpatrick-Lewis, Diana Sherifali, Parminder Raina McMaster University, Hamilton Ontario Canada Evidence Review Clinical Expert: Dr. John Miller Canadian Task Force on Preventive Health Care Working Group: Gabriela Lewin (Chair), Maria Bacchus, Neil Bell, Jim Dickinson, Harminder Singh Public Health Agency of Canada Scientific Research Managers: Lesley Dunfield and Alejandra Jaramillo Garcia 1 Abstract Background: This report was produced for the Canadian Task Force on Preventive Health Care (CTFPHC) to inform the development of guidelines on the screening of adults for lung cancer. The last CTFPHC guideline on this topic was published in 2003. Purpose: To synthesize evidence on the benefits and harms of screening asymptomatic adults who are at average and high risk for lung cancer. Data Sources: For benefits of screening we searched CENTRAL, Ovid MEDLINE(R) In- Process & Other Non-Indexed Citations and Ovid MEDLINE(R), and Embase from May 2012 to May 13, 2014 to update the search conducted for the Cochrane 2013 review on this same topic. The same databases were searched to look at harms of screening but the date range was extended to 2000. We also searched for evidence to answer the contextual questions (Embase and MEDLINE; 2009-June 2014), checked reference lists of included studies and relevant systematic reviews, and conducted a targeted grey literature search. Study Selection: The titles and abstracts of papers considered for the key questions and sub- questions were reviewed in duplicate; any article marked for inclusion by either team member went on to full text screening. -

Lung Microbiome Participation in Local Immune Response Regulation in Respiratory Diseases
microorganisms Review Lung Microbiome Participation in Local Immune Response Regulation in Respiratory Diseases Juan Alberto Lira-Lucio 1 , Ramcés Falfán-Valencia 1 , Alejandra Ramírez-Venegas 2, Ivette Buendía-Roldán 3 , Jorge Rojas-Serrano 4 , Mayra Mejía 4 and Gloria Pérez-Rubio 1,* 1 HLA Laboratory, Instituto Nacional de Enfermedades Respiratorias Ismael Cosío Villegas, Mexico City 14080, Mexico; [email protected] (J.A.L.-L.); [email protected] (R.F.-V.) 2 Tobacco Smoking and COPD Research Department, Instituto Nacional de Enfermedades Respiratorias Ismael Cosío Villegas, Mexico City 14080, Mexico; [email protected] 3 Translational Research Laboratory on Aging and Pulmonary Fibrosis, Instituto Nacional de Enfermedades Respiratorias Ismael Cosío Villegas, Mexico City 14080, Mexico; [email protected] 4 Interstitial Lung Disease and Rheumatology Unit, Instituto Nacional de Enfermedades Respiratorias Ismael Cosío Villegas, Mexico City 14080, Mexico; [email protected] (J.R.-S.); [email protected] (M.M.) * Correspondence: [email protected]; Tel.: +52-55-5487-1700 (ext. 5152) Received: 11 June 2020; Accepted: 7 July 2020; Published: 16 July 2020 Abstract: The lung microbiome composition has critical implications in the regulation of innate and adaptive immune responses. Next-generation sequencing techniques have revolutionized the understanding of pulmonary physiology and pathology. Currently, it is clear that the lung is not a sterile place; therefore, the investigation of the participation of the pulmonary microbiome in the presentation, severity, and prognosis of multiple pathologies, such as asthma, chronic obstructive pulmonary disease, and interstitial lung diseases, contributes to a better understanding of the pathophysiology. Dysregulation of microbiota components in the microbiome–host interaction is associated with multiple lung pathologies, severity, and prognosis, making microbiome study a useful tool for the identification of potential therapeutic strategies. -

CT Screening for Lung Cancer in Heavy Smokers Policy Number: PG0049 ADVANTAGE | ELITE | HMO Last Review: 04/01/2021
CT Screening for Lung Cancer in Heavy Smokers Policy Number: PG0049 ADVANTAGE | ELITE | HMO Last Review: 04/01/2021 INDIVIDUAL MARKETPLACE | PROMEDICA MEDICARE PLAN | PPO GUIDELINES This policy does not certify benefits or authorization of benefits, which is designated by each individual policyholder terms, conditions, exclusions and limitations contract. It does not constitute a contract or guarantee regarding coverage or reimbursement/payment. Self-Insured group specific policy will supersede this general policy when group supplementary plan document or individual plan decision directs otherwise. Paramount applies coding edits to all medical claims through coding logic software to evaluate the accuracy and adherence to accepted national standards. This medical policy is solely for guiding medical necessity and explaining correct procedure reporting used to assist in making coverage decisions and administering benefits. SCOPE X Professional X Facility DESCRIPTION In the United States, lung cancer is the most commonly occurring noncutaneous cancer in men and a woman combined, and is the leading cause of cancer deaths. The most important risk factor for lung cancer is tobacco use. Other risk factors are small compared with cigarette smoking—these causal factors include exposures to environmental and occupational substances and family history of lung cancer. Currently, most lung cancer is diagnosed clinically when patients present with symptoms such as persistent cough, pain and weight loss; unfortunately, patients with these symptoms usually have advanced lung cancer. Due to the prevalence and the mortality associated with lung cancer, detecting the disease and initiating treatment at an early stage, in particular, for at-risk individuals is important for improving survival. -

Lung Cancer Screening with Sputum Cytologic Examination, Chest Radiography, and Computed Tomography: an Update for the U.S
Lung Cancer Screening with Sputum Cytologic Examination, Chest Radiography, and Computed Tomography: An Update for the U.S. Preventive Services Task Force Linda L. Humphrey, MD, MPH; Steven Teutsch, MD, MPH; Mark S. Johnson, MD, MPH Screening for lung cancer is not currently increasing in epidemic proportions,3,4 with an recommended by any major medical professional estimated 1 million deaths in the year 2000.5 organization. The U.S. Preventive Services Task Although there are other important risk factors Force (USPSTF) gave lung cancer screening a “D” for lung cancer,3,6–10 cigarette smoking is the major recommendation in both 1985 and 1996, meaning risk factor; approximately 87% of all lung, that there were fair-quality data to recommend bronchial, and tracheal cancer are attributed to against screening for lung cancer1 based largely on 3 smoking.3 Consequently, the most important public negative trials conducted in the United States in the health intervention that could reduce lung cancer 1970s. Since the last Task Force review, several new incidence and deaths is changing smoking habits. studies of lung cancer screening have been reported, Unfortunately, although overall prevalence rates of and greater attention has been directed toward the smoking in the United States have decreased over limitations of existing literature. This review was the past 2 decades, the prevalence of current adult conducted to aid the current USPSTF in updating smokers remains high at 24%.10,11 In the clinical its lung cancer screening recommendation. setting, -

Manatee Anatomy and Physiology
Manatee Anatomy and Physiology Grade level: Elementary 5 Subject Area: Biology, Anatomy and Physiology, Marine Biology Duration: Teach: 15 minutes, Activity: 20 minutes, Discussion: 20 minutes. Setting: Classroom Next Generation Sunshine State Standards: Reading: LAFS.5.RI Reading standards for Information text Cluster 3 LAFS.5.RI.3 Writing: LA.B.2.1, LA.B.1.2 Speaking and Listening: Cluster 2 LAFS.5.SL.Z Presentation of Knowledge and Ideas Science: Body of Knowledge Life Science: SC.5.L.14, SC.5.L.15, SC.5.L.17, Body of Knowledge Nature of Science Supporting Idea 1: SC.5.N.1 Practice of Science, Supporting Idea 2:SC.5.N.2 Characteristics of Scientific Knowledge Earth Systems and Patterns: 7SC.E.E.7 Statewide Science Assessment Prompt: How might humans help manatees survive? Objectives: Students will learn about manatee bodies and explain some anatomical and physiological differences between manatees, humans and other animals. Materials: Handouts of basic manatee anatomy, dolphin anatomy & human anatomy, crayons or markers, coloring direction sheet, question worksheet, Quiz sheet Vocabulary: Mammal, endangered species, habitat, conservation, vibrissae, nares, blowhole, flipper, herbivore, omnivore, carnivore. Background/Preparation: Handouts of manatee, dolphin, and human anatomy. Fact sheets comparing and contrasting specific and unique anatomical aspects of each species. Basic manatee fact sheet highlighting personality, limited habitat, endangered status and conservation efforts. Teachers can review the manatee fact sheets, and select points of interest they would most like to incorporate into a lesson. This activity may fit best into the week where the human anatomy lessons are addressed. Teachers can present the information via traditional lecture, group discussion, question and answer session, or doing the coloring activity as the lesson points are addressed, etc. -

The Fifth Pulmonary Vein
CASE REPORT Anatomy Journal of Africa. 2016. Vol 5 (2): 704 - 706 The Fifth Pulmonary vein Hilkiah Kinfemichael, Asrat Dawit Correspondence to Hilkiah Kinfemichael, Myungsung Medical College, Addis Ababa, Ethiopia PO Box 14972 Email : [email protected]. ABSTRACT A cadaver in Myungsung Medical College (MMC) had a 3rd pulmonary vein originating from the middle lobe of the right lung. Such anatomical variations are very rare. People with this variation have a total of five pulmonary veins entering left atrium. It has clinical implications especially for thoracic surgeons and radiologists during radiofrequency ablations, lobectomies, valve replacements, pulmonary vein catheterizations, video-assisted thoracic surgery (VATS) and others. Key Words: Anatomy, Variations, Pulmonary veins. INTRODUCTION Two pulmonary veins usually drain oxygenated upper lobe, is formed by the union of blood from each lung to left atrium of the apicoposterior, anterior and lingular veins. The heart. The lobular tributaries lie mainly in the inferior left pulmonary vein, which drains the interlobular septa and two pulmonary veins lower lobe, is formed by the hilar union of two from each lung enter left atrium through two veins, superior and common basal veins. The separate pulmonary ostia on either side. On the right and left pulmonary veins perforate the right lung veins from the apical, anterior and fibrous pericardium and open separately in the posterior part of upper lobe unite with a middle posterosuperior aspect of the left atrium lobar vein, which is formed by lateral and (Standring et al., 2008). This anatomy could medial tributaries, and form the superior right show variations, with more veins draining pulmonary vein (Standring, 2008). -
The Respiratory System
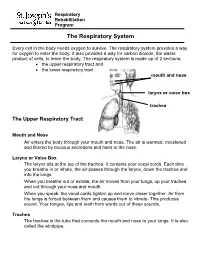
Respiratory Rehabilitation Program The Respiratory System Every cell in the body needs oxygen to survive. The respiratory system provides a way for oxygen to enter the body. It also provides a way for carbon dioxide, the waste product of cells, to leave the body. The respiratory system is made up of 2 sections: the upper respiratory tract and the lower respiratory tract mouth and nose larynx or voice box trachea The Upper Respiratory Tract Mouth and Nose Air enters the body through your mouth and nose. The air is warmed, moistened and filtered by mucous secretions and hairs in the nose. Larynx or Voice Box The larynx sits at the top of the trachea. It contains your vocal cords. Each time you breathe in or inhale, the air passes through the larynx, down the trachea and into the lungs. When you breathe out or exhale, the air moves from your lungs, up your trachea and out through your nose and mouth. When you speak, the vocal cords tighten up and move closer together. Air from the lungs is forced between them and causes them to vibrate. This produces sound. Your tongue, lips and teeth form words out of these sounds. Trachea The trachea is the tube that connects the mouth and nose to your lungs. It is also called the windpipe. The Lower Respiratory Tract Inside Lungs Outside Lungs bronchial tubes alveoli diaphragm (muscle) Bronchial Tubes The trachea splits into 2 bronchial tubes in your lungs. These are called the left bronchus and right bronchus. The bronchus tubes keep branching off into smaller and smaller tubes called bronchi. -

Lung Lobe Segmentation Based on Lung Fissure Surface Classification
algorithms Article Lung Lobe Segmentation Based on Lung Fissure Surface Classification Using a Point Cloud Region Growing Approach Xin Chen 1, Hong Zhao 2 and Ping Zhou 3,* 1 College of Electrical and Information Engineering, Hunan University, Changsha 410082, China; [email protected] 2 College of Aerospace Science and Engineering, National University of Defense Technology, Changsha 410003, China; [email protected] 3 College of Biology, Hunan University, Changsha 410082, China * Correspondence: [email protected] Received: 2 September 2020; Accepted: 13 October 2020; Published: 15 October 2020 Abstract: In anatomy, the lung can be divided by lung fissures into several pulmonary lobe units with specific functions. Identifying the lung lobes and the distribution of various diseases among different lung lobes from CT images is important for disease diagnosis and tracking after recovery. In order to solve the problems of low tubular structure segmentation accuracy and long algorithm time in segmenting lung lobes based on lung anatomical structure information, we propose a segmentation algorithm based on lung fissure surface classification using a point cloud region growing approach. We cluster the pulmonary fissures, transformed into point cloud data, according to the differences in the pulmonary fissure surface normal vector and curvature estimated by principal component analysis. Then, a multistage spline surface fitting method is used to fill and expand the lung fissure surface to realize the lung lobe segmentation. The proposed approach was qualitatively and quantitatively evaluated on a public dataset from Lobe and Lung Analysis 2011 (LOLA11), and obtained an overall score of 0.84. Although our approach achieved a slightly lower overall score compared to the deep learning based methods (LobeNet_V2 and V-net), the inter-lobe boundaries from our approach were more accurate for the CT images with visible lung fissures. -

Clay Adams Anatomical Model
3D Educational Resources LEARN ABOUT THE HUMAN BODY! The human body is an amazing living machine. It contains complex organs that perform all sorts of functions that work together to keep us alive. Find out more about how they do this in a series of fun mini-activities and demonstrations. ONTARIO CURRICULUM LINKS Through this activity, you and your students will use an anatomical model to go through a series of mini-activities and demonstrations about our body’s organs. This activity can be connected to multiple aspects of the school curriculum, our suggested link is: Grade 5: Science (Human Organ Systems) MATERIALS Grades 1 measuring cup 1 3D printout of the anatomical 5 – 9 1 tablespoon (15 mL) model or 3D files of the anatomical 2 bowls (around 1 L model and each) software* to view the files Ag e Range 1 ruler 1.65 m yarn 8 – 14 years 1 measuring tape 900 mL water 750 mL vinegar * Note: There are many free programs available to view the 3D files. Some examples include Sketchup Make (https://www.sketchup.com/download/all) and 3D Builder, which is included with Windows 10. IngeniumCanada.org INSTRUCTIONS These activities can be done either with a 3D printed anatomical model or through viewing the 3D model with a computer program. Feel free to add your own contributions and explore parts of the model not covered in this document. Assembling the Anatomical Model If you are having trouble putting together the anatomical model, you can find below a series of diagrams that should help you out.